Currently, for patients with non-valvular atrial fibrillation (NVAF) who cannot tolerate or do not wish to undergo long-term anticoagulation therapy to prevent stroke, percutaneous left atrial appendage closure (LAAC) is an effective and safe surgical method for stroke prevention in atrial fibrillation (AF) patients. Regarding the management after LAAC, guidelines recommend short-term anticoagulation post-surgery, followed by dual antiplatelet therapy (DAPT) until 6 months post-operation, and finally lifelong treatment with aspirin alone. For patients who do not meet the criteria for warfarin, novel oral anticoagulants (NOACs) can be used for anticoagulation to prevent device-related thrombosis (DRT) and promote endothelialization of the closure device. However, there is currently no clinical data comparing the efficacy and safety of dabigatran and rivaroxaban for anticoagulation after LAAC. Recently, a single-center prospective cohort study was conducted to compare the safety and efficacy of different types of NOACs used after LAAC.This study consecutively included 250 patients who successfully had a left atrial appendage closure device implanted. All patients received a 3-month course of NOACs after LAAC to promote endothelialization of the device, with approximately 97 receiving dabigatran (38.8%) and 153 receiving rivaroxaban (61.2%). They then underwent dual antiplatelet therapy until 6 months post-operation, and continued lifelong aspirin therapy after discharge. During this period, transesophageal echocardiography (TEE) was used to assess thrombosis formation/dissolution on the device. The results showed that within the 3 months of anticoagulation therapy, a total of 11 cases of DRT occurred, with 8 patients on dabigatran and 3 patients on rivaroxaban. For patients who experienced DRT, NOACs were switched to warfarin, and anticoagulation was continued for 3 months before re-evaluating the TEE to confirm whether the thrombus had dissolved. The study utilized K-M curves to assess the cumulative event occurrence, showing that during the 6-month follow-up period, the DRT incidence in the rivaroxaban group was significantly lower than that in the dabigatran group (P=0.038, OR=3.843, 95% CI: 0.991–14.836). Furthermore, TEE results regarding thrombus size indicated that the average length and width of DRT in the dabigatran group were significantly higher than in the rivaroxaban group (2.16mm vs. 1.60mm, P=0.017; 1.71mm vs. 1.30mm, P=0.003). For patients with DRT, after switching NOACs to warfarin for 3 months, the average length and width of the thrombus post-dissolution in the dabigatran and rivaroxaban groups were 0.64mm vs. 0.40mm, P=0.206; 0.43mm vs. 0.27mm, P=0.082, respectively. Additionally, there were no significant differences between the two groups in coagulation indicators, cardiac function, and bleeding events.The study results suggest that compared to dabigatran, administering rivaroxaban after LAAC may be a more favorable choice, as it can prevent DRT complications without increasing the risk of bleeding. Furthermore, for patients who experience DRT, switching NOACs to warfarin for continued anticoagulation is a viable option.
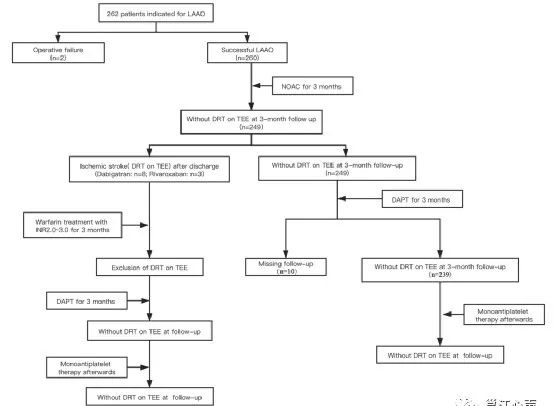
Figure 1. Study Flowchart
Table 1. Baseline Characteristics of the Study Population
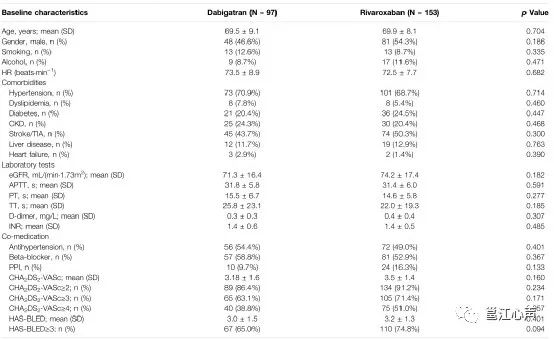
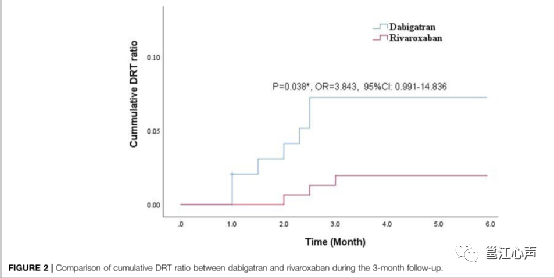
Figure 2. Cumulative Events of DRT in Both Groups
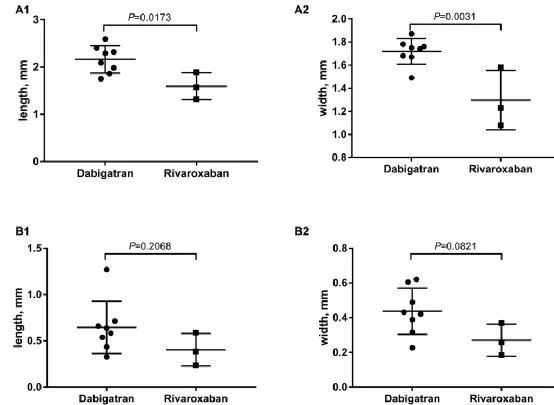
Figure 3. Dissolution of DRT in Both Groups
Source: Li X, Zhang X, Jin Q, Xue Y, Lu W, Ge J, Zhou D, Lv Q, Clinical Efficacy and Safety Comparison of Rivaroxaban and Dabigatran for Nonvalvular Atrial Fibrillation Patients Undergoing Percutaneous Left Atrial Appendage Closure Operation[J]. Front Pharmacol 2021;12
Planning: Ying Zhong
Review: Jiang Wen
Guidance: Su Su
Supervision: Qing Wei