
The standard treatment (SoC) for surgically resectable early-stage (I-IIIB) NSCLC patients is surgery combined with (new) adjuvant systemic therapy for patients with stage II to IIIB and certain stage IB patients, with chemotherapy and radiotherapy used in select cases (for stage III disease with mediastinal lymph node metastasis). Despite these treatments, metastatic recurrence is common and associated with poor survival outcomes, highlighting the need for more effective systemic therapies than the current SoC. Following the successful treatment of advanced NSCLC patients with oncogenic driver mutations using targeted therapy (TT), these drugs are being explored for perioperative (neoadjuvant and adjuvant) treatment in early NSCLC patients. Osimertinib is the only TT approved for adjuvant treatment in early patients, and currently, no neoadjuvant TTs are approved. This article discusses the importance of comprehensive biomarker testing at diagnosis to identify patients who may benefit from neoadjuvant targeted therapy and summarizes new data from neoadjuvant TT trials. Additionally, it addresses the potential challenges of establishing neoadjuvant TT as the SoC in early patients, including the identification and validation of early response biomarkers to guide treatment and accelerate drug development, as well as safety considerations in perioperative treatment. Preliminary data indicate that neoadjuvant TT is effective and well-tolerated in patients with early NSCLC who are positive for EGFR or ALK. Ongoing trial data will determine whether neoadjuvant targeted therapy can become a new SoC for resectable NSCLC patients with oncogenic addiction.
Background
Approximately half of NSCLC patients are diagnosed at an early stage, and this number is expected to increase with the expansion of high-risk population screening programs. Surgery is the primary curative treatment option for resectable NSCLC (I-IIIB) patients, with neoadjuvant or adjuvant systemic therapy recommended for stage II to IIIB patients and selected stage IB patients, or chemotherapy and radiotherapy in very few cases for stage III patients with mediastinal lymph node metastasis. Despite available treatments, disease recurrence is common among patients undergoing resection, associated with poor survival outcomes and socioeconomic burdens. A meta-analysis of five adjuvant chemotherapy trials in resected NSCLC patients showed a 5-year overall survival (OS) increase of 5.4% compared to surgery alone. Similarly, in a meta-analysis of neoadjuvant chemotherapy in resectable NSCLC patients, a 5-year OS increase of 5% was observed compared to surgery alone. Therefore, additional treatments are needed to reduce disease recurrence, prolong survival for early NSCLC (eNSCLC) patients, and improve cure rates. Recent advances in eNSCLC treatment include the approval of various adjuvant treatment regimens, including osimertinib for surgically resected NSCLC patients with classic EGFR mutations (IB-III), atezolizumab for NSCLC patients after surgical resection and platinum-based chemotherapy (II-III), with tumor programmed death ligand-1 (PD-L1) expression based on national-specific thresholds; and pembrolizumab for NSCLC patients after surgical resection ± platinum-based chemotherapy (IB [T2a ≥ 4 cm], II, or IIIA; TNM cancer staging system, 7th edition). Ongoing studies may lead to the approval of additional adjuvant targeted therapies (TT), including the exploration of alectinib in the ALINA trial for adjuvant treatment in ALK-positive surgically resected NSCLC patients. With the recent approval of neoadjuvant nivolumab combined with platinum-based doublet chemotherapy for resectable NSCLC patients, the field of neoadjuvant treatment is rapidly evolving. Currently, no neoadjuvant TTs are approved for resectable NSCLC.
For advanced NSCLC (aNSCLC) patients, the standard treatment (SoC) includes comprehensive biomarker testing, assessing PD-L1 status, and the presence of oncogenic driver mutations (including various EGFR mutations, ALK, RET, NTRK, ROS1, KRAS G12C, BRAF V600E, METex14 skipping, ERBB2). The recommended first-line treatment for oncogene-addicted aNSCLC is TT, with TT recommended as second-line treatment except for patients with KRAS G12C mutations, ERBB2 mutations, or EGFR exon 20 insertions. Clinical evidence suggests that EGFR mutation or ALK-positive advanced NSCLC patients benefit little or not at all from cancer immunotherapy (CIT), and combining CIT with TT does not provide additional benefits. Importantly, among patients with advanced disease, TT combined with CIT and sequential therapies are associated with increased toxicity. In early patients, it remains unclear whether CIT is also less effective in patients with EGFR or ALK alterations; ongoing perioperative trials have varying standards for whether to allow enrollment of known EGFR or ALK altered patients and whether pre-enrollment genetic testing is required. Preliminary subgroup analyses of adjuvant CIT trials suggest efficacy in a small subset of patients with EGFR activating mutations; however, these results should be interpreted cautiously, considering the significant OS benefits of osimertinib as adjuvant treatment.
Given these efficacy and safety considerations, as well as the recent approvals of therapies for early patients excluding tumors with EGFR and ALK mutations, it is crucial to conduct oncogenic driver gene mutation testing to guide perioperative treatment decisions. This article discusses the importance of biomarker testing to identify patients who may benefit from neoadjuvant targeted therapy and the potential challenges of establishing perioperative TT as standard treatment. The aim of this review is to provide a comprehensive summary of the existing literature and ongoing clinical trials to evaluate the feasibility, efficacy, and safety of neoadjuvant TT for eNSCLC patients.
Materials and Methods
Table 1 is compiled based on known neoadjuvant treatment clinical trials with published results. Given the limited number of published results from neoadjuvant targeted therapy trials, a systematic review is not appropriate. To identify all ongoing neoadjuvant TT clinical trials for eNSCLC patients, we conducted a systematic search on clinicaltrials.gov using the keywords “neoadjuvant” and “lung cancer.” Trials that were terminated or completed were excluded. Studies were then classified by treatment, excluding trials exploring only CIT or chemotherapy, radiotherapy, or other treatments. The resulting trials were further categorized by monotherapy (Table 2) and TT plus chemotherapy (Table 3). Studies were subjected to final screening, excluding those deemed inappropriate. Full details of the systematic search and exclusion of studies are shown in Figure 1. The systematic search was first completed on June 14, 2022. An additional search was conducted on October 19, 2022, to identify any other studies registered since the first search.
