Click the title below to follow this accountContinuously obtain knowledge and information on adverse pregnancy
●Comprehensively understand the knowledge points related to pregnancy failure, avoid detours, and quickly have a baby!
●Flexibly use the search function of the public account, access the menu bar, and use keyword auto-replies to quickly read previously published articles or materials.
Previously, we published an article related to “cells” titled “Understanding T Cell Cytokines, Serum Cytokines, Regulatory T Cells (Treg), and Lymphocyte Subpopulations”. Besides cells, another term that is quite common is protein!

Don’t make a fuss, I didn’t call you! But you are indeed a protein! Haha! But since you are here, let me recommend an article: “One Egg a Day, Don’t Waste the Yolk!” Wow, Master, you also have such popular science! Yes, were you and your friends surprised?

Actually, the proteins we are going to talk about today are mainly Protein C/S, Anti-Protein C/S Antibodies, C-Reactive Protein, High-Sensitivity C-Reactive Protein, Immunoglobulin MAGDE (testing items), Intravenous Immunoglobulin (blood products), Human Serum Albumin (blood products), are you confused? Explaining them can be quite tiring, so here comes a series of “Understanding in One Article” on proteins, which is relatively convenient. If you have questions, just throw the article!

Just right, Dr. Chen Zeyu gave a talk on the application of “Immunoglobulin in Immune-related Adverse Pregnancy” at the Academic Exchange and Patient Education Conference on Recurrent Adverse Pregnancy held in Qingdao on May 31. When I asked Dr. Chen about the knowledge of Immunoglobulin MAGDE and C-Reactive Protein, I suggested that he write a popular science article about various terms containing the word protein, and Dr. Chen readily agreed!

Dr. Chen Zeyu is a doctor in the Rheumatology and Immunology Department of Jiamusi Central Hospital. Three years ago, he studied the diagnosis and treatment of immune-related adverse pregnancy under Professor Liu Xiangyuan from Peking University Third Hospital. After returning to the hospital, he has gained fame in Jiamusi, Heilongjiang, and even in the three northeastern provinces for his work in preserving pregnancy, with patients coming from outside the province and even abroad.Currently, he is the first person to return for further training, studying the diagnosis and treatment of immune-related adverse pregnancy under Professor Liu Xiangyuan for the second time. He also serves as the leader of the training doctor group and will be responsible for the short-term intensive training class of Liu Xiangyuan’s studio in July-August, showing a determination to become a warrior! So, thank you, Leader Chen, for taking the time to write for me amidst your busy schedule, and I asked him to revise it twice! I want to set this as an original article, and the income from appreciation will be paid to Leader Chen as a manuscript fee . Additionally, to show my gratitude, I am placing Dr. Chen Zeyu’s online consultation QR code here. Patients who need consultation during pregnancy preparation or require monthly packages for preserving pregnancy (600 yuan/month, will the price increase after this article is published?
. Additionally, to show my gratitude, I am placing Dr. Chen Zeyu’s online consultation QR code here. Patients who need consultation during pregnancy preparation or require monthly packages for preserving pregnancy (600 yuan/month, will the price increase after this article is published?  ), can scan or long-press to identify, and feel free to ask him any questions:
), can scan or long-press to identify, and feel free to ask him any questions:

Now, let’s publish the knowledge about Protein C/S, Anti-Protein C/S Antibodies, C-Reactive Protein, High-Sensitivity C-Reactive Protein, Immunoglobulin (testing items), Intravenous Immunoglobulin (blood products), Human Serum Albumin (blood products), and other terms containing the word “protein”. Some opinions from Director Guo Zhongjie or other doctors will be interspersed, and will be specifically noted.
Guo Zhongjie Talks About Protein C/S
Speaking of Protein C and Protein S, we really need to share the article by Director Guo Zhongjie titled “Let’s Talk About Anticoagulation! Protein S, Protein C, Antithrombin III” as follows:
The Significance of Blood Flowing in Blood Vessels
First, it carries oxygen to the whole body
Second, it brings nutrients to the whole body
Third, it removes metabolic waste from various parts
Blood flow is the driving force of metabolism. What would happen without blood flow? It’s simple: you would die! Any part where blood does not flow will die!
For example, if a brain blood vessel does not flow, it leads to a cerebral infarction!
If the coronary artery of the heart is blocked and blood does not flow, it leads to a myocardial infarction!
The same type of blood vessel blockage can occur in various parts of the body! Some people have renal vascular blockage, and others have lower limb vascular blockage. This is abnormal blood coagulation.
If your hand is cut with a knife, blood will flow out, but soon it will coagulate. Why is that? The reason is simple: blood must remain flowing inside the blood vessels, and once it is outside the vessels, it must coagulate. This is a natural mechanism given to humanity by nature, which is the coagulation and anticoagulation mechanism!
When the hand is cut, blood will stop, which is not our topic today. Today we are discussing Protein S, Protein C, and Antithrombin III in the blood vessels.
