 C-reactive protein (CRP) is an acute-phase response protein induced by interleukin 6 (IL-6) produced in liver cells, with normal reference value < 5 mg/L. The advancement of testing technology has improved the sensitivity and accuracy of CRP detection. Existing testing instruments can detect extremely low concentrations of CRP in serum samples, known as high-sensitivity C-reactive protein (HS-CRP).When the body is infected or tissue is damaged, CRP rises sharply in plasma, functioning by activating complement and enhancing phagocytosis to eliminate invading pathogens and damaged, necrotic, or apoptotic tissue cells. Therefore, it plays an important protective role in the body’s innate immune process. CRP is a nonspecific inflammatory marker, and its elevation cannot simply indicate bacterial infection. In addition to infection, tissue damage, inflammation, and stress can also cause CRP to begin rising after 6 hours, peaking at 1-2 days.The pathological mechanism of CRP in the inflammatory response is quite complex. As shown in Figure 1, inflammatory trigger factors induce the release of cytokines (such as IL-1β or IL-6) in the peripheral system, leading to CRP synthesis in the liver. CRP activates the complement system and the FcγR receptors on monocytes, promoting macrophage activation, transport, and induction of inflammatory signaling cascades. This cascade can also activate endothelial FcγR receptors in the central nervous system (CNS), upregulating CRP expression in microglia.
C-reactive protein (CRP) is an acute-phase response protein induced by interleukin 6 (IL-6) produced in liver cells, with normal reference value < 5 mg/L. The advancement of testing technology has improved the sensitivity and accuracy of CRP detection. Existing testing instruments can detect extremely low concentrations of CRP in serum samples, known as high-sensitivity C-reactive protein (HS-CRP).When the body is infected or tissue is damaged, CRP rises sharply in plasma, functioning by activating complement and enhancing phagocytosis to eliminate invading pathogens and damaged, necrotic, or apoptotic tissue cells. Therefore, it plays an important protective role in the body’s innate immune process. CRP is a nonspecific inflammatory marker, and its elevation cannot simply indicate bacterial infection. In addition to infection, tissue damage, inflammation, and stress can also cause CRP to begin rising after 6 hours, peaking at 1-2 days.The pathological mechanism of CRP in the inflammatory response is quite complex. As shown in Figure 1, inflammatory trigger factors induce the release of cytokines (such as IL-1β or IL-6) in the peripheral system, leading to CRP synthesis in the liver. CRP activates the complement system and the FcγR receptors on monocytes, promoting macrophage activation, transport, and induction of inflammatory signaling cascades. This cascade can also activate endothelial FcγR receptors in the central nervous system (CNS), upregulating CRP expression in microglia.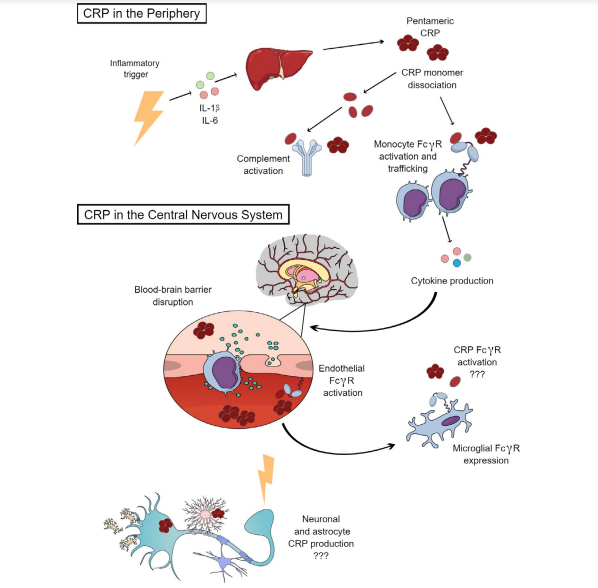 Figure 1: Pathological Mechanism of CRP in Peripheral and CNS Inflammatory Responses [1]CRP interacts with complement C1q and FcTR to produce various biological activities, including host defense against infection, phagocytosis, and modulation of inflammatory responses. Therefore, CRP’s binding to damaged cells, apoptotic cells, and nuclear antigens plays an important role in autoimmune diseases.As a commonly used clinical biomarker for infection or inflammation, the levels of CRP are of significant value in clinical assessment of infectious pathogens, severity of patient condition, and distinguishing between infectious and non-infectious diseases. Once the cause is identified, the rise and fall of CRP are closely related to the appropriateness of treatment measures and the judgment of disease outcome.CRP in Judging Infectious PathogensCRP levels in viral infections are often normal or mildly elevated, while in bacterial infections, CRP levels rise more significantly; 80% of bacterial infection patients have CRP > 100 mg/L [2].Other studies indicate thatCRP < 10 mg/L can basically rule out bacterial infection. In confirmed bacterial infections, the average CRP level in Gram-positive bacterial infections is 48 mg/L; while in Gram-negative bacterial infections, CRP levels are 2 times higher than in Gram-positive infections [3].CRP for Assessing Infection Severity and Treatment DurationFor confirmed infections, when serum CRP levels are in the range of 10-100 mg/L, it often indicates the presence oflocal or superficial infections; if CRP ≥ 100 mg/L, then invasive infection or septicemia should be considered [2].If the CRP level in infected patients significantly decreases compared to before treatment, it indicates that the current anti-infection treatment is effective, and CRP levels can provide a reference for assessing the duration of anti-infection treatment. Therefore, CRP levels can be used to assess the severity of infection, differentiate severe infections, and provide references for evaluating anti-infection treatment, benefiting patients.CRP in Evaluating Infectious DiseasesAppendicitisThe GCGH team