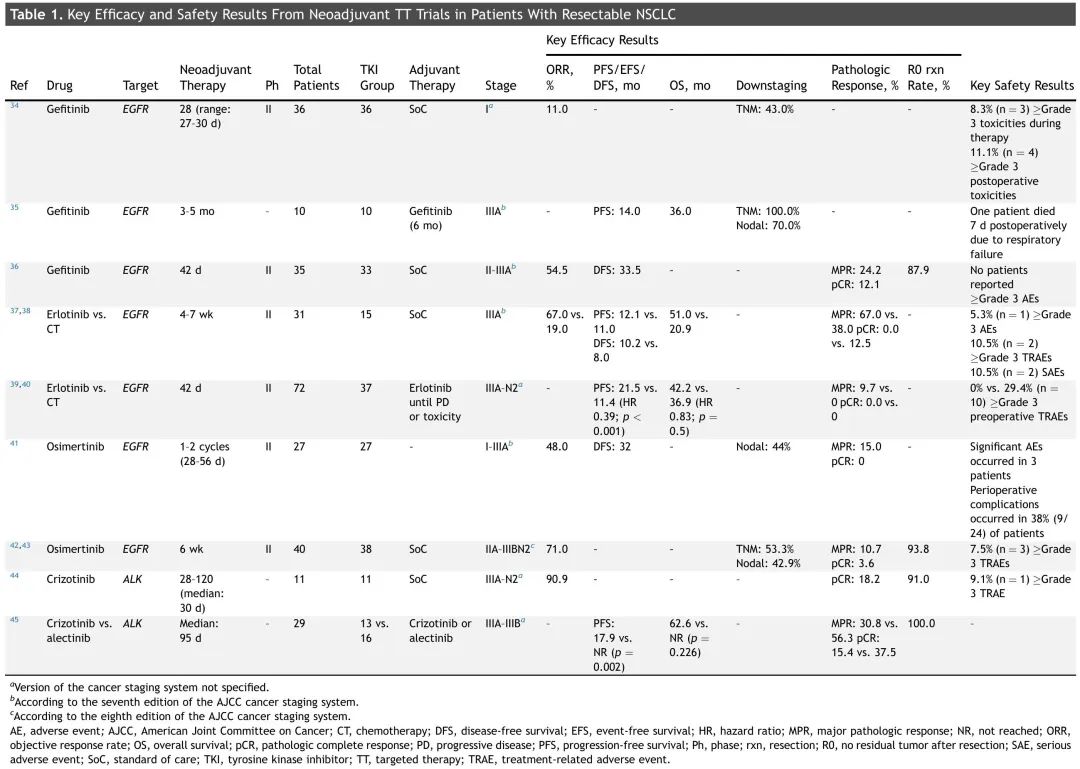
Table 1. Key Efficacy and Safety Results of Neoadjuvant TT Trials in Resectable NSCLC Patients
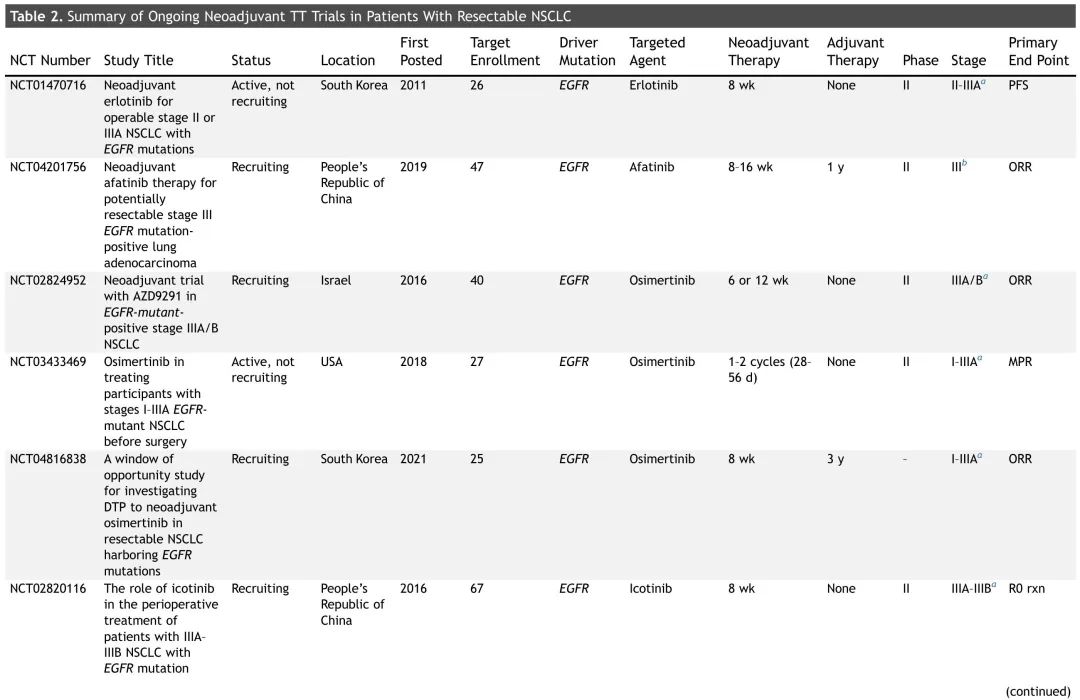
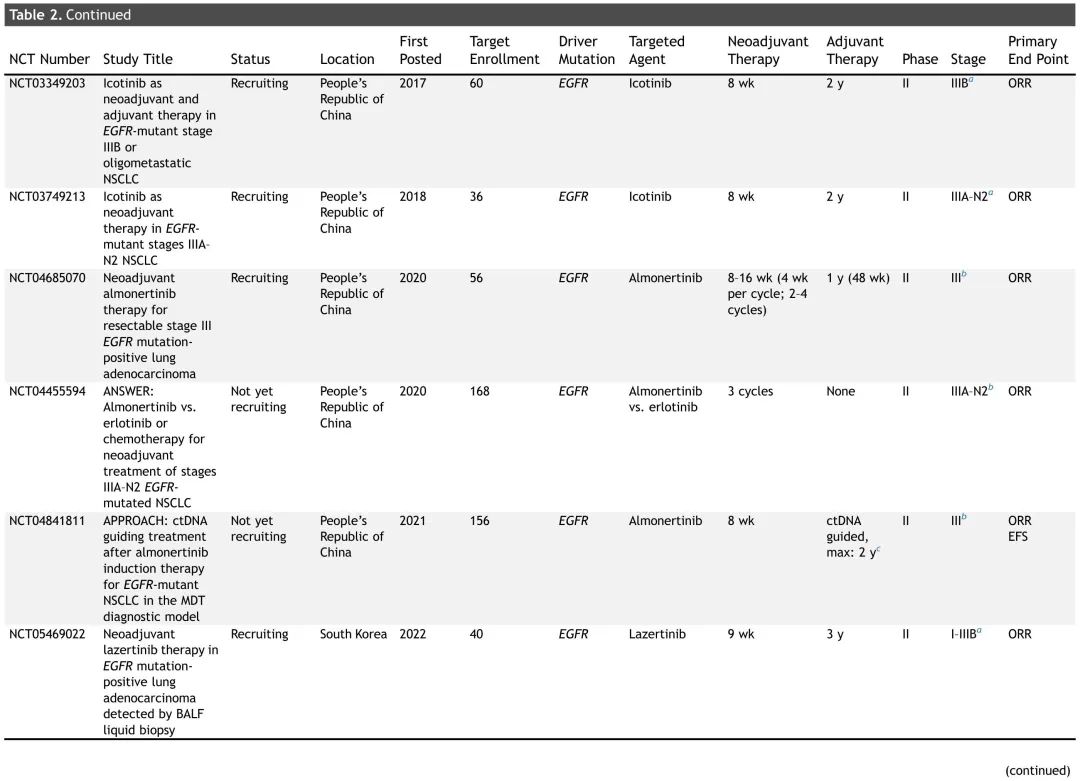
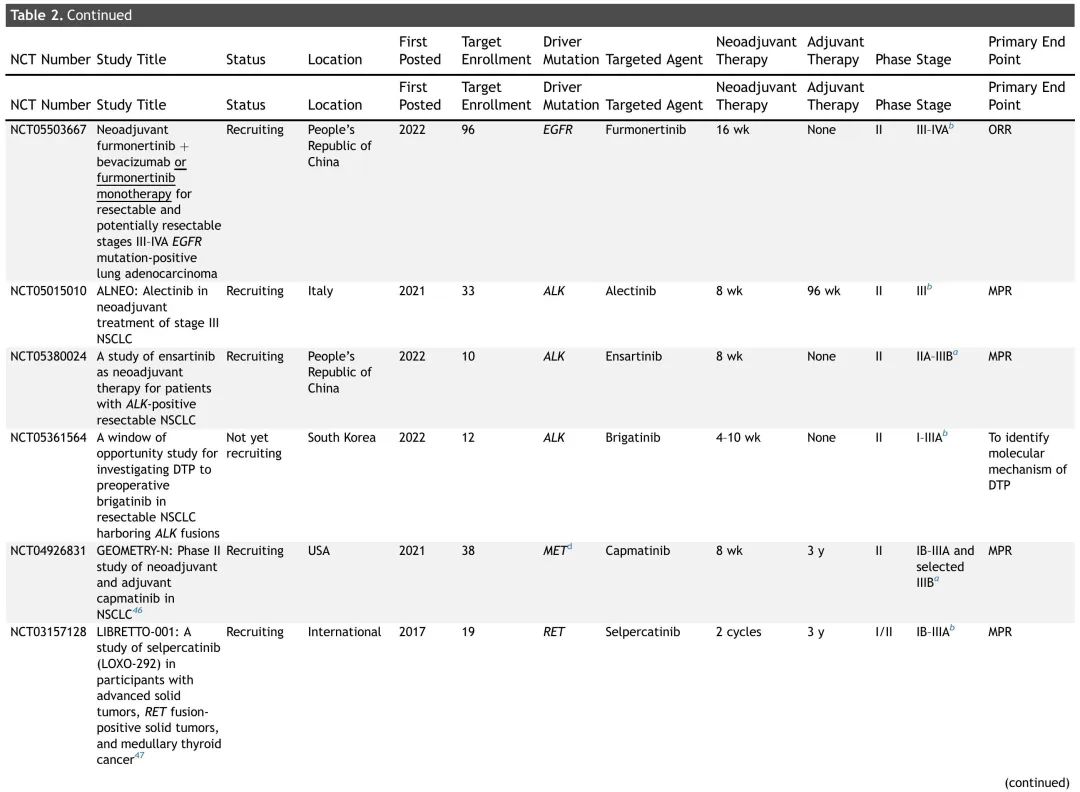
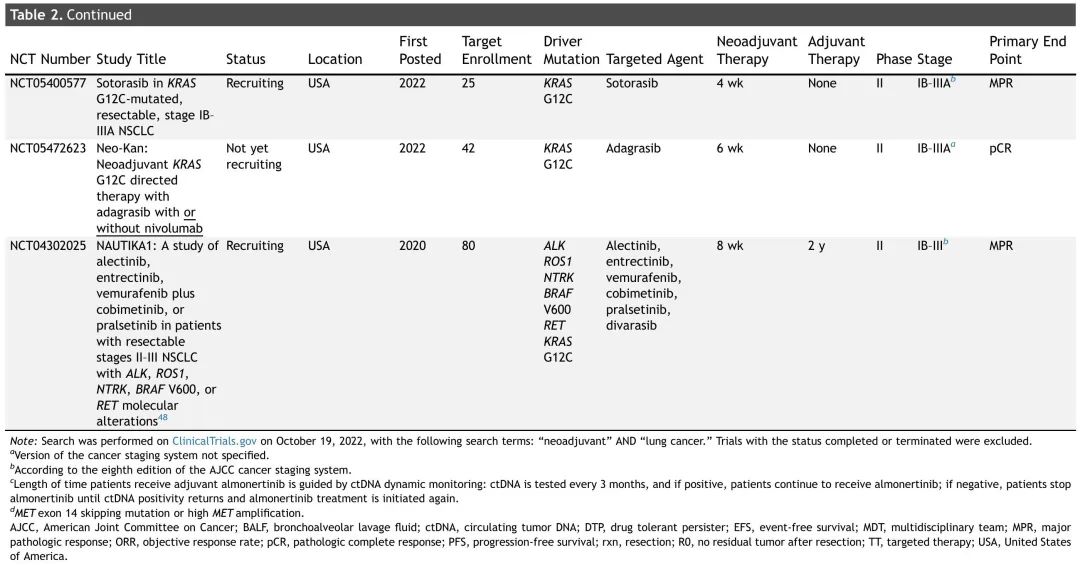
Table 2. Summary of Ongoing Neoadjuvant TT Trials in Resectable NSCLC Patients
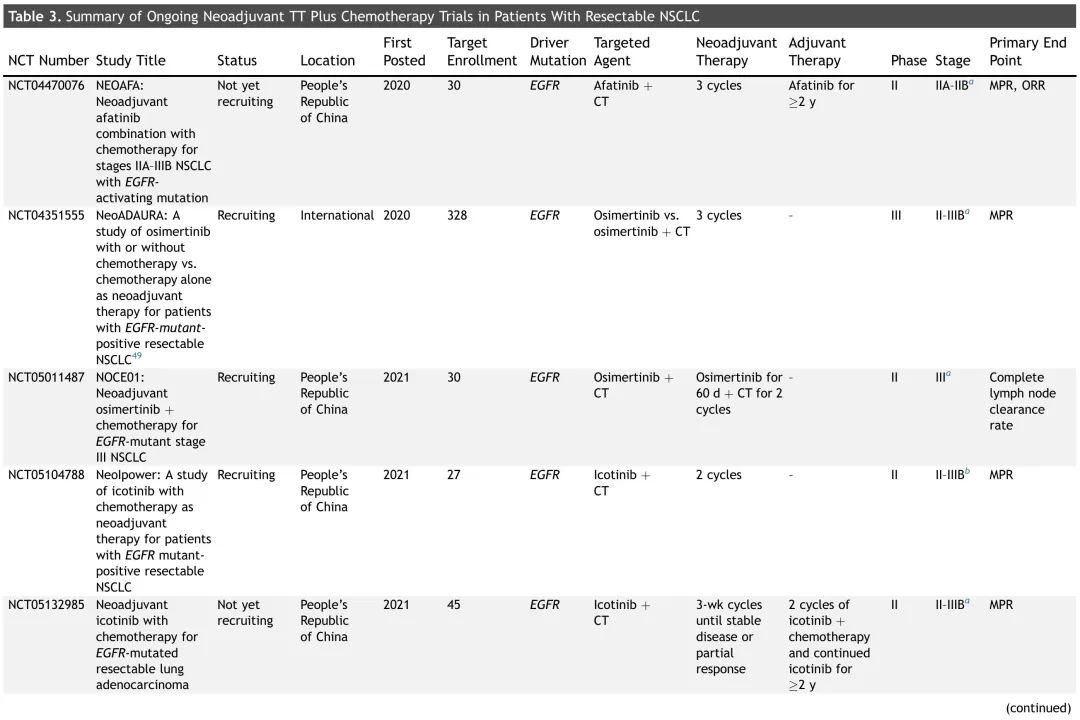
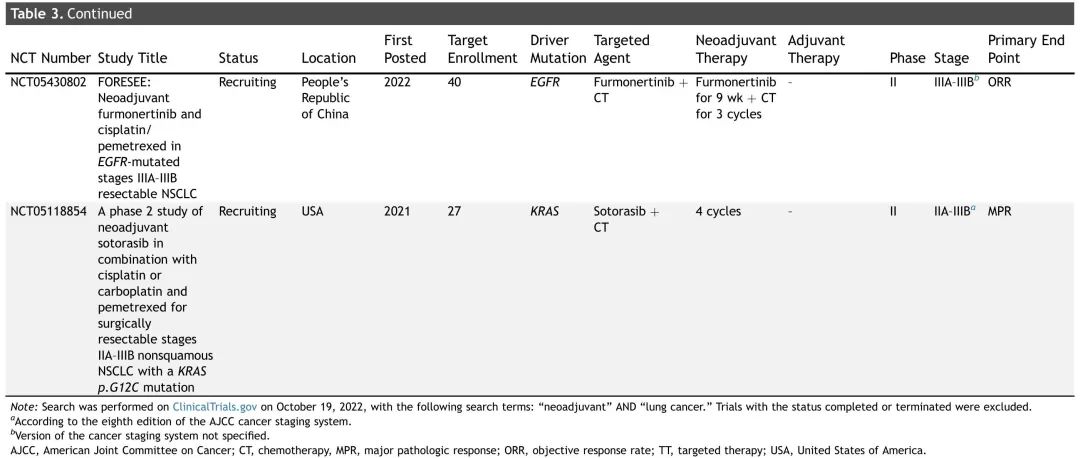
Table 3. Summary of Ongoing Neoadjuvant TT Plus Chemotherapy Trials in Resectable NSCLC Patients
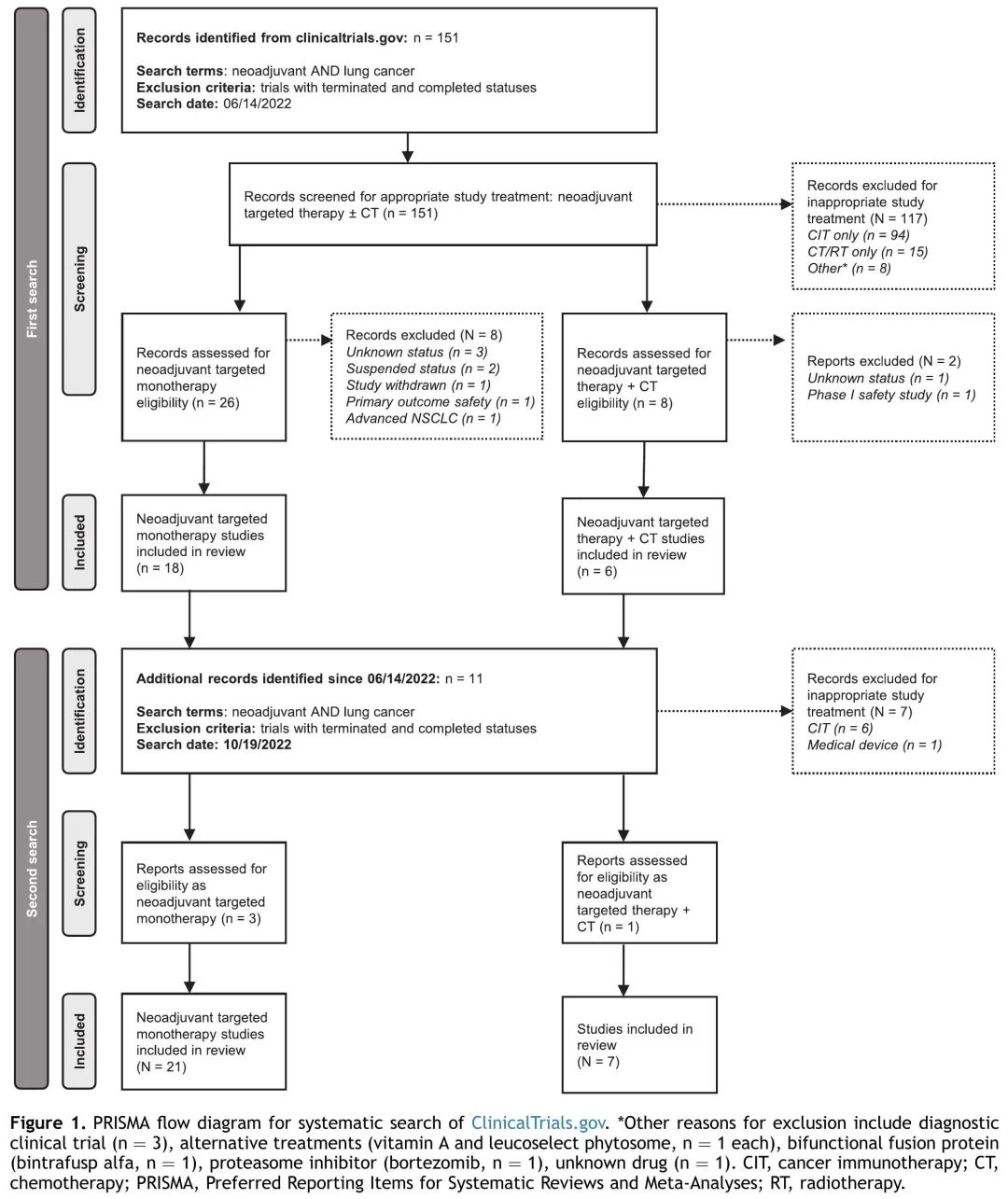
Figure 1. Study Screening Process
Rationale for Neoadjuvant Treatment in eNSCLC
Neoadjuvant treatment for resectable NSCLC has several potential benefits, including: better tolerance of neoadjuvant therapy compared to adjuvant therapy; early systemic treatment can control micrometastatic disease; the required extent of surgical resection may be smaller (lung-preserving surgery), and the rate of complete resection (R0) is higher. Neoadjuvant treatment allows for alternative endpoint assessments of survival estimates (OS, disease-free survival [DFS]), such as clinical, pathological, or relevant biomarker assessments of treatment response. Preoperative therapies also help assess treatment effects in vivo and may guide adjuvant treatment. Another anticipated advantage is that adherence to neoadjuvant treatment is higher than that of adjuvant treatment. A common argument against neoadjuvant treatment is that, although treatment duration is shorter (three to four cycles), it may prolong the time from diagnosis to curative surgery, during which patients may experience disease progression. However, evidence from neoadjuvant CIT trials provides confidence that this will not impact patient prognosis.