These three are the main forces that maintain blood flow; only when they work normally can the blood vessels avoid embolism. Blockage of blood vessels in the embryo is an important reason for fetal arrest.

Protein S and Protein C: Both are blood components synthesized by the liver and are the main anticoagulants. Protein S is a suicide squad, with a very short lifespan; Protein C is a long-term warrior, but its endurance is also not long, about only a few minutes. Both can only detect activity.
By the way, let’s talk about Antithrombin III, in hospitals in Guangdong, it is generally detected for the activity of Antithrombin III, which means checking how strong the fighting ability of Antithrombin III is. Having a lot of soldiers does not necessarily mean winning the battle, right?! Sometimes elite soldiers are more useful than a bunch of useless ones! Why do we emphasize detecting activity? Because there is a portion of the population in China with genetic mutations in Antithrombin III. These individuals may have a sufficient quantity of Antithrombin III, but their activity is poor! Rather than checking how many people exist, it is better to check how much labor force there is.
The reference range for Antithrombin III antigen is 25, and the reference lower limit for Antithrombin III activity is 85, which is the unified standard in China. What if there is a genetic mutation? Even if there is a sufficient quantity of Antithrombin III, the activity will still be poor!
So what to do if the levels of these three anticoagulants are found to be low? What are the implications?
Low detection data for these three anticoagulants indicates a high coagulation state in the blood or a tendency towards high coagulation. Once pregnant, under the hormonal changes during pregnancy, the high coagulation state will worsen, and if the blood vessels supplying the embryo become blocked, the nutritional supply to the embryo will be compromised, leading to fetal arrest.
The impact of a deficiency in these three substances on fetal arrest is sequential: lowest for Protein S, next for Protein C, and the most significant impact is from Antithrombin III.
Protein S deficiency only requires appropriate anticoagulation.
Protein C deficiency requires a longer duration of low molecular weight heparin use.
If there is Antithrombin III deficiency, heparin may need to be used until about 32 weeks.
Of course, if there is a deficiency of two or more anticoagulants, the situation may be worse.
Targeted treatment:
In cases of deficiency of these anticoagulants, what treatment options do we have?
The first is aspirin, the most common medication;
The second is low molecular weight heparin products;
The third is the “protein C” developed in Japan, which directly injects Protein C to solve the deficiency of anticoagulants, but this invention from Japan is too expensive, costing 8000 RMB for a week’s supply.
When adjusting the dosage of low molecular weight heparin for different situations, we will consider many factors, such as weight, age, and whether there are other factors causing a high coagulation state, such as immobility, prolonged bed rest, hyperhomocysteinemia, etc.
The duration and dosage of low molecular weight heparin use will still depend on monitoring results; there is no fixed formula for this.
Alright, after sharing Director Guo Zhongjie’s article, the following content is all from Dr. Chen Zeyu, and the blue words may also be my interjections:
Protein C and Protein S
The Protein C system is a plasma protein system with anticoagulant properties, including Protein C (proteinC: PC), Protein S (proteinS: PS), Thrombomodulin (TM), and Activated Protein C Inhibitor (APCI).
Protein C and Protein S are both vitamin K-dependent anticoagulant proteins synthesized in the liver, and the Protein C system plays an important role in the fluid anticoagulation system. Its anticoagulation pathways include: ① Inactivation of coagulation factors V and VIII; ② Limiting the binding of factor Xα to platelets; ③ Enhancing the dissolution of fibrin.
Protein C: a vitamin K-dependent proenzyme synthesized in the liver, binds to Protein S on the surface of platelets, and together they function. Its main role is to inactivate coagulation factors Vα and VIIIα after activation, inhibiting blood coagulation. Normal PC activity: 70%-140%.
Protein S: a vitamin K-dependent proenzyme synthesized in the liver, serves as a cofactor to synergistically activate Protein C, eliminating the protective effect of coagulation factors IXα on factors Vα and VIIIα, allowing them to be hydrolyzed, thus inhibiting blood coagulation. Normal PS activity: 63.5%-149%.
Let me interject: A value below the reference lower limit indicates a coagulation issue, while a higher value can be ignored.
Thrombomodulin (optional)
Thrombomodulin (TM): Binds to thrombin to reduce its coagulation activity while enhancing its ability to activate Protein C. Since activated Protein C has anticoagulant properties, TM is an important vascular factor that shifts thrombin from pro-coagulant to anti-coagulant. Reference value: 20-35.
