Introduction
This article describes the development history of the Da Vinci surgical robot from the early days of Intuitive Surgical to 2009. It also summarizes the origins of remote surgery, including unique technological trends and clinical needs, and introduces pioneers who profoundly understood robotics and remote technology and applied them in healthcare. In this section, we describe some important equipment regulations and their impact on the development of medical devices. However, it should be noted that these views come from Intuitive Surgical and are not detailed enough; nonetheless, we hope these perspectives can provide insights into technological and medical development and innovation, ultimately benefiting humanity.
The Origins of Remote Surgery
Remote surgery emerged from the intersection of two very different technologies, achieving a completely innovative minimally invasive surgery. The first technology dates back to the “remote operation” concept from the 1940s. Robert A. Heinlein wrote a short science fiction story titled “Waldo” in 1942, describing a character named Waldo Farthingwaite-Jones, who was born weak (unable to stand) and could use his hands and fingers to operate a remote-controlled glove to control a powerful robotic arm. Not long before, a remote manipulator called “waldoes” was designed to handle dangerous radioactive materials. These devices used cables to drive joints, allowing operators to safely handle hazardous materials from behind protective glass. In the 1950s, Raymond Goertz and his colleagues researched remote manipulators that could operate at greater distances, replacing mechanical structures with electric sensors and drivers, thus allowing operators to be physically far from the “hand,” greatly expanding the uses of remote operation.
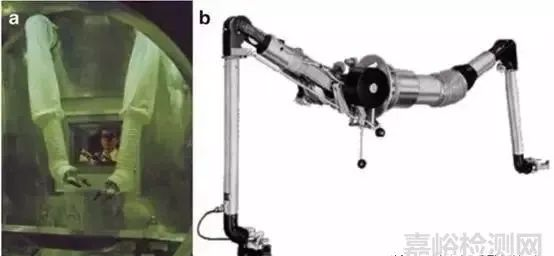
▲ Figure 9.1 Mechanical remote manipulators operating in hazardous environments. The model on the right is from Central Research Laboratories.
In the medical field, the idea of applying endoscopes can be traced back to an Arab physician named Albukasim (936–1013 A.D.). However, it wasn’t until the 19th century that Phillip Bozzini invented practical methods for observing the insides of living human bodies. He used an instrument he named “Lichtleiter” to observe the urinary system, rectum, and throat. Endoscopic devices continued to develop until around 1980 when the advent of CCD and video devices revolutionized the field and led to the development of minimally invasive laparoscopic techniques, marked by the first laparoscopic cholecystectomy completed by French physician Mouret in 1987.
Before the emergence of remote minimally invasive surgical robots, several other key technologies appeared. Remote operation technology was further developed in applications involving hazardous materials, deep-sea exploration, and space exploration. In the 1980s, microelectronics and computing power advanced rapidly, and virtual display technology (VR) began to introduce concepts of environmental immersion, such as head-mounted displays (capable of vividly and flexibly showcasing 3D worlds) and haptic interactions. Around 1990, laparoscopic surgery experienced rapid development, but the application of this technology was limited. Laparoscopic surgery found widespread application in relatively simple procedures such as laparoscopic cholecystectomy, oophorectomy, and simple hysterectomy. However, laparoscopic surgery failed in complex reconstructive surgeries, leading to the emergence of complex mechanical medical devices such as staplers and other tissue suturing devices, which still could not facilitate laparoscopic surgery in complex operations.
In around 1990, several research teams began exploring the potential of combining remote operation with virtual displays. These groups studied the shortcomings of laparoscopic minimally invasive surgery and realized that remote robots could develop and apply in this area. Below are some teams that first began researching the combination of remote robotic technology with minimally invasive surgery, whose research results ultimately influenced the development of the Da Vinci surgical robot:
Dr. Russell Taylor and his team, who, while at IBM’s Watson Research Center, collaborated with a general surgeon from Johns Hopkins University, Dr. Mark Talamini, to develop a laparoscopic robotic-assisted system called “Third Hand” (LARS), which allowed surgeons to control an endoscope using a joystick.
At the University of California in Santa Barbara, Dr. Yulun Wang developed a robotic system for NASA, which he later used in 1992 to control an endoscope during laparoscopic surgery, leading to the creation of the Automated Endoscopic System for Optimal Positioning (AESOP). This project was jointly advanced by Dr. Wang and Dr. Carlos Gracia from San Ramon Regional Medical.