Rationale for Biomarker Testing at Diagnosis and the Necessity of Collecting Sufficient Biopsy Samples at Diagnosis
As research explores the role of TT in eNSCLC, biomarker testing is crucial for guiding treatment selection and optimizing clinical outcomes. Following the recent approval of perioperative systemic therapy for eNSCLC patients, the NCCN oncology clinical practice guidelines (NCCN Guidelines) recommend using FDA-approved tests to assess EGFR mutations, ALK rearrangements, and PD-L1 status in stage IB to IIIA and IIIB (T3, N2) NSCLC patients, providing information for (neoadjuvant) treatment decisions. For metastatic NSCLC, the NCCN guidelines recommend molecular testing before starting first-line treatment when clinically feasible. Nevertheless, a real-world study showed that only 46% of metastatic NSCLC patients received assessments for the five recommended biomarkers. This highlights that barriers to molecular testing in advanced disease may also limit testing in early disease, anticipating changes in treatment patterns that will require testing beyond EGFR mutations, ALK rearrangements, and PD-L1 status.
There are several considerations regarding the inclusion of preoperative biomarker testing as part of routine clinical practice at diagnosis to guide neoadjuvant treatment decisions. Minimizing turnaround time for obtaining test results is essential to ensure timely initiation of the correct systemic treatment. Collecting sufficient biopsy samples is imperative for biomarker testing (PD-L1 expression and oncogenic driver mutations), as low yields may render testing unfeasible. In neoadjuvant treatment, therapy may lead to pathological complete response (pCR), making biomarker testing using resected tissue specimens unfeasible, emphasizing the importance of collecting sufficient biopsy tissue at diagnosis.
The accessibility of comprehensive genomic analysis using next-generation sequencing (NGS) is increasing and is widely used for tissue and plasma samples to inform treatment decisions for NSCLC. However, the routine application of NGS in eNSCLC will depend on the accessibility of approved TTs, the need to exclude oncogenic driver mutation patients before CIT treatment, and the availability of clinical studies exploring TT for early disease. In preoperative treatment, blood-based biomarker testing for oncogenic drivers may overcome the inherent limitations of tissue sampling: convenient and minimally invasive, with shorter turnaround times. The BFAST study (NCT03178552) reported clinical benefits for aNSCLC patients receiving TT based solely on blood NGS results. However, due to the lower disease burden in eNSCLC compared to aNSCLC, plasma samples may not contain sufficient circulating tumor DNA (ctDNA) for analysis. Genetic testing of blood samples from eNSCLC patients is highly dependent on the testing methods used, requiring more sensitive technologies to avoid false-negative results. Additionally, blood-based NGS is not routinely performed outside of clinical trials in specialized cancer centers. Finally, the approach of relying solely on liquid biopsies without tissue analysis cannot assess PD-L1 expression.
The LEADER trial (NCT04712877) is a diagnostic study aimed at determining the proportion of early (IA2-III) NSCLC patients with oncogenic driver mutations (Figure 2). If oncogenic driver mutations are found in more than 35% of enrolled patients, the screening approach taken in this trial is considered feasible. Assessment of tumor mutation burden is a secondary endpoint. Approximately 1,000 patients will be recruited using tissue and plasma samples for NGS (FoundationOne). Results will be shared with treating physicians to guide treatment or allow referral to neoadjuvant clinical trials and may provide an ideal framework for assessing actionable biomarkers in neoadjuvant treatment. Plasma samples will be collected before and after neoadjuvant treatment and post-surgery for relevant studies. Evidence from CIT trials CheckMate 816 and IMpower010 indicates that not all patients respond to neoadjuvant or adjuvant CIT, necessitating testing for PD-L1 expression and oncogenic driver mutations, as well as other prognostic factors such as co-mutations to identify patients most likely to benefit from CIT or TT. This underscores the necessity of comprehensive molecular testing using NGS to guide treatment options for resectable NSCLC.