Activated Protein C becomes an effective anticoagulant, and its activation through interaction with thrombin is significantly lower than the 1000-fold activation of Protein C by the thrombin-TM complex on endothelial cells. Activated Protein C inhibits blood coagulation formation through proteolytic action and selectively inactivates factors Va and VIIIa. This reaction requires the presence of Protein S. In the normal population, Protein C deficiency accounts for 0.4%, with an incidence of thrombosis at 5%-8%. Young people with periodic thromboembolic disease can be as high as 10%-15%. JH Griffin first reported hereditary Protein C deficiency in 1983, where patients are heterozygous, with Protein C antigen levels only 38%-49% of normal, presenting with recurrent venous thromboembolism. Homozygous patients often present at birth with neonatal purpura, with Protein C levels less than 5% of normal, with an incidence of 1/600000, leading to necrotizing skin damage due to capillary bed embolism, brain, eye damage, and DIC. Reduced Protein C can also be seen in cases of decreased hepatic synthesis, severe liver disease, vitamin K deficiency, or the use of anticoagulant medications such as warfarin or coumarin, excessive consumption, seen in DIC, major surgeries, deep vein thrombosis, etc. Impaired activation of Protein C occurs in adult respiratory distress syndrome, severe infections, vascular endothelial damage, SLE, and other diseases due to reduced TM. In addition, Dohlback reported a familial tendency to thrombosis due to a lack of response to activated Protein C (APC), later confirmed to be due to mutations in the coagulation factor Vα gene, which causes resistance to activated Protein C (APCR), leading to reduced inactivation of factor Vα by APC, which accounts for 40%-60% of thrombosis incidence. It is particularly noted that in APCR patients, the coagulation activity of their factor Vα is normal. However, elevated levels of Protein C or Protein S are not often associated with medical issues or considered clinically significant.
Anti-Protein C/S Antibodies
Anti-Protein C Antibodies and Anti-Protein S Antibodies are two of the atypical phospholipid antibodies found in the non-classical phospholipid antibody spectrum, detailed in Professor Liu Xiangyuan’s presentation: “Clinical Significance of Non-Classical Phospholipid Antibodies in the Diagnosis of Obstetric Antiphospholipid Syndrome (APS)“.
Anti-Protein C Antibodies and Anti-Protein S Antibodies are specific antibodies against Protein C and Protein S, a group of calcium-dependent phospholipid-binding proteins. Anti-Protein C antibodies and Anti-Protein S antibodies bind to Protein C/Protein S, blocking the protein activation pathway, leading to acquired Protein C deficiency, reducing Protein C activity, and increasing non-functional Protein C, inducing thrombosis. They are associated with severe thrombotic events, with a positive rate of 14-49%.
Let me interject: A positive result or a level above the reference upper limit indicates a tendency toward antiphospholipid syndrome (APS), and treatment can be conducted according to APS guidelines; of course, regular re-examinations may also be needed to confirm, so listen to your doctor. Professor Zhang Jianping’s view on APS: Better to believe it exists than to believe it doesn’t!
C-Reactive Protein
C-Reactive Protein (CRP) is an inflammatory protein that appears in the examination report of the rheumatic three items.
C-Reactive Protein is an acute phase reactant protein that reacts with the C polysaccharide of Streptococcus pneumoniae to form a complex. It rapidly increases after tissue damage, activating complement; promoting the destruction of melanoma cells by monocytes; facilitating the movement and phagocytosis of granulocytes and macrophages; affecting the reactivity of lymphocytes to mitogenic substances, and binding with some T lymphocytes to inhibit their function; suppressing mixed lymphocyte reactions; and inhibiting platelet aggregation and blood clot contraction. Normal CRP ≤ 10mg/L. CRP levels rise within hours of the onset of inflammation, peaking within 48 hours, and return to normal levels as lesions resolve and tissue, structure, and function recover. This reaction is not affected by radiotherapy, chemotherapy, or corticosteroid treatment. It can be used as an indicator for evaluating disease activity and monitoring treatment efficacy. The degree of CRP elevation reflects the size or activity of the inflammatory tissue, and there is a good correlation between CRP and disease activity during acute inflammation and infection.
Common causes of elevation include:
1. Tissue damage, infection, tumors, myocardial infarction, and a series of acute and chronic inflammatory diseases, such as rheumatoid arthritis, systemic vasculitis, polymyalgia rheumatica;
2. Indicators of postoperative infection and complications: CRP levels should decrease 7-10 days after surgery; if CRP does not decrease or rises again, it may indicate possible complications such as infection or thrombosis;
3. It can be used to differentiate between bacterial and viral infections: most bacterial infections will cause an increase in serum CRP levels, while viral infections usually do not.
High-Sensitivity C-Reactive Protein
High-Sensitivity C-Reactive Protein (hs-CRP) is a non-specific marker of systemic inflammatory response synthesized by the liver during the acute phase, also known as high-sensitivity C-Reactive Protein. The clinical guiding role of hs-CRP mainly manifests in cardiovascular diseases, neonatal bacterial infections, kidney transplants, etc., and is one of the strongest predictors of cardiovascular events.
In fact, high-sensitivity C-Reactive Protein is a clinical laboratory that uses high-sensitivity detection techniques to accurately measure low concentrations of C-Reactive Protein, improving the sensitivity and accuracy of the test, making it a sensitive indicator for distinguishing low-level inflammatory states. In other words, high-sensitivity C-Reactive Protein and C-Reactive Protein are both indicators of inflammatory response, but high-sensitivity C-Reactive Protein is more sensitive.