At MIT, Professor Kenneth Salisbury and his students innovatively developed human-computer interaction and haptic feedback systems. One of his students, Dr. Akhil Madhani, developed the “Black Falcon” system, a remote force feedback system equipped with surgical instruments during his doctoral work. An alumnus from Salisbury’s lab, David Brock, and Dr. Gary Rogers from Boston University Medical Center co-founded a company in 1996 called Brock–Rogers Surgical.
Dr. Hari Das from the Jet Propulsion Laboratory (Pasadena, California) collaborated with ophthalmologist Steve Charles, and with NASA’s support, their surgical robot, Robot Assisted Microsurgery (RAMS), also made achievements in the fields of remote operation and minimally invasive surgery.
Professor Brian Davies and his team from Imperial College (London, UK) developed surgical robots for prostate and neurosurgery, and their I.C. PROBOT prostate surgery robot underwent trials in the early 1990s.
Professor Blake Hannaford and his team from the University of Washington (Seattle, Washington) conducted experiments and research on remote operation and haptic feedback in the mid-1990s.
Phil Green from SRI International (Menlo Park, CA) and Dr. John Bowersox from Stanford University, who was also a military doctor, developed the “telepresence surgery system,” which had a critical impact on the early prototypes of da Vinci.
Early Funding Sources
Several early remote robotic surgery projects were funded by military funds. Dr. Richard Satava from the Defense Advanced Research Projects Agency (DARPA) was very interested in the use of surgical robots on the battlefield and provided funding for remote robotic projects in the early 1990s. The SRI team initially secured internal funding and later received grants from the National Institutes of Health (NIH), eventually starting to obtain funding from DARPA. Dr. Yulun Wang received seed funding from DARPA to study his early voice-controlled mechanical imaging arm, and Dr. Salisbury’s team at MIT also received funding from DARPA.
The goal of remote surgery was to provide immediate assistance to injured soldiers on the front lines while doctors could operate safely from the rear. During the Iraq War, this method of frontline surgery became a way to stabilize casualties quickly and evacuate them, but the DARPA funds played a significant role in supporting early remote surgery research.
History of Intuitive Surgical
In 1994, Dr. Frederick Moll became interested in SRI’s remote robotic systems. Guidant tried to gain venture capital, and in 1995 he was introduced to Rob Younge, a co-founder of Acuson Corporation. Fred Moll, Rob Younge, and John Freund co-authored a business plan and successfully secured the first investment for Intuitive Surgical Devices.
Intuitive Surgical obtained licensing for remote surgical robot technology from SRI and began recruiting engineers. In April 1996, an engineering team was formed, and over the next three years, they developed three generations of robotic prototypes, conducting animal and human trials, ultimately launching Intuitive Surgical’s core product: the da Vinci surgical system. During this development process, new technologies and personnel from other teams continuously joined, such as Dr. Russell Taylor’s team from IBM and Dr. Ken Salisbury’s team from MIT.
While waiting for FDA approval, Intuitive Surgical began selling the da Vinci surgical system in the European market. In June 2000, Intuitive Surgical raised $46 million through a public offering, and a month later received FDA approval for use in general surgical procedures. In 2001, the FDA approved the da Vinci surgical system for use in thoracic surgery indications and radical prostatectomy indications.
Before the public sale of the da Vinci surgical system in 2000, Intuitive Surgical was sued for patent infringement by its competitor Computer Motion, which had released the Zeus surgical system in 1997. The Zeus system was an upgraded version of the AESOP system, which was the first voice-controlled surgical robot endoscope control system to receive FDA approval, aimed at providing laparoscopic surgeons with a higher quality and stable view. The concept behind the da Vinci surgical system was slightly different; it aimed to provide surgeons with an experience similar to open surgery using minimally invasive techniques.
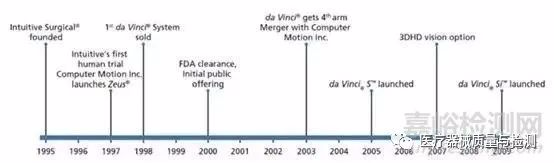
▲ Figure 9.2 History of Intuitive Surgical (up to 2009)
To achieve this goal, the da Vinci system needed to provide 3D stereoscopic vision inside the human abdomen and intuitive dexterity in operation. The difference was that the da Vinci system targeted the previous open surgery market, while the Zeus system primarily focused on the laparoscopic surgery market. Initially, the Zeus system was accepted by general laparoscopic surgeons, while the da Vinci system was accepted by surgeons with experience in open surgery. Relatively speaking, the Zeus system was smaller and cheaper but performed worse, while the da Vinci system was large and often criticized for being over-engineered. However, by 1999, Computer Motion began to shift towards Intuitive Surgical’s design philosophy.