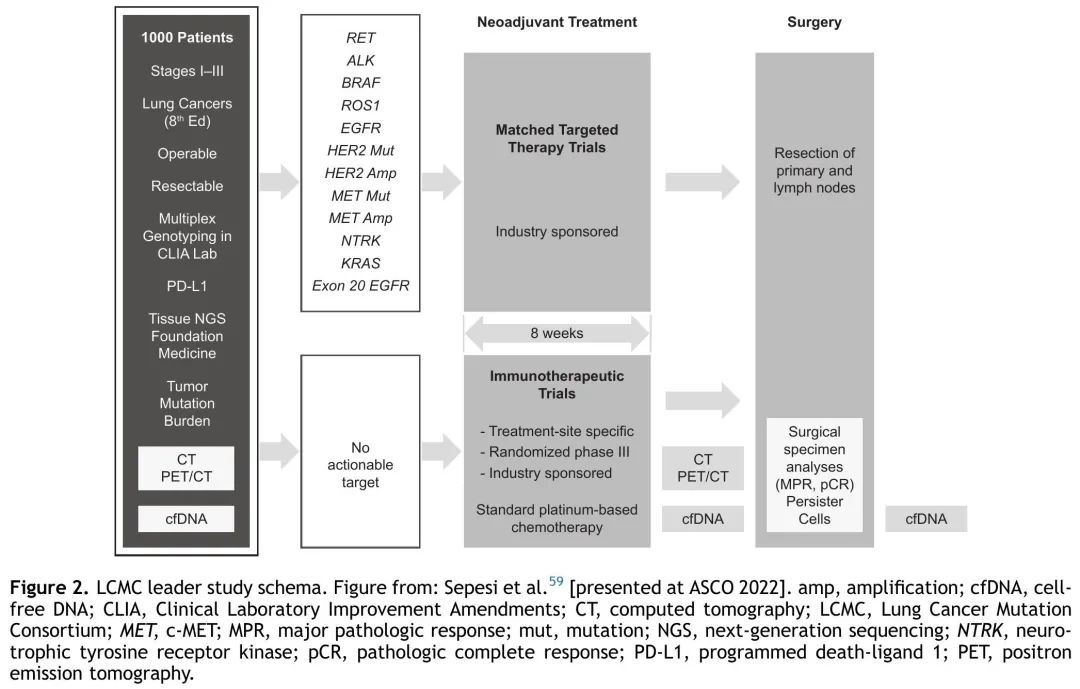
Figure 2. LEADER Trial
Data from Neoadjuvant TT Clinical Trials
Given the success of TT in advanced disease and the impressive survival benefits of osimertinib as adjuvant therapy, neoadjuvant TT is increasingly being explored for oncogene-addicted resectable lung cancer. Most neoadjuvant TT trials utilize EGFR and ALK tyrosine kinase inhibitors (TKIs), which are the most mature TTs in this field (Table 1). Notably, NSCLC patients with EGFR mutations and ALK rearrangements have inherent differences in tumor biology, and different TKIs (including multiple generations) are associated with different resistance mechanisms. Therefore, EGFR and ALK TKIs and their relevant targets have unique distinctions.
Currently, EGFR TKIs such as gefitinib, erlotinib, and osimertinib have been explored for neoadjuvant treatment (Table 1). An open-label, single-arm phase II study (NCT00188617) reported that gefitinib is generally a safe and feasible option in unselected stage I NSCLC patients, with an objective response rate (ORR) of 11%, with the strongest predictor of treatment response being the presence of EGFR mutations. Another single-arm phase II study (NCT01833572) indicated that neoadjuvant gefitinib is a viable treatment option for EGFR-mutated stage II to IIIA NSCLC patients, with an ORR of 54.5%, major pathological response (MPR) of 24.2%, and median DFS of 33.5 months. In a retrospective study, 10 patients with borderline resectable NSCLC underwent salvage surgery after neoadjuvant gefitinib treatment, with a median progression-free survival (PFS) of 14 months and OS ≥ 36 months. Erlotinib has also been reported as an effective neoadjuvant treatment in a phase III study involving Chinese stage IIIA NSCLC patients (NCT01217619): erlotinib’s ORR (67% vs 19%), pathological response rate (67% vs 38%), and OS (51.0 vs 20.9 months) were higher than those of platinum-based doublet chemotherapy. The EMERGING-CTONG 1103 study is a randomized phase II trial comparing the efficacy of neoadjuvant chemotherapy with erlotinib in EGFR-mutated stage IIIA to N2 NSCLC patients. The primary endpoint ORR was not met (erlotinib 54.1%, chemotherapy 34.3%), but median PFS improved (21.5 months vs 11.4 months), although it did not translate into OS benefits. Preliminary results from ongoing osimertinib clinical trials indicate that this third-generation EGFR TKI is generally safe and may be an effective neoadjuvant treatment. In a small phase II study including 27 EGFR-mutated stage I to IIIA NSCLC patients (NCT03433469), neoadjuvant osimertinib induced pathological response (MPR: 15%) and downstaging; however, this study did not meet its primary endpoint. The NEOS study included 38 EGFR-mutated resectable stage II to IIIB NSCLC patients, with final results showing an ORR of 71.1%, R0 resection rate of 93.8%, and MPR of 10.7%.
In ALK-positive resectable locally advanced NSCLC patients, Zhang et al. reported that crizotinib neoadjuvant treatment is feasible and well-tolerated (Table 1). Overall, among 11 patients, 10 had partial responses, and 1 had stable disease. Among these, 10 patients underwent R0 resection, with 2 achieving pCR. A retrospective study involving patients receiving induction therapy with alectinib (n=16) or crizotinib (n=13) found that alectinib was more effective than crizotinib (pCR: 37.5% vs 15.4%). Multiple clinical trials are exploring the efficacy and safety of next-generation ALK inhibitors as neoadjuvant treatments (Table 2).
The exploration of neoadjuvant TT is still in its early stages, and the optimal duration of treatment remains unclear. In the ADAURA study, 41% of patients received osimertinib treatment upon recurrence after at least 3 years of adjuvant therapy, suggesting that some patients may require osimertinib for more than 3 years. The duration of neoadjuvant treatment is limited by the need for surgical resection (limiting the number of TT cycles) and challenges related to efficacy assessment. Additional data from ongoing clinical trials are crucial to determine the optimal duration of neoadjuvant TT.
Preliminary data indicate that the rates of MPR or pCR in neoadjuvant TT trials may be lower compared to neoadjuvant CIT trials, while other efficacy endpoints (R0 resection rate, downstaging, event-free survival [EFS], DFS, PFS) are similar (Table 1). This may be due to inherent differences in mechanisms of action. The antitumor effect of chemotherapy is driven by cytotoxic effects, CIT is driven by enhanced immune surveillance, while TT is immunosuppressive, which may affect the necessary duration of neoadjuvant TT. Until a better understanding of pathological response after neoadjuvant TT is achieved, early patients should still undergo surgical resection, and survival assessment remains an essential endpoint.
Ongoing Neoadjuvant TT Trials
Most ongoing neoadjuvant (or perioperative) trials are investigating TT for EGFR-mutated NSCLC, although trials exploring targeted drugs for other oncogenic driver mutations are also recruiting patients (Table 2). Non-EGFR trial designs are similar, with neoadjuvant treatment lasting two cycles (6-8 weeks), most trials also including adjuvant treatment (1-3 years). The primary endpoints of these trials are diverse, including pathological response (MPR, complete response), ORR, DFS, EFS, and PFS. NAUTIKA1 is an ongoing phase II umbrella trial evaluating various therapies as neoadjuvant treatments in resectable NSCLC patients with specific biomarkers (Figure 3). This clinical trial outlines a potential future management paradigm, where patients with tumors carrying oncogenic driver mutations receive perioperative TT, while non-carriers receive CIT.
