
Introduction
Antibody-drug conjugates (ADC) therapy has rapidly developed over the past few decades, with 14 products approved globally and over 140 ADCs currently in clinical trials. By 2030, the ADC market is expected to exceed $15 billion. The basic principle of ADCs is that by combining the specificity of monoclonal antibodies with the cytotoxicity of effective small molecule drugs, ADCs can accurately deliver toxins to tumors while sparing normal tissues, thus increasing the therapeutic window of the drugs.
Preclinical data indicate that coupling drugs with antibodies can reduce the minimum effective dose (MED) and increase the maximum tolerated dose (MTD). However, increasing clinical evidence suggests that the tolerated dose of ADCs does not significantly differ from that of the related small molecules. After standardizing for the cytotoxic content, the MTD of ADCs is roughly equivalent to that of the corresponding small molecules in humans. Therefore, the general understanding of the ADC therapeutic window may currently be inaccurate. Here we explore several questions regarding the ADC therapeutic window, hoping to provide some insights that could aid in improving the design of the next generation of ADCs.
Can ADCs Really Achieve Higher MTDs Than Small Molecules?
The MTD of a drug is the highest tolerated dose without serious side effects (dosing-related toxicity). In the past, determining the MTD was a primary goal of phase I tumor trials. Recently, especially for new targeted therapies (including ADCs), the focus has shifted to determining the recommended phase II dose (RP2D) that better observes chronic toxicities and certain grade 2 side effects that may arise after multiple treatment cycles.
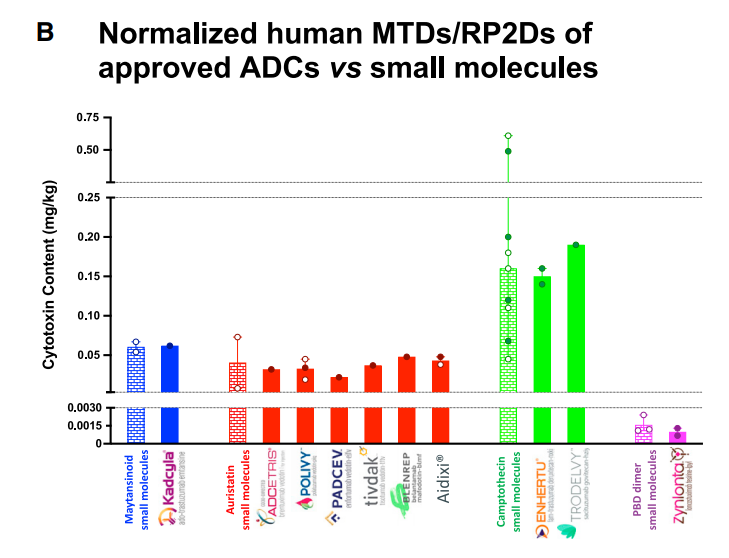
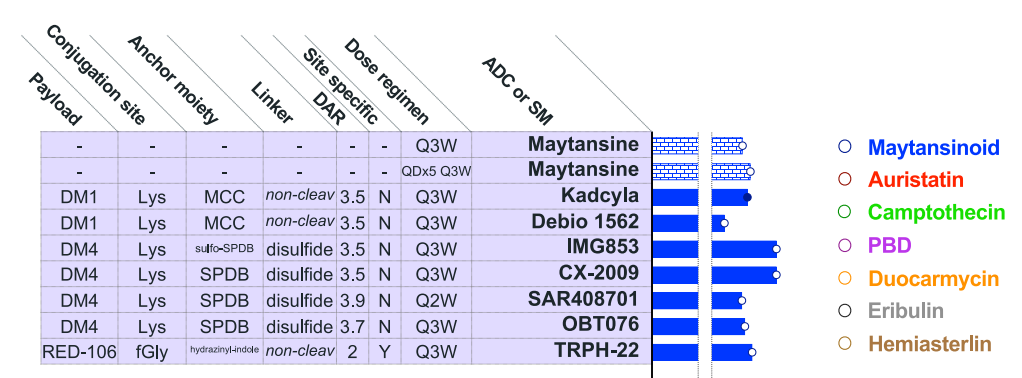
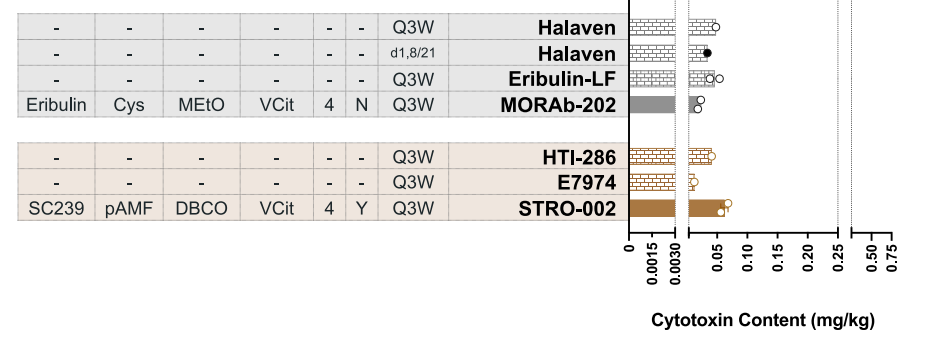
The above figure summarizes the MTD/RP2D values of 10 approved ADC drugs. By converting the doses of ADCs and small molecules into common units, one can standardize molecular weights and drug-antibody ratios, allowing for a more accurate comparison of the therapeutic windows of ADCs and effective payload small molecules. The results are clear: ADCs do not significantly enhance the MTD of their effective payloads. This understanding may help clarify several existing observations in the field:
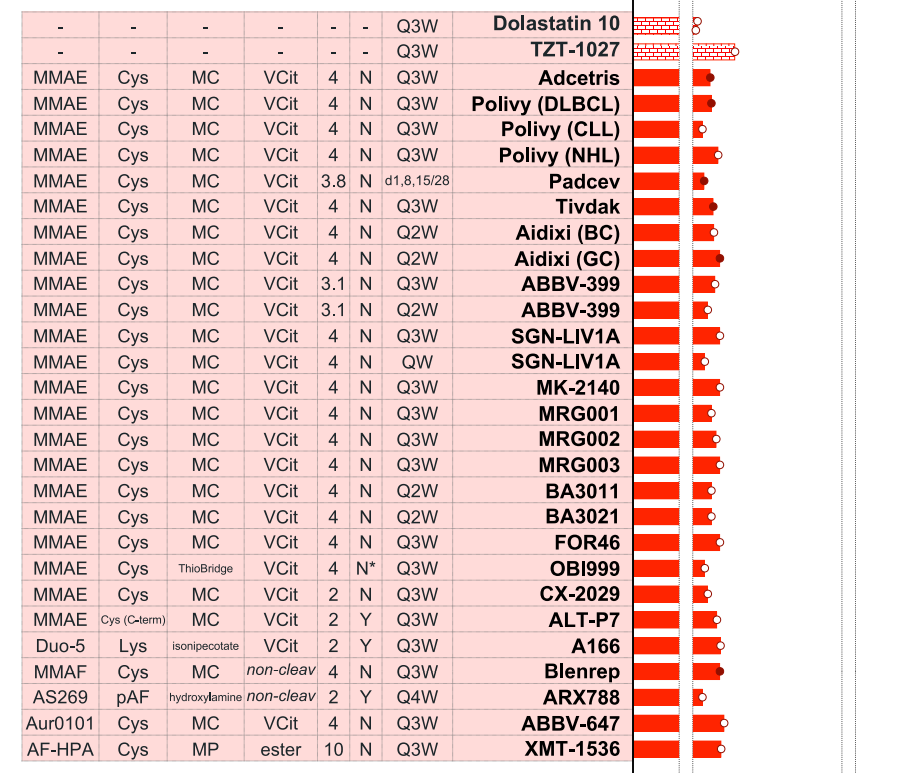
(1) ADCs with common effective payload-linkers typically encounter similar MTDs because the toxicity associated with the effective payload is platform-related and unrelated to the target antigen. This highlights that most non-targeted adverse events are unrelated to the antibody.