Immunoglobulin (Testing Items)
Reference: “The Application of Immunoglobulin in Immune-related Adverse Pregnancy”
Immunoglobulin (Ig) is composed of two identical light chains and two identical heavy chains and is a class of important immune effector molecules produced by the lymphocytes of higher animals’ immune systems. It can be transformed into antibodies upon antigen induction (antibodies are a biological functional concept, while immunoglobulins are a chemical structural concept. All antibodies have a chemical basis of immunoglobulin, but not all immunoglobulins have antibody activity). It primarily exists in plasma but is also found in other body fluids, tissues, and some secretions. It can be divided into five types based on structural differences: IgG, IgA, IgM, IgD, and IgE, with most being gamma globulin (γ-globulin). Immunoglobulins can be divided into antibodies and membrane immunoglobulins. Antibodies primarily exist in serum but can also be found in other body fluids and excretions, with their main function being to specifically bind to antigens and participate in humoral immunity; membrane immunoglobulins are B lymphocyte antigen receptors that can specifically recognize antigen molecules.
Immunoglobulin IgG
The main component of human serum immunoglobulin is IgG, which accounts for 70-75% of total immunoglobulin, with a molecular weight of about 150,000 and containing 2-3% sugar. Human serum immunoglobulin IgG is the most persistent and important antibody in the primary immune response, existing only in monomer form. Most antibacterial, antitoxic, and antiviral antibodies belong to IgG, which plays a major role in anti-infection. It can promote the phagocytic action of mononuclear macrophages (opsonization), neutralize the toxicity of bacterial toxins (neutralization of toxins), and bind to viral antigens to render viruses incapable of infecting host cells (neutralization of viruses). IgG synthesis in the body begins later than IgM, starting from the third month after birth, reaching levels close to adult levels by ages 3-5. It is the only Ig that can cross the placenta, playing an important role in natural passive immunity. Additionally, IgG also has opsonization and binding SPA functions. However, certain autoimmune diseases, such as autoimmune hemolytic anemia, immune thrombocytopenic purpura, lupus erythematosus, and rheumatoid arthritis, have autoimmune antibodies that are IgG. Once it binds to the corresponding self-cells, it instead exacerbates tissue damage.
Normal Values: 9.5~12.5mg/ml.
Clinical Significance:
Increased: Seen in IgG-type multiple myeloma, chronic liver disease, chronic infections, connective tissue diseases, allergic purpura, malignant lymphoma, psoriasis, leprosy, malaria, nephritis.
Decreased: Congenital immunodeficiency diseases, nephrotic syndrome, viral infections, protein-losing diseases, immunosuppressive therapy.
Immunoglobulin IgA
IgA can be divided into serum type and secretory type, with the serum type mostly being monomers, while the secretory type is all dimers and contains a secretory piece. Serum IgA can mediate opsonization and ADCC; secretory IgA (SIgA) is the main component of the body’s mucosal defense system, covering the surfaces of the nose, pharynx, trachea, intestines, and bladder. It can inhibit the attachment of microorganisms to respiratory epithelial cells, slow down viral replication, and has antibody activity against certain viruses, bacteria, and general antigens, serving as the first line of defense against the invasion of pathogens. When foreign antigens enter the respiratory or digestive tract, the local immune system is stimulated, and without the involvement of the central immune system, it can autonomously conduct an immune response, producing secretory antibodies, i.e., SIgA. Colostrum contains secretory SIgA. The aggregates of IgA can activate complement through the classical pathway.
Normal Values:
Cord blood: 0-50mg/L; Newborns: 0-22mg/L; 0.5-6 months: 30-820mg/L; 6 months-2 years: 140-1080mg/L; 2-6 years: 230-1900mg/L; 6-12 years: 290-2700mg/L; 12-16 years: 810-2320mg/L; Adults: 760-3900mg/L;
Clinical Significance:
Increased: Commonly seen in IgA-type multiple myeloma, systemic lupus erythematosus (SLE), sarcoidosis, rheumatoid arthritis, Behçet’s syndrome, portal hypertension liver cirrhosis, certain infectious diseases, eczema, and thrombocytopenia.
Decreased: Commonly seen in hereditary telangiectasia (80%), non-IgA-type multiple myeloma, heavy chain diseases, light chain diseases, malabsorption syndrome, primary immunoglobulin deficiency, secondary proteinemia, secondary hypogammaglobulinemia, secondary immunodeficiency (radiation exposure, use of immunosuppressive agents), recurrent respiratory infections, blood transfusion reactions, autoimmune diseases, nephrotic syndrome, chronic lymphocytic leukemia, Hodgkin’s disease, hereditary thymic hypoplasia, type III gammopathy (IgG and IgA decreased, IgM increased), type II gammopathy (no IgA, IgM normal) etc.
