We report a sternum-based single-port robotic thymectomy performed using the Da Vinci Xi multi-port robotic system, without the need for an intercostal approach. A vertical incision of 4 cm is made 1 cm below the xiphoid process. An AIRSEAL ROBOTIC SOLUTION gas sealing system compatible with the Da Vinci ports is used to insufflate carbon dioxide at a pressure of 8 mmHg..When inserting the ports, the left and right hands are crossed into the wound, with the camera, left hand, and right hand inserted in order from the anterior chest to the posterior side. To reduce interference between the ports, a key technique is to pull the camera port forward to prevent it from colliding with other ports. The sternum-based single-port robotic thymectomy performed using the Da Vinci Xi system is a technique that combines excellent surgical visibility from the sternum, minimally invasive nature, and enhanced operability provided by the robotic system.
Introduction
Endoscopic thymectomy is typically performed through the lateral intercostal space, but there have been recent reports of a sternum-based approach. The advantage of the sternum-based approach is that the camera is inserted from the midline of the body, making it easier to observe both sides of the phrenic nerve and the upper pole of the thymus. Furthermore, the sternum-based single-port thymectomy requires only a single incision of no more than 4 cm in the subxiphoid area, thus avoiding the intercostal space, resulting in minimal pain and no chronic pain or numbness due to intercostal nerve injury..The sternum-based robotic thymectomy (SRT) involves inserting the camera through the subxiphoid incision and the robotic arms through the lateral intercostal space. This method combines the excellent visibility from the sternum with the ease of operation of the robotic system, allowing for complex procedures such as vascular anastomosis. Here, we report a sternum-based single-port robotic thymectomy (SURT) performed using the Da Vinci Xi multi-port robotic system (Intuitive Surgical, Sunnyvale, California, USA) without the need for an intercostal approach.
Surgical Technique
The patient is placed in a supine position with arms and legs separated. A vertical incision of 4 cm is made 1 cm from the xiphoid process. A Lapsingle port (Sejong Medical Co., Paju, South Korea) with a 12 mm sub-port and three connected 8 mm sub-ports is used. This port is transparent, allowing for wound observation, and is very useful when the Da Vinci port is placed transversely within the wound; three 8 mm ports were used. An AIRSEAL ROBOTIC SOLUTION (ConMed, Utica, New York, USA) compatible with the Da Vinci ports is used to insufflate carbon dioxide at a pressure of 8 mmHg..During port insertion, the left and right hands are crossed into the wound, with the camera, left hand, and right hand inserted in order from the anterior chest to the back. To reduce interference between the ports, a key technique is to pull the camera port forward to prevent it from colliding with other ports (Figure 1). Additionally, to ensure proper crossing of the left and right instruments, adjustments to the hand control settings on the console are required to switch the allocation of left and right hands. We start with a 0° camera angle, adjusting to 30° when the camera interferes with the working area or the field of view is obstructed. The assistant supports the surgeon by inserting a 32 cm Schwarz curved swab (B. BRAUN, Tokyo, Japan) and a 32 cm curved suction through the small gap of the three port wounds (Video 1). The camera view from below the xiphoid may pose challenges for visualizing the left pericardium; however, there are no restrictions on arm movements. Between February and December 2024, we studied five consecutive cases of anterior mediastinal tumors, all of which were confirmed preoperatively to not invade other organs. All five cases underwent total thymectomy, including resection of the upper pole of the thymus. No cases required additional infusion ports. The arms may contact the abdomen, but without excessive pressure, and no complications were reported. In mediastinal surgery, we remove the drainage tubes in the operating room to allow for early patient mobilization. However, if lung resection is performed simultaneously, we retain the drainage tubes due to the risk of air leaks leading to bilateral pneumothorax. All drainage tubes were removed outside the operating room. The median surgical time was 117 (105-178) minutes; the median console time was 75 (33-118) minutes, and the median blood loss was 5 (0-5) ml. No complications or deaths were reported. Postoperative pathology indicated two cases of thymoma and three cases of thymic cysts. All patients had a resting state score of 0 on the numeric rating scale at their first outpatient follow-up after discharge [median, 10 days (6-12 days)].
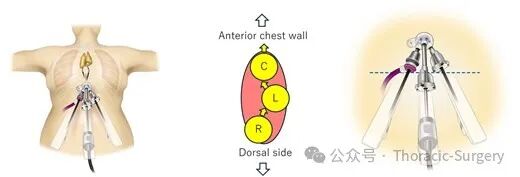
Figure 1: The left and right ports cross within the wound. The camera port is adjusted to a position that does not interfere with the left and right ports.
Video 1 (https://academic.oup.com/ejcts/article/67/4/ezaf127/8114636): Sternum-Based Single-Port Robotic Thymectomy. In this case, the camera is primarily set at a 0° direct view angle.
Discussion
The SURT technique presented in this report combines the minimally invasive nature of sternum-based single-port thymectomy with the superior operability of SRT. Although sternum-based single-port thymectomy offers significant benefits to patients, it has not been widely adopted by surgeons due to the complexity of the procedure. SURT allows for thymectomy using a highly operable robotic system through a single subxiphoid incision, potentially enabling more complex surgeries. In recent years, the da Vinci SP system designed specifically for single-port surgery has been launched, with reports of its application in thymectomy. However, the single-port system is expensive and has limited operational capabilities, leading to low adoption rates in medical institutions. Additionally, using flexible endoscopic cameras to clearly visualize the narrow neck area remains challenging. This surgical technique allows for minimally invasive sternum-based single-port thymectomy without the expensive robotic systems of single-port systems, and pain is almost completely alleviated within 1-2 weeks post-surgery. However, challenges include the lack of retraction arms, requiring assistants to use long, curved swabs or suction devices to open the surgical area through the narrow wound. Furthermore, the camera may sometimes interfere with the left and right hands, limiting operations. To avoid interference, it is crucial to position the left and right hands in the center of the screen when adjusting the camera viewpoint. If bleeding occurs, first apply pressure to the bleeding point with cotton or the thymus. Once temporary hemostasis is achieved, a 12 mm port with a valve is placed in the right fifth intercostal space along the anterior axillary line to enhance operability and further support. TachoSil® (Takeda Austria GmbH, Linz, Austria) can be used to suture or seal the bleeding point. If hemostasis is difficult, a supine surgical position may be adopted for a rapid transition to median sternotomy. Incising the mediastinal pleura on both sides may pose risks of tumor dissemination to the same side and contralateral side, as well as adhesions with the lungs. However, in the 108 sternum-based thymectomies performed at our institution over the past 10 years, only two cases of ipsilateral dissemination were observed, with no contralateral dissemination noted. Nevertheless, long-term outcomes still need to be evaluated.
The key to initiating this operation is to always maintain the initial position of the ports. Adjust the camera arm to a position that does not interfere with the camera port head. If the camera arm interferes with the operation, ensure that the internal position of the port is consistent with the initial settings. The right hand used a SynchroSeal anatomical forceps. This forceps can perform dissection, sealing, and separation without changing instruments, making it very suitable for this operation. If the assistant can insert long, curved swabs or forceps through the narrow port gaps to support the surgeon, this operation can be simplified.
Using the Da Vinci Xi for SURT is a technique that combines excellent surgical visibility from the sternum, minimally invasive nature, and enhanced operability provided by the robotic system.