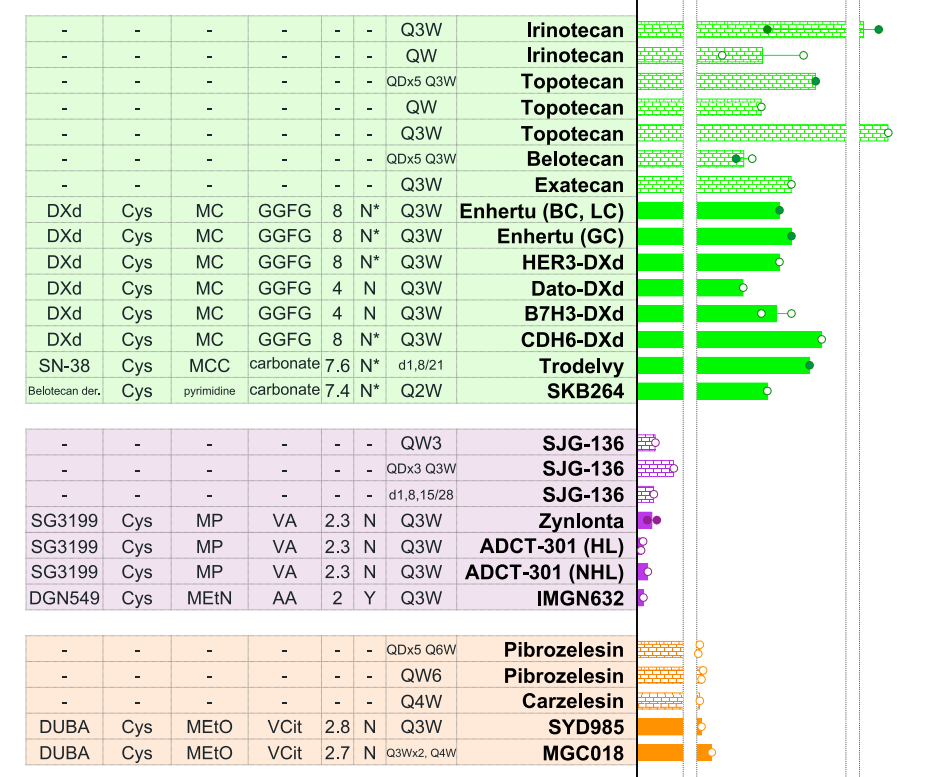
(2) Targeted non-tumor toxicity resulting from antibody binding in normal tissues is relatively common. In such cases, the MTD may be lower than that of other ADCs using the same effective payload-linker. For instance, Dato DXd (the DAR4 DXd ADC targeting TROP2) failed to achieve the same cytotoxic dose as other ADCs containing DXd (T-DXd, HER3-DXd, B7H3-DXd, and CDH6-DXd), possibly due to drug-related adverse events caused by TROP2 expression in normal tissues (rash, stomatitis, and mucositis). Similar toxicities were also observed in patients treated with other TROP2 ADCs.
(3) Engineering ADCs with designed limitations for binding to normal tissues (e.g., CX-2009, CX-2029, BA3011, BA3021) did not improve MTD compared to conventional ADCs with the same effective payload-linker.
(4) In some cases, reducing the DAR of ADCs leads to a proportional increase in the tolerated ADC dose, but there is little improvement after standardizing for the cytotoxic content. For example, ALT-P7 (DAR2 MMAE ADC) has a similar MTD compared to other DAR4 MMAE ADCs. Correspondingly, B7H3 DXd (DAR4) shows no difference compared to other DAR8 DXd ADCs.
Although somewhat surprising, ADCs were previously widely believed to broaden the therapeutic window of their effective payloads. However, clinical data clearly show that the MTD has not increased. This is further corroborated by clinical data from nearly 40 active ADCs.
Why Is There No Significant Change in MTD for Effective Payloads and ADCs?
The reasons ADCs have failed to improve the MTD of their effective payloads remain unclear. One possible explanation lies in the critical role antibodies play in protecting effective payloads from clearance and metabolism. The effective payload “full dose” is attached to the antibody until ADC-mediated targeted and non-targeted cellular uptake occurs, leading to the release of free effective payloads or effective payload metabolites, which are then cleared through traditional small molecule pathways.
ADC effective payload-linkers can also undergo extracellular cleavage in plasma or tumor microenvironments, providing a direct source of effective payloads in circulation without the need for endocytosis. While newer ADCs use more stable linkers than previous generations, some effective ADCs (including approved ADCs) are constructed using linkers with relatively short half-lives in plasma.