Immunoglobulin IgM
IgM is the first Ig produced in response to antigen stimulation in humoral immunity, with a strong ability to bind to antigens; it contains five Fc segments and is more effective at activating complement than IgG. It is primarily distributed in serum. IgM accounts for 5%-10% of the total serum immunoglobulin, with a serum concentration of about 1mg/ml. Due to its high binding capacity, IgM is a highly effective antibody against pathogens, with bactericidal, lytic, phagocytic, and agglutination actions 500-1000 times higher than IgG, playing an important role in the body’s early defense. For example, natural blood group antibodies are IgM, and incompatible blood transfusions can cause serious hemolytic reactions. Since IgM is the first antibody synthesized and secreted during individual development, it can be produced by a fetus as early as 20 weeks of gestation, thus elevated cord blood IgM indicates the fetus has an intrauterine infection (such as rubella virus or cytomegalovirus infection). IgM is also the first antibody to appear in the primary humoral immune response, serving as a marker for recent infections, but its duration is short.Decreased IgM is often considered in immunodeficiency diseases, non-IgA and IgG-type multiple myeloma, Hodgkin’s disease, chronic lymphocytic leukemia, protein-losing gastroenteropathy, reticuloendothelial cell proliferation diseases, and uremia.
Normal Values:
Cord blood: 40-240mg/L; Newborns: 50-300mg/L; 0.5-6 months: 150-1090mg/L; 6 months-2 years: 430-2390mg/L; 2-6 years: 500-1990mg/L; 6-12 years: 500-2600mg/L; 12-16 years: 450-2400mg/L; Adults: 400-3450mg/L.
Immunoglobulin IgD
IgD was discovered in 1995 from human myeloma protein, with a molecular weight of 175kD, mainly produced by plasma cells in the tonsils and spleen. The serum immunoglobulin D (IgD) content is very low, with a concentration of 3-40μg/ml, accounting for less than 1% of the total serum Ig. It is synthesized later in individual development. The hinge region of IgD is very long and sensitive to proteolytic hydrolysis, resulting in a short half-life of only 2.8 days. The exact immune function of IgD in serum is still unclear. It can exist as a membrane receptor on the surface of B cells, showing immune tolerance when B cells differentiate into mature B cells. After antigen stimulation, it is expressed as immune tolerance. After activation or transformation into memory B cells, SmIgD gradually disappears. Its function may be related to initiating B cells to produce antibodies and is associated with certain autoantibodies and antitoxin antibodies, such as anti-nuclear antibodies, anti-basement membrane antibodies, anti-insulin antibodies, anti-thyroid antibodies, anti-diphtheria toxin antibodies, and anti-tetanus toxin antibodies.
Reference Values: Adults: 1-60mg/L.
Clinical Significance:
Increased: ① Multiple myeloma with high IgD: chronic infectious diseases (tuberculosis, leprosy, osteomyelitis, purulent skin diseases), Kwashiorkor (malnutrition), specific reactive diseases, periodic fever (2-12 years) etc. ② Simple high IgD syndrome: IgD myeloma, benign simple immunoglobulin syndrome is rare, IgD-type multiple myeloma etc.
Decreased: IgD deficiency families (autosomal abnormalities), IgD, IgA, IgM immunoglobulin reduction is primary immunodeficiency (transient hypogammaglobulinemia in newborns, infant agammaglobulinemia), severe combined immunodeficiency (SCID), Good syndrome, significant reduction or disappearance of IgD: sarcoidosis, IgD isolated deficiency has a tendency to susceptibility etc.
Immunoglobulin IgE
IgE is a class of antibodies with δ chains, mainly involved in the regulation of the pathogenesis of allergic rhinitis, allergic asthma, and eczema. Since Japanese scholar Ishizaka discovered IgE in 1966, significant progress has been made in the study of IgE, and IgE receptors have been found on the surfaces of mast cells, basophils, eosinophils, and macrophages. Specific IgE targeting various pollen, dust mites, fungi, and animal fur has been isolated from the sera of patients with various allergic diseases, including allergic asthma. Recent years have confirmed that many cytokines such as IL-4 and γ-interferon are involved in the regulation of IgE synthesis. IgE antibodies can initiate immediate allergic reactions and induce delayed allergic reactions.
Reference Values: 0.1~0.9mg/L.
Clinical Significance:
Increased: Seen in IgE-type multiple myeloma, atopic asthma, atopic dermatitis, allergic rhinitis, parasitic infections, SLE, rheumatoid arthritis, tropical eosinophilia, certain fungal infections, hyper-IgE syndrome, and certain cellular immune deficiency syndromes (Nezelof syndrome and Wiskott-Aldrich syndrome, etc.), as well as some pediatric minimal change nephrotic syndrome.
Decreased: Seen in primary hypogammaglobulinemia, ataxia-telangiectasia, malignant tumors, and after treatment with cytotoxic drugs.
Intravenous Immunoglobulin (For Preserving Pregnancy)
Intravenous Immunoglobulin (IVIG):
With an IgG content greater than 90%, it is called gamma globulin, which is divided into human blood gamma globulin and placental blood gamma globulin based on its source. Human blood gamma globulin is extracted from human blood, with a concentration of 100 grams/liter, where immunoglobulin (IgG) accounts for 90%-95%. Placental gamma globulin (referred to as fetal globulin) is extracted from the placental blood of healthy mothers, with a concentration of 40 grams/liter, where IgG content accounts for 80%-85%. The main component of both is gamma globulin, just differing in content.Currently, the latter has been discontinued.