conducted a retrospective analysis of 1,076 pediatric cases admitted for acute abdominal pain to explore the diagnostic value of CRP levels in appendicitis. The study found that if a child’s CRP < 10 mg/L and abdominal pain symptoms > 48 hours, the likelihood of appendicitis is low. Using CRP 10 mg/L as a critical threshold for preliminary diagnosis of appendicitis, its sensitivity and specificity were 0.87 (95% CI, 0.77-0.94) and 0.77 (95% CI, 0.74-0.79), respectively.It is noteworthy that CRP’s specificity is not high. Surgery, trauma, autoimmune diseases, tumors, myocardial infarction, and other non-infectious diseases can also lead to elevated serum CRP levels.Non-infectious Diseases with Elevated CRPPulmonary Embolism (PTE)In 379 PTE patients, serum CRP levels ranged from 0.3 to 813.2 mg/L, with 288 patients having elevated CRP (> 10.0 mg/L) and 91 patients having normal CRP (0.1-10.0 mg/L) [5]. This study indicates that most PTE patients have elevated CRP levels, possibly related to CRP promoting blood coagulation.Cardiovascular DiseasesCRP promotes atherosclerosis, blood coagulation, and plaque formation, and the pathological process of cardiovascular diseases includes leukocyte invasion and inflammation of the vascular wall; thus, patients with cardiovascular diseases tend to have higher serum CRP levels. Some scholars suggest including CRP along with low-density lipoprotein cholesterol (LDL-C) and total cholesterol (TC) in the biochemical indicators for diagnosing cardiovascular diseases [6].Rheumatoid Arthritis (RA)The onset of RA is related to the activation of macrophages and mast cells, leading to the induction of IL-6, tumor necrosis factor (TNF), and the production and release of CRP. The trend of CRP levels in RA patients is significant for assessing their response to drug treatment and disease progression.The Nawata M team recruited 244 RA cases treated with infliximab for at least one year, and analyzed the modified total change score (mTSS) of subjects using multivariate logistic regression analysis at baseline and after 54 weeks of treatment. The trial found that CRP in effective RA patients treated with infliximab decreased from baseline 1200 mg/L to 100 mg/L. Therefore, high CRP levels in RA patients during infliximab treatment are independent predictors of disease progression (such as exacerbation of joint destruction), and the rise and fall of CRP levels are associated with the activity of other autoimmune diseases and treatment outcomes.Gastric CancerLu J et al. analyzed CRP levels in 401 gastric cancer patients before and after radical gastrectomy and conducted multifactorial analysis to explore independent variables for recurrence-free survival (RFS). The trial showed that preoperative CRP ≥ 3.1 mg/L and postoperative peak CRP (CRPmax) ≥ 77.1 mg/L are both risk factors for RFS [8].It is important to note that CRP can elevate during the active phase of malignant tumors. Therefore, routine follow-up of CRP in patients with malignant tumors can assist in assessing the progression of their condition.Acute PancreatitisIn severe acute pancreatitis patients, serum CRP concentrations can reach ≥ 200 mg/L, and the severity of the condition is positively correlated with CRP levels. Using a CRP level of 210 mg/L as a reference for assessing the severity of acute pancreatitis, its sensitivity is 83% and specificity is 85% [9].ConclusionThis article summarizes the pathological mechanisms of CRP as a biomarker in infection or inflammatory responses and discusses its clinical value in inferring infectious pathogens and assessing infection severity. CRP’s specificity is not high; both infectious and non-infectious diseases can cause its levels to rise, but the rise and fall of CRP levels have guiding significance for clinical practice. Therefore, common diseases that lead to elevated CRP levels are listed in this article, hoping to provide some suggestions for clinical diagnosis and treatment.This article was first published on the professional platform under Dingxiangyuan: Dingxiangyuan Respiratory TimePlanning: ChaochaoReview Experts:
Figure 1: Pathological Mechanism of CRP in Peripheral and CNS Inflammatory Responses [1]CRP interacts with complement C1q and FcTR to produce various biological activities, including host defense against infection, phagocytosis, and modulation of inflammatory responses. Therefore, CRP’s binding to damaged cells, apoptotic cells, and nuclear antigens plays an important role in autoimmune diseases.As a commonly used clinical biomarker for infection or inflammation, the levels of CRP are of significant value in clinical assessment of infectious pathogens, severity of patient condition, and distinguishing between infectious and non-infectious diseases. Once the cause is identified, the rise and fall of CRP are closely related to the appropriateness of treatment measures and the judgment of disease outcome.CRP in Judging Infectious PathogensCRP levels in viral infections are often normal or mildly elevated, while in bacterial infections, CRP levels rise more significantly; 80% of bacterial infection patients have CRP > 100 mg/L [2].Other studies indicate