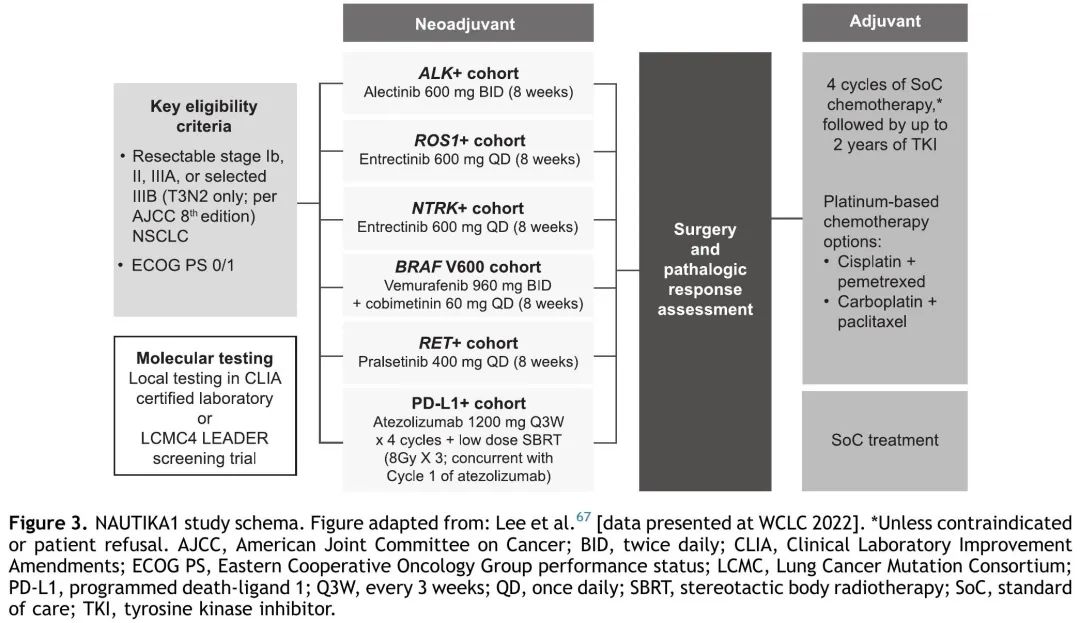
Figure 3. NAUTIKA1 Study
Given that TT is generally well-tolerated, several ongoing neoadjuvant trials are evaluating TT combined with chemotherapy (Table 3). Most are assessing EGFR inhibitors, and a phase II study (NCT05118854) is exploring the efficacy of neoadjuvant KRAS G12C inhibitor sotorasib combined with chemotherapy in KRAS G12C-mutated resectable (IIA-IIIB) NSCLC patients. The results of these trials are highly anticipated and will further clarify whether neoadjuvant TTs (either alone or in combination with chemotherapy) are a viable and effective treatment strategy for NSCLC patients. In future perioperative TT trials, it will be interesting to explore the interactions between KRAS G12C and co-mutations, as well as the efficacy and safety of TT combinations.
Endpoints of Neoadjuvant TT Trials
A range of clinical endpoints can be used to evaluate the efficacy of neoadjuvant treatment in eNSCLC patients. OS is the primary endpoint in oncology clinical trials, but neoadjuvant trials take 10 to 13 years from enrollment to OS data publication, indicating a strong need for robust surrogate markers to accelerate the development and approval of new therapies in early disease. Surrogate biomarkers of drug response are commonly used in other areas of oncology and have been shown to correlate with OS. A meta-analysis of neoadjuvant treatment in early breast cancer showed a close correlation between pCR and long-term survival (EFS and OS). Similarly, in landmark neoadjuvant chemotherapy trials for resectable lung cancer, strong correlations between DFS and OS have been reported. The CheckMate 816 trial included resectable NSCLC patients receiving neoadjuvant nivolumab combined with chemotherapy, and patients achieving pCR appeared to have longer EFS than those who did not achieve it (median EFS: not reached vs 26.6 months). Additionally, a recent study explored response assessments in neoadjuvant NSCLC trials, finding that MPR is a better predictor of long-term OS than ORR. Interestingly, digital pathology response assessment has shown utility in ongoing neoadjuvant CIT trials and may also be useful for assessing similar endpoints in TT trials.
Results from trials of adjuvant TT for resectable NSCLC indicate that surrogate markers (pCR, MPR, EFS, and DFS) may be associated with survival; however, these studies were not designed to evaluate OS, and more data are needed to determine clear associations. The SELECT trial, a single-arm phase II study evaluating adjuvant erlotinib for EGFR-mutated eNSCLC patients, showed high DFS and OS rates: 2-year and 5-year DFS rates were 88% and 56%, respectively, with a 5-year OS of 86%. The phase II EVAN trial evaluated the efficacy of adjuvant erlotinib vs chemotherapy in EGFR-mutated stage III NSCLC patients, finding that erlotinib improved survival outcomes compared to chemotherapy, and DFS was associated with OS: the 5-year DFS and OS rates for the erlotinib group were 48.2% and 84.8%, respectively. Results from the randomized phase III IMPACT study showed that the 2-year DFS rate for gefitinib as adjuvant treatment was higher than that of chemotherapy, but this advantage was lost at 5 years and did not translate into OS benefits. Similarly, in the final analysis of the phase III ADJUVANT-CTONG1104 trial comparing gefitinib vs chemotherapy in EGFR-mutated surgically resected stage I to IIIA NSCLC patients, significant improvements in DFS did not translate into OS benefits. The phase III ADAURA study demonstrated that adjuvant osimertinib significantly improved DFS compared to placebo in stage II to IIIA NSCLC patients: 3-year DFS rates were 84% vs 34%. Osimertinib also resulted in DFS improvement across the overall population (IB-IIIA) and reduced local regional recurrence, distant recurrence, and central nervous system (CNS) recurrence. The FDA approved adjuvant osimertinib for surgically resected NSCLC patients based on DFS data from this study, although OS was immature at the time of approval. Recent data from this trial indicate that osimertinib provides significant, clinically meaningful OS improvements. This is the first instance where DFS benefits have translated into OS improvements for TT, validating DFS as a surrogate marker for OS.
In neoadjuvant treatment, it remains unclear whether surrogate markers in resectable NSCLC TT trials are associated with survival. A phase II study of gefitinib indicated that MPR was associated with DFS but not with OS. A small study comparing erlotinib with chemotherapy showed that erlotinib’s ORR and MPR were slightly superior, which were not associated with improvements in DFS or PFS, but there was a trend towards OS improvement. Results from the EMERGING-CTONG 1103 study indicated that ORR was associated with PFS, but pathological response was not associated with PFS, and the PFS advantage did not translate into OS benefits. However, it should be noted that the OS analyses in these studies were not powered for efficacy.