Its mechanism of action falls under passive immunity and automatic immune action under passive immune protection, which began to be used in the treatment of RSA in the 1980s.Its functions include:
1. IVIG can specifically recognize pathogens and bind to them, inducing phagocytes to engulf the pathogens, thereby eliminating them, i.e., exerting an anti-infection effect. For example, in the case of viral encephalitis, IVIG can effectively clear pathogens and prevent infection;
2. IVIG can also use its Fab segment to bind to toxins or antigens, encapsulating them and delivering them to phagocytes for destruction, protecting cells from toxin attacks and damage, thereby safeguarding organ and body health and accelerating recovery;
3. IVIG can neutralize antigens, preventing them from acting on target cells and reducing the production of autoantibodies by immune cells, thus preventing self-attack;
4. The large Fc segments of IgG in IVIG can bind to Fc receptors on phagocytes, preventing them from binding to self-antibodies and corresponding cytokines, thus preventing activation of phagocytes and blocking damage to body tissues and cells;
5. Directly inhibiting the maturation and proliferation of immature T cells, thereby inhibiting the secretion and production of inflammatory mediators (IL-2, 3, 4, 5, 10, and TNF-α), and IVIG contains specific antibodies against IL-1, IL-6, IL-8, and TNF, which can directly neutralize these inflammatory mediators and cytokines, reducing their blood concentration;
6. IVIG has a regulatory effect on T and B lymphocyte immune functions, inhibiting lymphocyte proliferation, regulating cell apoptosis, and maintaining the immune balance of the body;
7. By neutralizing pathological autoantibodies through unique antibodies, IVIG regulates complement to block MAC (C5b-9) membrane attack complexes from depositing in target tissues.
The following content comes from “NK Diagnosis and Treatment Logic and Countermeasures Summary (20181219 Edition)”,
Reported Dosage:
400 mg per kilogram of body weight. For example, a patient weighing 50 kg needs a dosage of: 50*0.16=8, which means 8 bottles (each bottle has a dosage of 2.5g). If it is 62 kg, then it would be 10 bottles.
Director Liu Xiangyuan believes its effects include: It can reduce NK cell counts, toxicity, and TNF-α, improve blocking antibodies, subchorionic hematomas, autoantibodies, immune intrauterine growth retardation, cardiac conduction block, or oligohydramnios, etc.
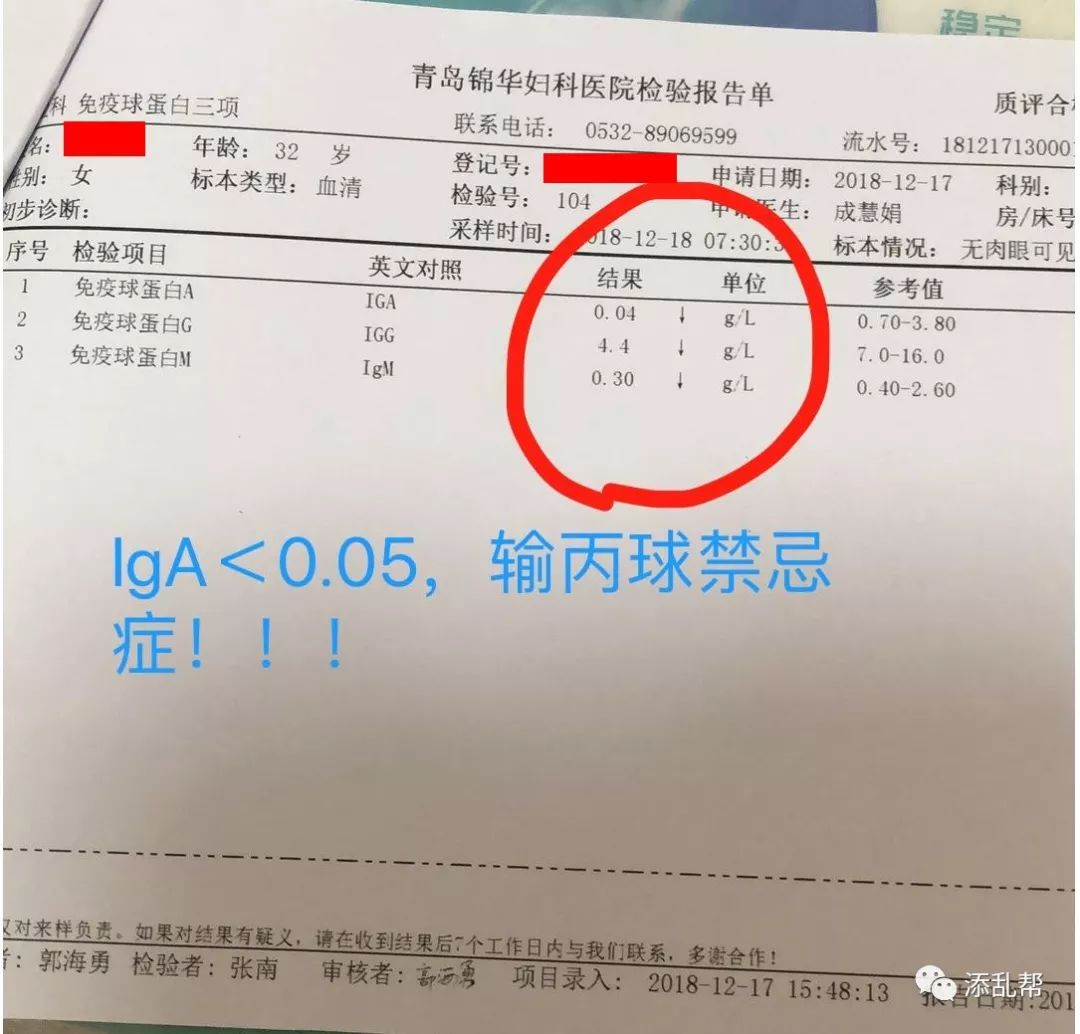
Contraindications:
1. Those allergic to immunoglobulin or with a history of other serious allergies. 2. Those with selective IgA deficiency and anti-IgA antibodies. The following image is provided by Professor Fu Jinhua with a reminder!!