Furthermore, ADCs prepared through thiol-maleimide chemistry, including most ADCs currently approved or in development, may allow the entire effective payload-linker to decouple from the antibody, a process known as the reverse Michael reaction. For instance, T-DXd and other deruxtecan ADCs, vedotin ADCs, and many ADCs under development. For these ADCs, up to 50%-75% of the effective payload-linker is decoupled after approximately 7 days, and the decoupled effective payload-linkers rapidly react with plasma molecules containing thiols (primarily albumin), forming new conjugates. Albumin has a long half-life in humans, so effective payloads are not released into circulation immediately but remain in the blood until the albumin conjugates are broken down. The transfer of effective payload-linkers from ADCs to albumin may contribute to certain toxicities through the nonspecific deposition of albumin conjugates and increased effective payload half-lives. On the other hand, it may also assist in antitumor effects by being directly absorbed by tumors through albumin conjugates. However, due to the biological differences of albumin in preclinical models compared to humans, assessing the role of albumin in toxicity and efficacy related to effective payload-linker decoupling remains challenging.
Does ADC Efficacy Exceed That of Its Effective Payload?
So far, the 14 approved ADCs have demonstrated the significance of the ADC therapeutic approach, with the latest data from DESTINY-Breast03 and DESTINY-Breast04 highlighting the potential of T-DXd to change the treatment paradigm for breast cancer. On the other hand, over 100 terminated ADC projects have also shown the challenges of selecting the correct combination of antibody, target, effective payload-linker, DAR, and indication.
In the 1970s, FDA cancer drug approvals were primarily based on objective response rates (ORR), but since the early 1980s, approvals have been based on more direct clinical efficacy evidence, including improvements in progression-free survival (PFS) and overall survival (OS). Because ORR is directly attributable to drug effects, it is also the most common surrogate endpoint supporting FDA accelerated approvals. Given that ORR is typically used as a primary endpoint in early ADC trials, here we compare the ORR of small molecules and ADCs when treating similar patient populations.
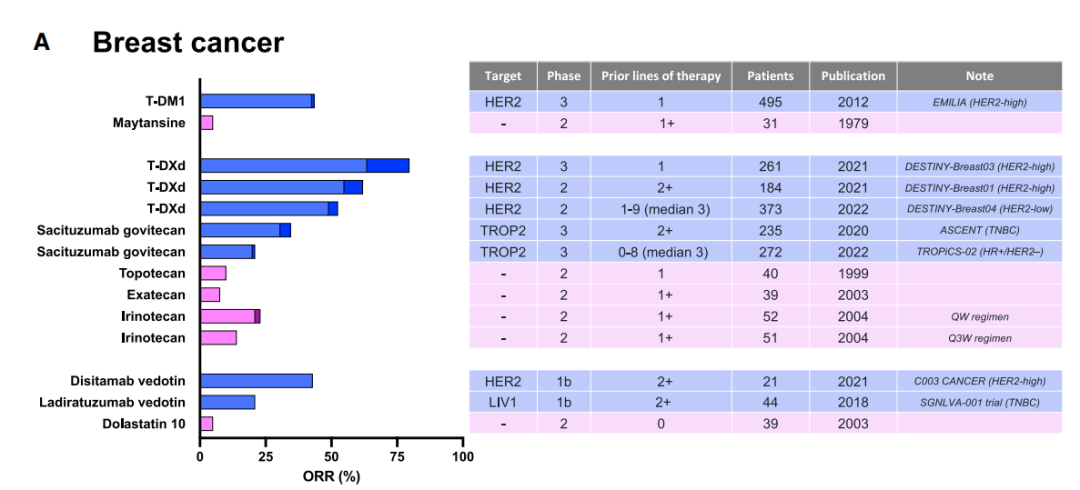
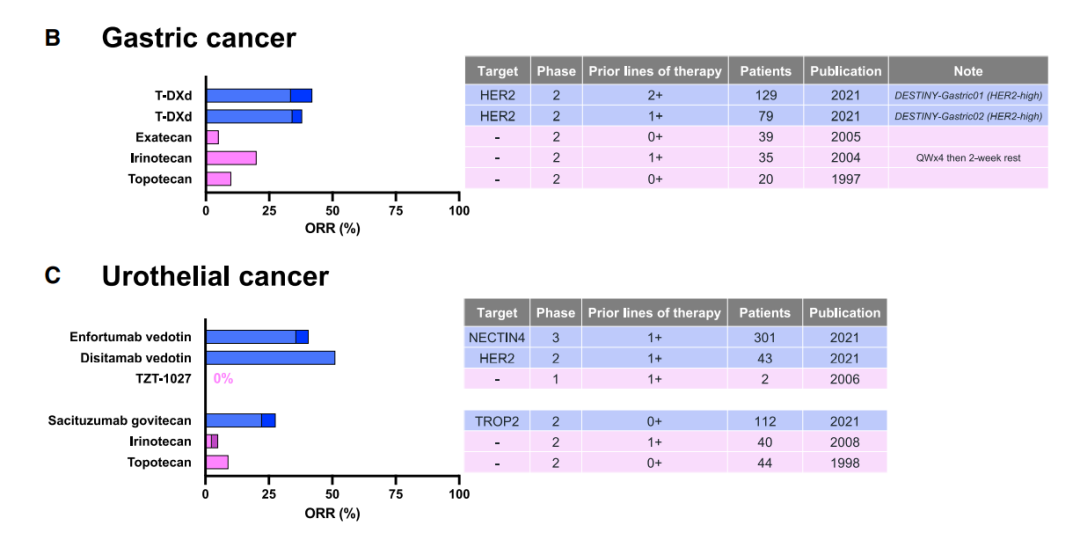