Preliminary results from neoadjuvant CIT trials indicate that ctDNA assessment has value as an early surrogate marker for response and survival, but more data are needed. The LCMC3 study showed that ctDNA reduction after neoadjuvant treatment with atezolizumab was associated with pathological response and imaging tumor shrinkage. Exploratory analyses of the phase II NADIM study indicated that pre-treatment ctDNA levels correlated with long-term survival more accurately than radiographic assessments in resectable stage IIIA NSCLC patients receiving neoadjuvant nivolumab and chemotherapy. In the CheckMate 816 study, ctDNA clearance was associated with longer EFS in patients receiving both nivolumab combined with chemotherapy and those receiving chemotherapy alone. However, there is currently no data demonstrating the utility of ctDNA as a surrogate marker for response or survival in neoadjuvant TT. ctDNA may also be a useful tool for guiding the duration and downgrading of (neoadjuvant) adjuvant treatment. Evidence supporting the feasibility of this approach is limited and depends on the sensitivity of the assays, while technologies are rapidly evolving. An ongoing related study is the APPROACH study (NCT04841811), which will assess the efficacy and safety of using ctDNA to guide the duration of neoadjuvant treatment with the EGFR TKI amivantamab in unresectable stage III NSCLC (Table 2).
Safety Considerations for Neoadjuvant TT
TT has unique safety considerations, and it is important to consider whether toxicities may occur during neoadjuvant treatment, which could delay or prevent curative surgery. For example, RET inhibitors pralsetinib and selpercatinib have been associated with impaired wound healing, which may affect surgical recovery. A few reports have documented serious respiratory adverse events (AEs) associated with some ALK, EGFR, and MET inhibitors (including pneumonia and interstitial lung disease), which may limit the use of these therapies before surgical resection. Other rare toxicities that may impact surgery include: cardiac toxicity (osimertinib), bradycardia (alectinib and crizotinib), thrombocytopenia (osimertinib), fever (dabrafenib plus trametinib), hepatotoxicity (sotorasib), and central nervous system toxicity (lorlatinib). Preliminary results from the ALK-positive cohort in the NAUTIKA1 study indicate that alectinib neoadjuvant treatment is well-tolerated, with all patients undergoing surgery without delays or serious complications. In addition to surgery, the safety of TT in conjunction with radiotherapy also needs to be considered. The BRIGHTSTAR study indicated that local consolidation treatment (surgery or radiotherapy or both) after treatment with brigatinib in aNSCLC patients is feasible and safe; however, additional data in early patients is needed.
When selecting curative treatment, the sequence of therapies is important, as first CIT followed by TT is associated with increased toxicity in advanced disease. Among patients receiving crizotinib treatment after first CIT (pembrolizumab, nivolumab, or atezolizumab), the risk of hepatotoxicity increases. Osimertinib after CIT (nivolumab, pembrolizumab, or ipilimumab + nivolumab) is also associated with severe immune-related AEs. In a phase II clinical trial of pembrolizumab followed by osimertinib, a treatment-related death occurred due to pneumonia. These data reveal the importance of testing for oncogenic driver mutations in eNSCLC to ensure that patients receive appropriate first-line neoadjuvant treatment and avoid toxicities from subsequent therapies.
Overall, neoadjuvant targeted therapy is expected to be well-tolerated and compatible with curative surgery. The safety and tolerability of osimertinib in both advanced and early patients (as adjuvant treatment) are consistent, providing confidence that no new safety issues related to neoadjuvant osimertinib treatment will arise. Additionally, preliminary data from the NAUTIKA1 study indicate that alectinib neoadjuvant treatment presents no new safety concerns. Ongoing clinical trials will provide further information on the safety and tolerability of neoadjuvant TT for eNSCLC.
Conclusion
For resectable early NSCLC patients, surgery plus (neoadjuvant) chemotherapy or, in rare cases, neoadjuvant chemoradiotherapy is associated with unacceptable rates of recurrence and low survival rates. Given the survival benefits of TT in advanced disease, these drugs are currently being explored for eNSCLC patients. Results from ongoing clinical trials suggest that neoadjuvant TT may be effective in EGFR and ALK-positive eNSCLC patients and may improve prognosis. Additional data from ongoing trials are eagerly awaited to determine whether neoadjuvant targeted therapy is feasible for eNSCLC patients with different oncogenic driver mutations.
As the field progresses towards the use of TT in eNSCLC, it is important to incorporate molecular testing and biomarker screening into clinical practice at diagnosis to optimize treatment regimens and clinical outcomes. A unified and robust surrogate marker is needed to accelerate the approval of TTs, which remains a challenge. Based on efficacy data from TT in aNSCLC and promising preliminary results from clinical trials, neoadjuvant TT holds the potential to improve the prognosis of eNSCLC patients with oncogenic driver mutations, changing the treatment landscape for early patients.
References:
Lee JM, McNamee CJ, Toloza E, Negrao MV, Lin J, Shum E, Cummings AL, Kris MG, Sepesi B, Bara I, Kurtsikidze N, Schulze K, Ngiam C, Chaft JE. Neoadjuvant Targeted Therapy in Resectable NSCLC: Current and Future Perspectives. J Thorac Oncol. 2023 Nov;18(11):1458-1477. doi: 10.1016/j.jtho.2023.07.006. Epub 2023 Jul 13. PMID: 37451404.
Recommended Reading:1. 17 Fourth-Generation Targeted Drugs to Overcome EGFR Resistance in Lung Cancer2. Understanding: Drug Treatment for Pancreatic Cancer3. What Makes Long-Term Survivors of Ovarian Cancer Special?4. How Cancer Cells Are Generated? Which Sites Do Cancer Cells Prefer to Metastasize?5. Tumor Ablation Techniques for Safer and More Effective Cancer Treatment!6.In the Next 30 Years, Cancer Will Cost China $6 Trillion! Increasing Spending on Screening, Diagnosis, and Treatment Will Benefit | Chen Siyiao/David Bloom/Wang Chen’s Latest Research7. Combating Cancer Pain: Common Treatment Drugs and Dosages8. Stay Away from Colon Cancer: These Medical Knowledge You Must Know! (22 Types of People Must Get Checked ASAP)9.The National Cancer Center Unveils the First “National Cancer High Incidence Map by Province,” with Lung Cancer Ranking First in Incidence of Malignant Tumors in China!10. Clinical Application of High-Throughput Sequencing (NGS) in Gastric Cancer: Chinese Expert Consensus (2023 Edition)——End of This Issue——We (Yishixiang, WeChat ID: medhealife) are committed to reporting scientific research results in the field of oncology and disseminating popular science knowledge; focusing on cancer prevention, early screening, early diagnosis, treatment, and rehabilitation management throughout the cancer life cycle to provide the latest information for doctors, patients, and related personnel; contributing to the benefit of medicine.