3. Patients with fever should avoid or use with caution. 4. Patients with liver and kidney dysfunction or a history of heart disease should avoid. 5. Patients with a history of migraines should avoid. Adverse Reactions and Precautions:
1. However, due to individual differences, a small number of patients may experience the following adverse reactions: allergies, thrombosis, redness and pain at the injection site, fetal abnormalities, and failure of pregnancy preservation.
2. Those allergic to gamma globulin may experience acute shock and cardiac arrest, so please ensure to infuse in a formal medical institution with rescue measures, and ensure that a doctor is present during the infusion, which typically takes about 7 hours. 3. This medication is expensive; it is recommended to purchase one bottle first, and infuse 5ml while waiting for half an hour to observe for allergic reactions. 4. If normal, continue infusion according to the dosage; if there are allergic reactions, stop the infusion immediately;
5. During the infusion, be sure to drink plenty of water and urinate often, ensuring an intake of no less than 2000ml of water,or temporarily increase the injection of low molecular weight heparin to prevent high coagulation.
6. During use, monitor blood and urine routine and liver and kidney function every 1-8 weeks; please read the medication instructions carefully for precautions.
7. Store at 2-8 degrees, do not freeze.
Albumin (Not for Preserving Pregnancy)
Albumin (also known as serum albumin, albumin, Alb) is synthesized by hepatic parenchymal cells, with a half-life of about 15-19 days in plasma, and is the most abundant protein in plasma, accounting for 40%-60% of total plasma protein. Although its synthesis rate is influenced by the protein content in food, it is mainly regulated by plasma levels, with almost no storage in liver cells, and trace amounts of albumin are present in all extracellular fluids.
Functions:
(1) Maintains the constant colloid osmotic pressure of plasma, preventing edema.
(2) Plasma albumin can reversibly bind to many insoluble small organic molecules and inorganic ions, forming soluble complexes, becoming the transport form of these substances in the blood circulation. Thus, albumin is a non-specific transport protein, which is physiologically significant and closely related to human health. Human serum albumin is suitable for the prevention and treatment of hypoproteinemia, treatment of edema or ascites caused by liver cirrhosis and kidney disease.
(3) The content of albumin in plasma is far greater than that of globulins, and its hydrophilic action is also greater than that of globulins, which allows plasma albumin to provide a colloidal protective stabilizing effect on globulins. When liver dysfunction leads to insufficient synthesis of albumin, it can cause plasma globulins to lose their colloidal protective effect, leading to decreased stability. The decreased stability of plasma globulins will severely affect their metabolism and utilization in the body, causing corresponding symptoms. Moreover, albumin is also an important nutrient in the human body. Albumin is continuously metabolized in plasma, and amino acids produced from the breakdown of plasma albumin can be used to synthesize tissue proteins, oxidized to supply energy, or converted into other nitrogen-containing substances. Active hormones or drugs can bind to albumin and may not exhibit their activity, serving as their storage form. Due to the reversibility of this binding and the dynamic equilibrium, it plays an important role in regulating the metabolism of these hormones and drugs. At the same time, albumin is a viscous, colloidal substance that automatically binds to heavy metal ions when encountered in the body, allowing for their excretion from the body, thus playing a detoxifying role. Therefore, consuming foods rich in albumin can prevent the absorption of heavy metal ions and poisoning. Albumin also has a protective effect on the gastric wall.
Human serum albumin is a blood product, commonly referred to as “life product” or “life-saving medicine”. It is extracted from the plasma of healthy human bodies through a low-temperature ethanol protein separation method and treated for virus inactivation. Clinically, it is mainly used for the treatment of shock caused by blood loss, trauma, and burns, as well as for critical conditions such as edema or ascites caused by liver cirrhosis and kidney disease, and for patients with hypoproteinemia.