To date, there have been no direct head-to-head randomized clinical trials comparing ADCs with their effective payloads. The closest example is the T-DXd treatment group in the physician’s choice arm of the DESTINY-Gastric01 trial, where the ORR was 42% for the T-DXd treatment group compared to 12.5% for the physician’s choice group. There is enough clinical data to conclude that multiple ADCs demonstrate better ORRs than related small molecule therapies.
What Mechanisms Contribute to ADC Success?
The pharmacokinetics (PK) of small molecules fundamentally change when conjugated with antibodies. ADCs extend the half-life of cytotoxic agents, including protecting them from renal clearance. On the other hand, ADCs face similar issues as other biologics, including significant non-tumor-targeted uptake and nonspecific clearance, limited extravasation due to capillary wall constraints, low diffusion within tumors due to increased interstitial fluid pressure, and the “binding site barrier” phenomenon (the antibody binds to its target faster than it diffuses, preventing deeper penetration). For monoclonal antibodies, some of these obstacles can be overcome by increasing the dose; however, this strategy is not applicable to ADCs because the conjugated cytotoxic agent determines the MTD. In fact, it has been reported that less than 1% of ADCs reach human tumors, with the remaining ADCs potentially causing unnecessary toxicity. Therefore, relying solely on ADC tumor targeting may not explain the observed efficacy improvements over related small molecules.
Thus, ADCs may depend on other mechanisms to enhance efficacy, such as effectively prolonging the release of effective payloads in circulation. Antigen expression and ADC characteristics influence ADC PK and metabolism, regulating the rate and location of effective payload release, which in turn affects free effective payload plasma levels and local tumor concentrations. Among these, the degree of effective payload bystander activity, conjugation chemistry, and linker type are key design parameters.
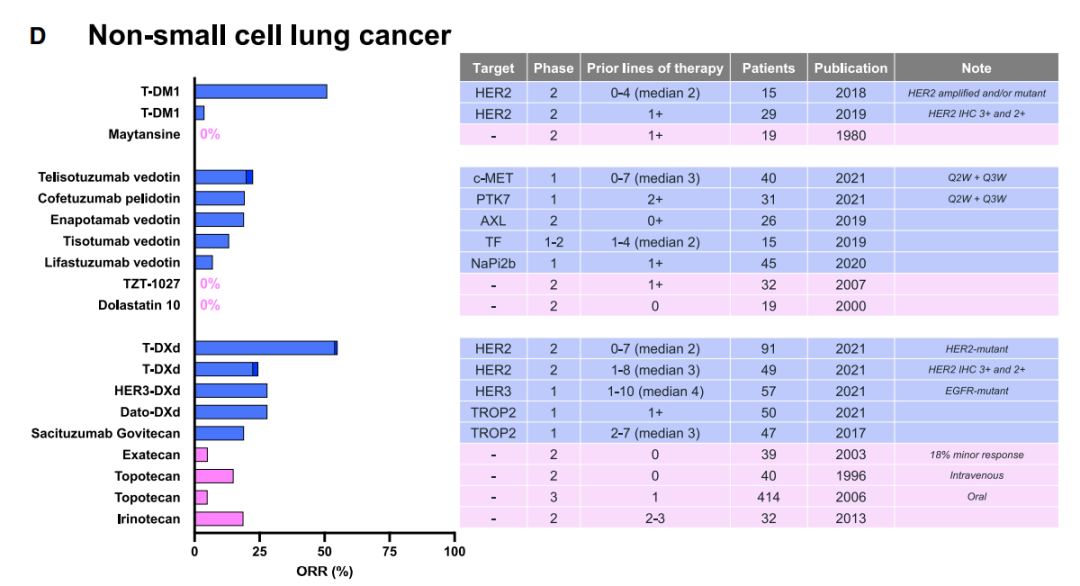
Furthermore, recent clinical results from patients with varying tumor antigen expression levels support the notion that circulating effective payloads can produce baseline anti-tumor effects. For example, many ADCs have shown efficacy in patients with low or negative tumor antigen expression. The antibody portion may enhance baseline activity potency provided by free cytotoxic agents, particularly in tumors with high antigen expression.