When Computer Motion filed a lawsuit, Intuitive Surgical also initiated a counterclaim, leading to an endless legal battle between the two inexperienced startups, which limited the development of both companies. In 2003, as both companies were nearly out of funds, they agreed to merge and end the litigation. From then on, the Zeus system was gradually replaced by the more functional da Vinci system.
The Development History of the da Vinci Surgical System
At the beginning of product development, Intuitive Surgical established four key design principles. The first and most important was that the system needed to be highly reliable and have failure protection to ensure the feasibility of a surgical device; second, the system needed to provide intuitive control of instruments to the surgeon; third, the instrument tips needed to have flexible six degrees of freedom; and fourth, the system needed to offer realistic 3D visual effects (3D endoscopy). These design principles ensured that the system could restore the capabilities lost by surgeons during conventional laparoscopic surgery, with the above technologies coming from SRI, IBM, and MIT.
In 1995, the prototype designed by SRI had four degrees of freedom for instruments (including tip opening and closing), using a master controller to intuitively control the motion of the instrument tips. The mechanical similarities between the master and slave hands simplified the calculations for master-slave control. Based on this generation of prototypes, three more generations were developed within three years, ultimately resulting in the da Vinci system being launched for sale.
The da Vinci system was named early in Intuitive Surgical’s establishment. Leonardo da Vinci, a representative figure of the Renaissance, combined art, science, anatomy, and engineering in his inventions and innovations, which seemed to align well with Intuitive Surgical’s vision. The early prototypes were not called da Vinci because that name was reserved for the product.
The Lenny Prototype
The first generation prototype was improved based on the SRI prototype, increasing the degrees of freedom at the patient-end manipulator (from 5dof to 7dof), although the instruments were still not interchangeable. The similarity of the master-slave mechanisms was retained. The patient-end manipulator was mounted on a simple positioning platform and could only be adjusted using a screwdriver and wrench.
To visualize the operation interface, the prototype directly used a commercial 3D endoscope from Welch Allyn, installed on a robotic arm similar to the SRI prototype. This endoscope’s CCD provided images with a resolution lower than the NTSC standard definition video, but offered stereoscopic vision that allowed users to sit while using it. The visual system utilized commercial stereoscopic glasses to display the 3D images obtained from the Welch Allyn 3D endoscope, using shutter-type stereoscopic glasses.
The Lenny prototype was completed in the summer of 1996 and underwent animal testing, designed for complex general surgical procedures. The experiments demonstrated that increasing the wrist’s six degrees of freedom made the instrument control more intuitive, justifying the added complexity in design. However, from another perspective, the Lenny prototype was fragile and unreliable, and its visual system was cobbled together. Moreover, this prototype proved that a structure must be designed for the patient-end manipulator that allows for easy adjustment and positioning. The Lenny prototype was used for about 6-9 months, but it provided crucial research directions for the next generation of prototypes.
The Mona Prototype
Based on the experiences gained from Lenny, significant changes were made to several robotic subsystems, leading to the Mona prototype. The name is derived from Leonardo’s famous painting: the Mona Lisa, and this prototype underwent human trials.
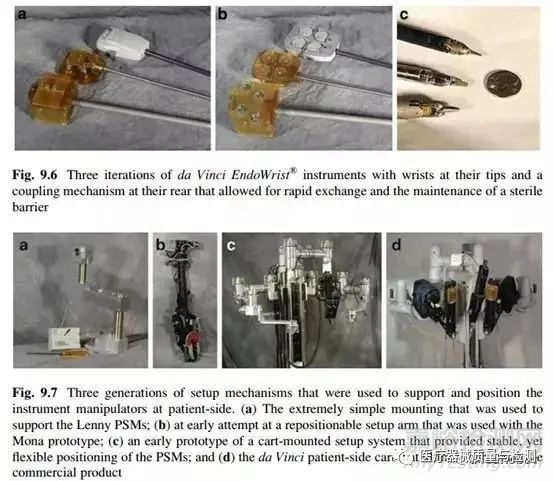
The most significant aspect of the Mona system was the redesign of the patient-end manipulator, achieving a replaceable sterile instrument structure. This was lacking in the Lenny prototype and was a necessary design for applications in humans. This replaceable instrument design ensured that different instruments could be swapped out according to various surgical needs and that instruments could be removed from the sterile robot for disinfection. The design of the instruments adopted a low-friction rope pulley scheme, which was significantly influenced by Kenneth Salisbury’s team from MIT.