Alright, this concludes the popular science on test reports or drugs containing the word protein. If you have any further questions, you can only scan the QR code below to consult Dr. Chen or Director Guo:
Online Consultation Channels and QR Codes
Below is Dr. Chen Zeyu’s online consultation QR code. You can consult once or subscribe monthly (600 yuan/month, will the price increase after this article is published?  ):
):
Below is Director Guo Zhongjie’s “Guo Zhongjie”, “Sheng Bei” (including online consultation channels, 288 yuan/48 hours) public account; scan or long-press to identify the QR code to follow:


“Conference Notice”, Guo Zhongjie serves as the executive chairman of the conference: 7.6-7 Chengdu: The First Multidisciplinary Diagnosis and Treatment Progress and Hotspot Forum on Recurrent Miscarriage in Sichuan Province in 2019

(Welcome to provide more conference information, word version or pdf version or H5 version URL, send to email: [email protected], email subject marked: time + city + conference theme)
Highly Recommended Reading
【Highly Recommended】Comprehensively Understand Knowledge Points Related to Pregnancy Failure, Avoid Detours, and Quickly Have a Baby! (Collecting the essence of articles from the “Tianluan Help” public account)
● Recently, the pregnancy preservation field is very popular! Crossing boundaries? Moral integrity? Medical ethics? Since it is difficult to conduct controlled experiments, let’s work hard to carry out clinical medical real-world research!
● Non-classical phospholipid antibodies have clinical significance in the diagnosis of obstetric antiphospholipid syndrome (APS)
● Grateful that they remember us! They successfully held babies, and also helped us fulfill our dreams!
● Are babies born after immune preservation healthy? Let’s look at the long-term follow-up data of 547 patients with adverse pregnancy after preservation and delivery.
● Three generations of test tubes are not a guarantee; there are capabilities and limitations!
● Doctor, do I have lupus? Hurry up and learn how to interpret lupus anticoagulant reports!
● Is HCG falsely low after medication for early pregnancy preservation? What is the level?
● All knowledge about thromboelastography is here!
● If there is vaginal bleeding after preservation, don’t panic; read this article before saying anything!
● Understand T cell cytokines, serum cytokines, regulatory T cells (Treg), and lymphocyte subpopulations in one article
● Repeated natural miscarriage, should we preserve or not? (Continuation)
● New perspectives on the diagnosis and treatment of infertility in polycystic ovary syndrome (PCOS) from both Chinese and Western medicine
● What is biochemical pregnancy? A crisis? This crisis must be resolved before pregnancy!
● How to prevent pregnancy VS how to get pregnant immediately!
Master of Tianluan Help, male, non-doctor, due to my partner’s experience of three fetal arrests and successful preservation in the fourth pregnancy, established this account to help more families with similar experiences avoid detours. All articles and materials published or saved in this account are based on self-study, collection, organization, and publication. Thank you for your attention and support!
“Tianluan Help” Function Introduction
1. Appreciation Feedback
Follow the “Tianluan Help” public account and enter “Appreciation” to learn about the rules for appreciation feedback or click the “Read Original” at the bottom left to get the most suitable diagnosis direction and plan based on your medical history and geographical location (not involving dosage, treatment duration, etc.) or cross-regional treatment strategies, allowing you to avoid detours and save time! You will also be helped to join the most suitable WeChat interactive group (at least 4).
Please add the assistant’s WeChat proactively after appreciation if you need a one-on-one chat and take a screenshot to inform; those who do not proactively contact will be regarded as pure appreciation without the need for a one-on-one chat. Long press to identify the QR code below to appreciate!

2. Join Patient Groups
Click here to read: Join groups to chat about experiences, exchange strategies, and help sisters who have experienced adverse pregnancies to avoid more detours: 190511 version “Tianluan Help” patient WeChat group rules, group selection, and joining guidance
3. Selected Original Articles by the Master
Follow the “Tianluan Help” public account and enter “Original” to get more lists of original articles by the master and read them carefully. Or visit the menu bar at the bottom of the public account to access【Illiteracy Zone】 for reference.
4. Other Keywords
Enter the names of various provinces such as Beijing Shandong Guangdong Shanghai Hubei Chongqing Heilongjiang …… etc., to obtain corresponding information on pregnancy preservation warriors and soldiers in those provinces (constantly updated).
Other keywords include the names of pregnancy preservation warriors, hospitals’ abbreviations, testing items, conditions, pregnancy preparation, and brands or names of pregnancy preservation medications, which can be input in the dialogue box to obtain corresponding texts and images.
5. Access the Menu Bar (Completely Redesigned!)
If the keywords entered do not match, it may be due to excessive input or typos, or the master has not set them yet. You can directly access the corresponding sections of the menu bar at the bottom of the public account. You can read and learn at your convenience! If you don’t understand in one go, read it several times!
ClickRead Original to view the appreciation rules
Advertisements at the end of the article are pushed by WeChat officials, feel free to visit
When reprinting original articles from this account, please indicate that it is from “Tianluan Help“