Comparing trial data from trastuzumab, T-DM1, and T-DXd in patients with brain metastases of HER2+ breast cancer reveals that in the subgroup analysis of DESTINY-Breast03, the intracranial ORR for T-DXd and T-DM1 were 64% and 33%, respectively, while trastuzumab alone did not produce an objective response in separate trials. The complete blood-brain barrier (BBB) prevents antibody penetration but does not restrict small molecules, depending on their physicochemical properties. Compared to trastuzumab, T-DXd (more permeable) and T-DM1 (less permeable) may best explain the observed differences in anti-brain metastasis activity due to the tendency of cytotoxic metabolites in circulation.
Conclusion
The success of ADCs demonstrates that the correct combination of target, antibody, conjugation method, DAR, linker, effective payload, and disease indication can yield significant clinical benefits. However, despite the wide diversity, current ADCs have not significantly increased the MTD of their effective payloads across various tumor disease states. Therefore, a better understanding of the mechanisms of action of clinically active ADCs, such as antibody-targeted delivery, sustained free drug concentrations in circulation, albumin transfer, or combinations of various mechanisms, as well as the interplay between ADC structural components and their PK/PD, is crucial for designing the next generation of ADCs.
Understanding ADC Drugs in One Image
After the era of chemotherapy, targeted therapy, and immunotherapy, ADC drugs, which couple cytotoxic drugs with targeted monoclonal antibodies, have opened the fourth tier of tumor treatment with outstanding results. They have now become a new class of drugs that cannot be overlooked in cancer treatment both domestically and internationally.
So, what are ADC drugs? Source: Medical Vision.
Researchers have found that certain tumors contain a special type of cancer cell, such as those that highly express human epidermal growth factor receptors 2 or 3 (HER2/HER3),TROP2, etc., and these cancer cells spread and grow faster than other cancer cells. Today, we take HER2 as an example to examine the mechanism of action of ADC drugs.

Currently, ADC drugs show excellent clinical efficacy in breast cancer, gastric cancer, urothelial carcinoma, lung cancer, and hematological malignancies, demonstrating that through technological innovation, drug properties can be combined under the traditional thinking of chemotherapy, targeted therapy, and immunotherapy, allowing previously “useless” targets to be fully repurposed, leading to a new round of drug breakthroughs, new hopes, and new dawns!
References:
1. The therapeutic window of antibody drug conjugates: A dogma in need of revision. Cancer Cell. 2022 Oct 10; S1535-6108(22)00445-7
Friends who like our articles, please give a“Like” and“Share”, otherwise, due to changes in WeChat push rules, you might miss us every day~
Disclaimer
“Gathering Southern Medicine” The public account reposts articles from other public platforms, mainly to share industry-related knowledge and convey the latest information. The copyright of images and articles belongs to the original author. If there is any infringement, please inform us in the comments, and we will delete the relevant information within 24 hours.
Information Source:Original Xiao Yao Talks Medicine
 Previous Recommendations
Previous Recommendations



This platform is not responsible for the views expressed in reposted articles, nor does it provide any express or implied guarantees regarding the accuracy, reliability, or completeness of the content included in the articles.