Another meaningful improvement was the positioning mechanism at the patient-end. The Mona system designed a flexible adjustment mechanism (adjustment arm) composed of gears, springs, and rods, which was locked onto a guide rail and could dynamically counteract the movements of the manipulator. Two such mechanisms were installed on one side of the platform, and a third was installed on the opposite side. A portion of this mechanism is shown in Figure 9.7b.
In the first half of 1997, Intuitive Surgical used the Mona prototype to conduct the first human surgical experiment at Saint-Blasius Hospital. This experiment demonstrated the clinical value of the robot but also highlighted areas for improvement:
Interchangeable instruments were extremely significant improvements; the precision requirements for the instruments and the patient-end manipulator were very high, and poor accuracy could lead to unreliable connections between the two;
Enhancements in visual quality during master-slave interactions revealed that both image information acquisition and display quality were inadequate, lacking clarity and comfort;
Perhaps the most unsatisfactory aspect of the Mona prototype was the operation of the adjustment mechanism, which was found to be unstable and inflexible, and too heavy. Thus, fundamental improvements were needed for the adjustment mechanism.
The da Vinci System
The early experiments with the Mona prototype exposed the shortcomings of the patient-end robot’s positioning, which was not flexible and stable enough. Consequently, engineers began to focus on resolving the adjustment arm issues, initially building models with toothpicks, then using 1:8 cardboard models, and finally full-scale wooden models, creating several prototype designs before using metal machining. The adjustment arm prototype was mounted on a large, heavy cart, but ultimately achieved flexible and stable adjustment capabilities.
At this stage, the visual system’s deficiencies were the second most important issue. The stereoscopic visual system adopted a new approach, implementing a dual-display design instead of the previous single-display solution. Figure 9.8b shows an early prototype.
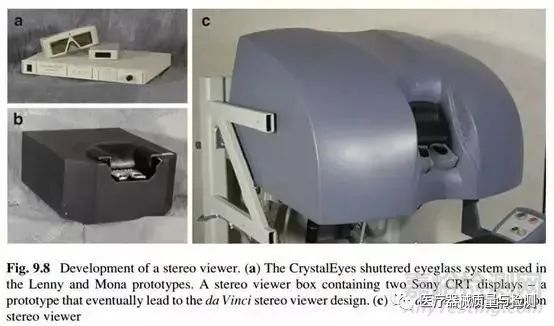
The da Vinci system’s stereoscopic visual system utilized two Sony CRT displays, employing mirrors to simplify the functions of the stereoscopic display system while enhancing image display quality and the depth and effects of the stereoscopic vision. To improve video quality, the da Vinci system adopted a design scheme of a single optical channel with dual cameras from Olympus (cameras at the end of the endoscope), replacing the previously low-resolution Welch Allyn endoscope. Although image quality improved, the stereoscopic effect remained unsatisfactory. Therefore, Intuitive Surgical entered into an agreement with Precision Optics Corporation (POC) to customize certain optical components, ultimately achieving a solution that installed a dual 5mm rod lens optical system within a 12mm endoscope, directing the images to a three-chip camera at the end of the endoscope.
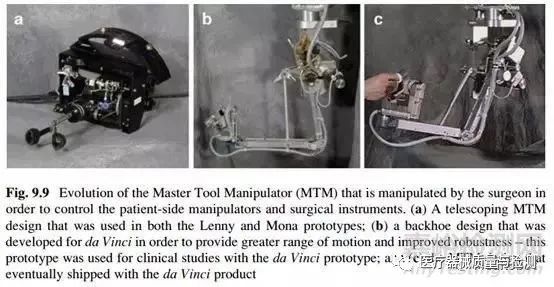
The issue of unreliable connections between instruments and robotic arms was resolved by applying a sliding coupler method, significantly reducing the mechanical precision impact at the instrument and platform interface. The main hand of the surgeon’s console also saw significant improvements; it transitioned from a telescopic design to a bucket-like structure, distinctly different from the slave hand’s configuration, greatly enhancing workspace and reliability.