thatCRP < 10 mg/L can basically rule out bacterial infection. In confirmed bacterial infections, the average CRP level in Gram-positive bacterial infections is 48 mg/L; while in Gram-negative bacterial infections, CRP levels are 2 times higher than in Gram-positive infections [3].CRP for Assessing Infection Severity and Treatment DurationFor confirmed infections, when serum CRP levels are in the range of 10-100 mg/L, it often indicates the presence oflocal or superficial infections; if CRP ≥ 100 mg/L, then invasive infection or septicemia should be considered [2].If the CRP level in infected patients significantly decreases compared to before treatment, it indicates that the current anti-infection treatment is effective, and CRP levels can provide a reference for assessing the duration of anti-infection treatment. Therefore, CRP levels can be used to assess the severity of infection, differentiate severe infections, and provide references for evaluating anti-infection treatment, benefiting patients.CRP in Evaluating Infectious DiseasesAppendicitisThe GCGH team conducted a retrospective analysis of 1,076 pediatric cases admitted for acute abdominal pain to explore the diagnostic value of CRP levels in appendicitis. The study found that if a child’s CRP < 10 mg/L and abdominal pain symptoms > 48 hours, the likelihood of appendicitis is low. Using CRP 10 mg/L as a critical threshold for preliminary diagnosis of appendicitis, its sensitivity and specificity were 0.87 (95% CI, 0.77-0.94) and 0.77 (95% CI, 0.74-0.79), respectively.It is noteworthy that CRP’s specificity is not high. Surgery, trauma, autoimmune diseases, tumors, myocardial infarction, and other non-infectious diseases can also lead to elevated serum CRP levels.Non-infectious Diseases with Elevated CRPPulmonary Embolism (PTE)In 379 PTE patients, serum CRP levels ranged from 0.3 to 813.2 mg/L, with 288 patients having elevated CRP (> 10.0 mg/L) and 91 patients having normal CRP (0.1-10.0 mg/L) [5]. This study indicates that most PTE patients have elevated CRP levels, possibly related to CRP promoting blood coagulation.Cardiovascular DiseasesCRP promotes atherosclerosis, blood coagulation, and plaque formation, and the pathological process of cardiovascular diseases includes leukocyte invasion and inflammation of the vascular wall; thus, patients with cardiovascular diseases tend to have higher serum CRP levels. Some scholars suggest including CRP along with low-density lipoprotein cholesterol (LDL-C) and total cholesterol (TC) in the biochemical indicators for diagnosing cardiovascular diseases [6].Rheumatoid Arthritis (RA)The onset of RA is related to the activation of macrophages and mast cells, leading to the induction of IL-6, tumor necrosis factor (TNF), and the production and release of CRP. The trend of CRP levels in RA patients is significant for assessing their response to drug treatment and disease progression.The Nawata M team recruited 244 RA cases treated with infliximab for at least one year, and analyzed the modified total change score (mTSS) of subjects using multivariate logistic regression analysis at baseline and after 54 weeks of treatment. The trial found that CRP in effective RA patients treated with infliximab decreased from baseline 1200 mg/L to 100 mg/L. Therefore, high CRP levels in RA patients during infliximab treatment are independent predictors of disease progression (such as exacerbation of joint destruction), and the rise and fall of CRP levels are associated with the activity of other autoimmune diseases and treatment outcomes.Gastric CancerLu J et al. analyzed CRP levels in 401 gastric cancer patients before and after radical gastrectomy and conducted multifactorial analysis to explore independent variables for recurrence-free survival (RFS). The trial showed that preoperative CRP ≥ 3.1 mg/L and postoperative peak CRP (CRPmax) ≥ 77.1 mg/L are both risk factors for RFS [8].It is important to note that CRP can elevate during the active phase of malignant tumors. Therefore, routine follow-up of CRP in patients with malignant tumors can assist in assessing the progression of their condition.Acute PancreatitisIn severe acute pancreatitis patients, serum CRP concentrations can reach ≥ 200 mg/L, and the severity of the condition is positively correlated with CRP levels. Using a CRP level of 210 mg/L as a reference for assessing the severity of acute pancreatitis, its sensitivity is 83% and specificity is 85% [9].ConclusionThis article summarizes the pathological mechanisms of CRP as a biomarker in infection or inflammatory responses and discusses its clinical value in inferring infectious pathogens and assessing infection severity. CRP’s specificity is not high; both infectious and non-infectious diseases can cause its levels to rise, but the rise and fall of CRP levels have guiding significance for clinical practice. Therefore, common diseases that lead to elevated CRP levels are listed in this article, hoping to provide some suggestions for clinical diagnosis and treatment.This article was first published on the professional platform under Dingxiangyuan: Dingxiangyuan Respiratory TimePlanning: ChaochaoReview Experts: