Research Background
Previous studies have shown that the incidence of DRT after LAAC is between 1% and 10%, and device thrombosis can have serious adverse effects on patient prognosis. Therefore, the effectiveness of post-device anticoagulation therapy needs to be strengthened. Currently, there is no clear consensus on the best postoperative anticoagulation strategy to prevent DRT after LAAC. This study aims to evaluate the long-term efficacy differences between standard anticoagulation strategies and half-dose DOAC after WATCHMAN device implantation.
Research Protocol
After successful left atrial appendage closure, patients were given standard anticoagulation therapy (SAT group, i.e., 45 days of DOAC + aspirin, followed by aspirin + clopidogrel for 6 months, then switched to aspirin monotherapy) or long-term half-dose DOAC (Hd DOAC group). The primary composite endpoints were DRT, thromboembolism (TE), and major bleeding events.
Research Results
From December 2014 to September 2019, a total of 555 patients underwent successful left atrial appendage closure at three centers (mean age 75±8 years, 63% male; median CHA₂DS₂-VASc score of 4, median HAS-BLED score of 3), divided into two groups (SAT group 357 cases, Hd DOAC group 198 cases), with similar baseline characteristics between the two groups. The median follow-up time was 13 months, and the follow-up results showed that 12 patients (2.1%) experienced DRT, all in the SAT group (3.4% vs 0.0%, P=0.009). In the SAT group, the incidence of the primary composite endpoint of DRT, TE, and major bleeding events was 9.5%, while in the Hd DOAC group it was only 1.0%. Compared to standard anticoagulation therapy, postoperative use of half-dose DOAC was also associated with a lower incidence of thromboembolic events (0.5% vs. 3.1%, P = 0.08), DRT/thromboembolic events (0.5% vs. 5.6%, P = 0.018), and major bleeding (0.5% vs. 3.9%, P = 0.04). There were no differences in all-cause mortality and cardiovascular mortality between the two groups. (Figure 1)
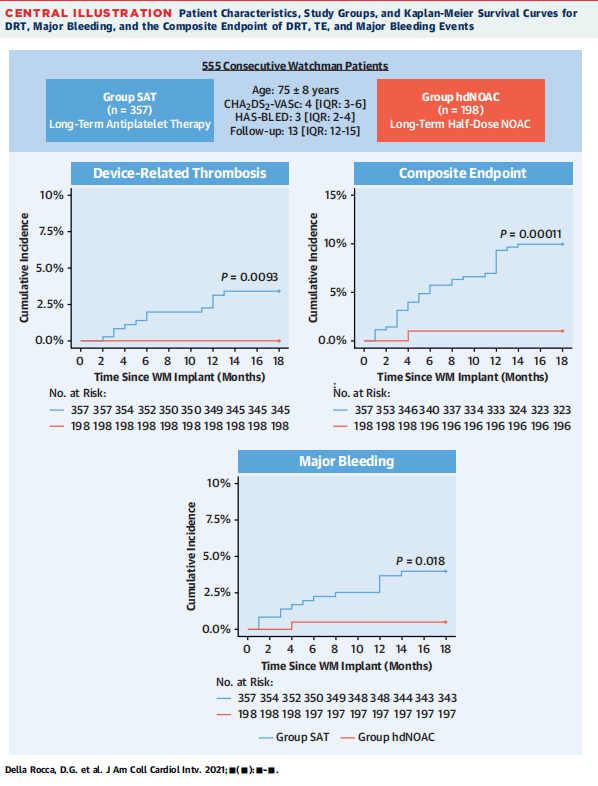
Figure 1. Characteristics of the enrolled population and study endpoints
After successful WATCHMAN implantation, long-term half-dose DOAC significantly reduced the risk of composite endpoint events of DRT, TE, and major bleeding compared to standard anticoagulation therapy.
Professor Domenico Della Rocca (Texas Cardiac Arrhythmia Institute, St. David’s Medical Center, Austin) stated that multiple studies have demonstrated that WATCHMAN implantation activates coagulation factors rather than platelets. Therefore, using low-dose anticoagulants to prevent DRT and reduce bleeding risk is a feasible strategy. Based on the results of this prospective, non-randomized study, half-dose DOAC may replace current postoperative standard anticoagulation therapy, but further validation from randomized trial results is still needed. In light of this, their team is conducting the FAD-DRT trial, which plans to include 360 patients to evaluate three anticoagulation strategies after Watchman FLX implantation: standard therapy, genetics-based customized therapy, and half-dose DOAC therapy, which may reveal clearer answers.
Professor Jens Erik Nielsen-Kudsk (Aarhus University Hospital, Denmark) pointed out in the commentary that the issue of DRT after left atrial appendage closure deserves attention. Since patients undergoing LAAC usually have a high bleeding risk, formulating the best postoperative anticoagulation therapy plan is very challenging. The results of this study are surprising; however, the limitations present in the study cannot be ignored: non-randomized controlled design, and selection bias, as patients who had indications for long-term antiplatelet therapy (e.g., those at high risk for coronary artery disease) or indications for reduced-dose anticoagulation therapy (e.g., patients with renal failure) were excluded. Nevertheless, this study preliminarily explored the feasibility of half-dose DOAC therapy after LAAC, and further controlled trials will be conducted for validation. In addition to exploring the efficacy of different anticoagulation strategies, future development of closure devices may directly integrate anticoagulants into the device to reduce DRT and postoperative bleeding.
This content is original to the “Outpatient” magazine. Reproduction requires authorization and must indicate the source.


Official WeChat of “Outpatient” magazine
Long press to scan the QR code to follow