By this stage, the system had matured sufficiently to deserve the name da Vinci, and the Intuitive team felt that this prototype was ready to be pushed to market as a product. Therefore, between 1998 and 1999, Intuitive Surgical conducted human trials of the da Vinci system in Mexico, France, and Germany, with clinical trial indications primarily focused on cholecystectomy, fundoplication, thoracoscopic access for chest arteries, and mitral valve repair. At this point, the adjustment arm issues had been resolved, and the system exhibited excellent 3D visual effects, with intuitive and dexterous control of surgical instruments, proving to be clinically valuable.
The four key product design principles mentioned above were ultimately proven to be extremely valuable. It took more than two years from the initial design of this robot, which exceeded the complexity of a car (approximately 10,000 parts), to the final delivery of the first product (in November 1998) to the Leipzig Heart Center in Germany. The first batch of orders consisted of ten units, intentionally limited because Intuitive Surgical, as an inexperienced new company, needed to learn how to manufacture products and provide product support. Figure 9.11.
Continuous Improvement and Research
From the sale of the first robot to the next four years, Intuitive Surgical focused on addressing reliability issues and expanding its production and sales teams. The product continued to improve after the sale of the first unit.
On the da Vinci platform, finer 5mm (instead of 8mm) instruments were developed. In 2003, the patient-end robot added a fourth mechanical arm, providing surgeons with greater surgical control (such as tissue retraction), while also adding the ability to switch control between different arms. At this time, the variety of surgical instruments had expanded from six to fifty.
The da Vinci S system was released in 2006, reducing preoperative setup time by half (cutting the preoperative adjustment steps in half) through ergonomic design, greatly enhancing the operating experience of the patient-end robot. The patient-end slave hand was improved to be smaller, lighter, easier to manufacture and maintain, and offered a larger range of motion. The fourth arm was better integrated into the design (rather than being awkwardly fitted in as in 2003). The surgical cart was also redesigned to be lighter and easier to adjust flexibly and simply. The distributed power and control system design greatly reduced cable lengths (power cables & steel cables). The visual system was upgraded to WXGA high resolution (1280*768 pixels, essentially achieving 720P), and adapted to the endoscope system. The patient-end robot added a touchscreen and TilePro system (image cart touchscreen system) to enhance interaction and control experience. Additionally, several meaningful improvements were made to enhance the robot’s reliability, fault tolerance, and accelerate the research and development speed.
The latest version of the da Vinci Si released in 2009 (followed by the da Vinci Xi and da Vinci X until 2017) focused on streamlining the platform to meet the mature market, while the previous generation product (da Vinci S) emphasized improvements to the patient-end robot. The da Vinci Si primarily enhanced the surgeon’s operating platform and image cart. Improvements included a more ergonomic design for the surgeon’s console, providing higher resolution 3D displays, routing all wiring for the main operator internally, and simplifying the user interface. Additionally, the foot pedals were modified to be smaller for easier operation by smaller nurses.
The video cart and endoscope were also modified: the touchscreen was changed to a widescreen format and supported higher resolutions (1440*900 pixels). Before the da Vinci Si, the endoscope controller and robot controller were separate, so when the operator wanted to complete a setup, they needed to adjust two control steps. The da Vinci Si integrated the visual control system, allowing for simultaneous adjustments to 3D visual information. Furthermore, the endoscope’s camera was made smaller for easier handling, and the setup steps for the image system were streamlined.
Finally, the da Vinci Si introduced a dual surgeon control console scheme, employing a “shared control” approach that allowed surgeons to jointly control the robot’s instruments, facilitating easier training and collaborative surgeries.
Regulatory Environment
In the United States, the regulatory body for medical devices is the Food and Drug Administration (FDA). In 1990, the Safe Medical Devices Act proposed that medical devices must demonstrate safety and effectiveness. Generally, medical devices are classified into three levels: Class I represents the lowest risk, followed by Class II, with Class III representing the highest risk. The classification hinges on the risks posed by the medical device to patients and users, including risks of intentional misuse. Class III devices are typically life-supporting equipment, such as cardiopulmonary support systems. Class II devices are those that could cause serious harm if misused or improperly used. Class I devices would not cause serious harm even if misused or improperly used.
As pioneers in computer-assisted surgery, Intuitive Surgical and Computer Motion were tasked with assisting the FDA in advancing the first registration of robotic medical products. One example is the classification of the da Vinci robotic system, which initially began as a Class III device but was later changed to Class II. Class II devices include those “remote-controlled” types of products, such as those used in aircraft and spacecraft, whose control signals rely on electromagnetic pulses from computers.
Over the past decade, the FDA regulators have worked diligently to understand these computer-assisted systems to facilitate their authorization for use. They have recently created some internal terminology to classify these special devices. The FDA has categorized computer-assisted systems into three major types. The first type is “stereoscopic vision positioning or magnetic positioning” systems, such as those used in computer-assisted thoracentesis systems, orthopedic navigation systems, and some stereotactic navigation systems for neurosurgery and radiation therapy. The second type is “remote-controlled flight” systems, which operate similarly to pilot systems, such as the da Vinci robot, which falls into this category. Devices capable of performing automated clinical surgeries are classified as the third type. Since most computer-assisted systems have received FDA approval within ten years, these terms are still primarily known within the FDA and industry.
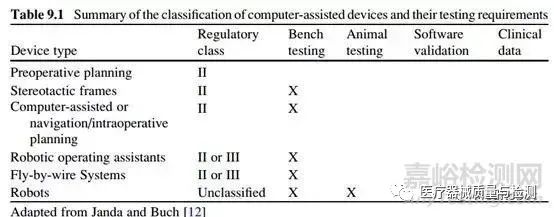
From the arguments above, it is evident that the registration path for a computer-assisted system with the FDA depends on the device’s structural composition, risks to patients and operators, and the risks of intentional misuse. Regulatory bodies issue opinions based on clinical data, simulated clinical environments, or appropriate animal testing data (bench-top), inspection and verification documents. A recent article by Janda and Buch summarized the classification levels of computer-assisted devices and the requirements for testing, design verification, and clinical data. While there will be disclaimers, Table 9.1 provides some guidance on the testing and clinical documentation requirements for computer-assisted medical devices entering the market.
Intuitive Surgical submitted the da Vinci surgical system to the FDA in 1997 under the name of a robotic endoscope control system. Initially, the da Vinci system was classified as a Class III medical device and required clinical data to demonstrate the system’s safety and usability (e.g., cutting, cauterizing, suturing, tying knots, etc.). Figure 9.3 illustrates the evolution of regulatory opinions regarding the da Vinci platform over ten years. This table does not include devices and accessories that went through the pre-market notification process. By 2009, Intuitive Surgical had submitted a total of 35 regulatory opinions regarding the da Vinci system platform to the FDA.
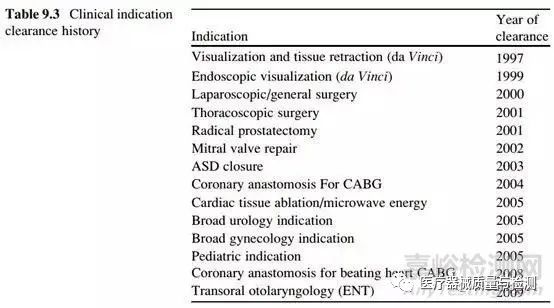
As mentioned above, FDA-approved Class II medical devices are specific to certain indications, and the FDA must confirm the safety and effectiveness of medical devices before approving their use. Table 9.3 describes the registration history of new clinical indications for the da Vinci surgical system. If the da Vinci surgical system wishes to obtain permission for new indications, it must submit clinical data proving the da Vinci surgical system’s safety and effectiveness, including anticipated clinical trials and analyses of past clinical data.
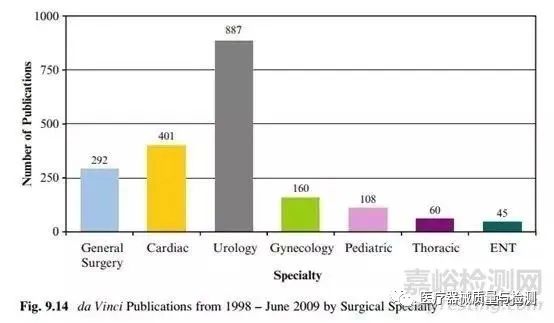
As government agencies seek to understand the output and costs of new technologies on public health, peer-reviewed clinical publications and evidence-based clinical practices have become increasingly important. Intuitive Surgical has tracked peer-reviewed articles related to the clinical applications of the da Vinci surgical system, with literature services indexing over 2000 articles showcasing the characteristics and advantages of the da Vinci surgical system, most of which were independently researched and written by Intuitive Surgical. Figure 9.14 shows the number of articles published in the field of surgery from 1998 to 2009. The number of articles in the clinical database of the da Vinci surgical system is currently growing at a rate of 90-110 articles per month. Meanwhile, some peer-reviewed articles critical of robotic surgery have also gained attention through practical clinical applications.
As the company advances the commercialization of computer-assisted applications, regulatory procedures present a high barrier to entry. Regulatory bodies worldwide have engaged in discussions and issued opinions on electronic design, imaging systems, embedded software, clinical trial design, and patient recovery outcome analysis. Over the past decade, regulatory agencies around the world have been learning about our (Intuitive Surgical’s) foundational technologies and understanding their clinical applications. Generally, the technological maturity of clinical and technical reasoning increases over time. Successfully bringing a product to market requires interdisciplinary collaboration (engineers, clinical experts, management experts) to review the opportunities and risks of computer-assisted intervention systems.
Conclusion
Over the past 20 years, the evolution of remote surgical robots from science fiction to reality has spurred developments in many subjects in medicine, engineering, technology, and industry. It is particularly noteworthy that the key funding for remote surgery has been secured by teams in clinical medicine and engineering research, recognizing the value brought by their interdisciplinary collaboration: providing a crucial catalyst for creating a brand new surgical approach. Simultaneously, regulatory agencies have had to innovate their processes to balance the benefits and risks brought by new technologies, as their pursuit and responsibility are for patient health and safety.
The surgical robot industry stands on the shoulders of industrial giants. As a team, we strive to achieve the innovations that readers of this book expect, pushing for the next surgical revolution. Multidisciplinary collaboration is a vital component of our field and will become increasingly important in new applications. This work, collaboratively conducted by clinical scientists, surgeons, academic researchers, engineers, and regulators, will transform ideas from novels into technological realities, ultimately benefiting patients and their families immensely.
Scissor Hands Raymond’s Commentary:
As a shining star stock in the NASDAQ market, Intuitive Surgical is a company well worth studying. It seized the opportunity to combine healthcare and remote operation robotics (which is quite rare), leveraging support from the capital market to develop a star product made in the USA. From their development history, I feel that some commendable aspects are as follows:
Interestingly, this project is a successful military-to-civilian transition, reminding me that the internet also originated from military projects, indicating that the US military has gathered a large number of excellent and forward-thinking talents;
Quickly obtaining advanced research results from excellent research institutions and universities, combining capital markets, and advancing development in a corporate model;
Defining the main features of the product at the design stage and verifying them during experiments can reduce detours;
Rapid iteration and experimentation can improve the speed of product launch; do not spread too many R&D tasks at the beginning, as it may overshadow the main requirements of the product;
If a product’s after-sales service may be complex and prone to failures, then do not sell too many units initially (production and after-sales cannot bear the pressure);
The information in this translation is up to 2009; the da Vinci surgical robot remains unmatched to this day. However, as surgical robots are high-end medical products, their application population in China is mostly from the affluent class, where the emphasis on quality outweighs the cost-performance ratio. At the same time, surgical robots have both equipment and consumable characteristics, making it challenging for domestic surgical robots to capture the market of imported surgical robot products (the difficulty is far greater than that of stent products). Common cost-performance weapons may not be very effective, so it is essential to prepare for a tough battle. Of course, it currently appears that the annual surgical volume of the da Vinci surgical robot in China far exceeds that abroad, indicating that there are certainly opportunities available.
1.【FMEA】 Collection of Knowledge Related to the New Version of FMEA

2.【CSR】 Collection of Customer Special Requirements CSR
3.【Special Characteristics】 Collection of Special Characteristics Management
4.【Equipment Management】 Collection of Equipment Maintenance Management
5.【IATF16949】 Collection of Knowledge Related to the IATF16949 System
THE END
Copyright Statement:This public WeChat account (IATF16949) sources some articles from the internet. Unless it is truly impossible to confirm, we will indicate the author and source. Some articles were unable to contact the original author during the push. If there are copyright issues, please contact us, and we will delete and process it within 24 hours, thank you! If there are any inaccuracies in the content, please feel free to criticize and correct us.
Add to group or inquire about course details.
Scan to add the customer service WeChat for consultation.

 Click to read the original text for more exciting content.
Click to read the original text for more exciting content.