Today we share a study published inAugust 2025 in Clin J Am Soc Nephrol titled Pregnancy and Long-Term Kidney Function in CKD: A Systematic Review and Meta-Analysis, which aims to explore the impact of pregnancy on the long-term kidney function of CKD patients.
1.Background and Purpose of the Study
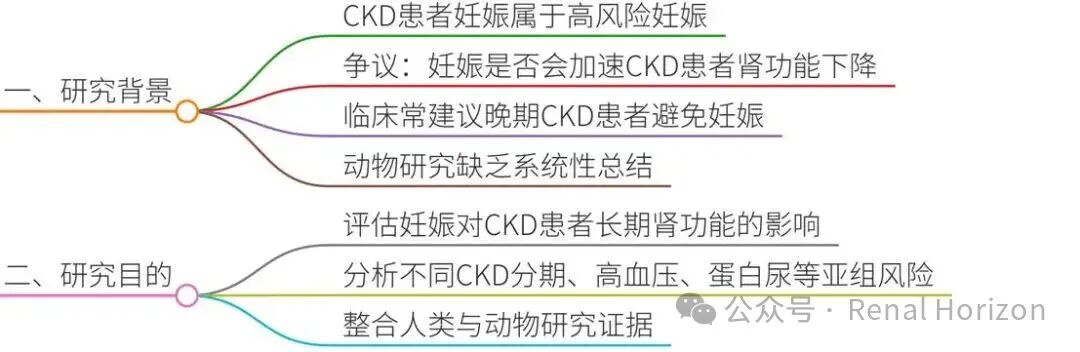
1.1Clinical Challenges of Chronic Kidney Disease (CKD) and Pregnancy
-
CKD affects approximately 3% of pregnancies and is considered a high-risk pregnancy due to the potential increased risk of preeclampsia, fetal growth restriction, preterm birth, and fetal death.
-
Current clinical paradigms suggest that the hyperfiltration state during pregnancy may accelerate the decline in kidney function in CKD patients, especially in those with advanced CKD, leading some physicians to recommend avoiding pregnancy. However, the specific impacts and subgroup risks (such as proteinuria or hypertension) remain unclear.
1.2Study Objectives
-
This study aims to synthesize evidence from human and animal studies through a systematic review and meta-analysis to:
-
Assess the impact of pregnancy on long-term kidney function in CKD patients (using standardized mean difference [SMD] and changes in glomerular filtration rate [GFR] as core indicators).
-
Identify high-risk subgroups (such as those with advanced CKD or chronic hypertension).
-
Provide mechanistic insights through animal studies.
1.3Innovations
-
This is the first study to simultaneously analyze human and animal studies and use patients as their own controls (rather than non-pregnant control groups), reducing selection bias.
2.Research Methods
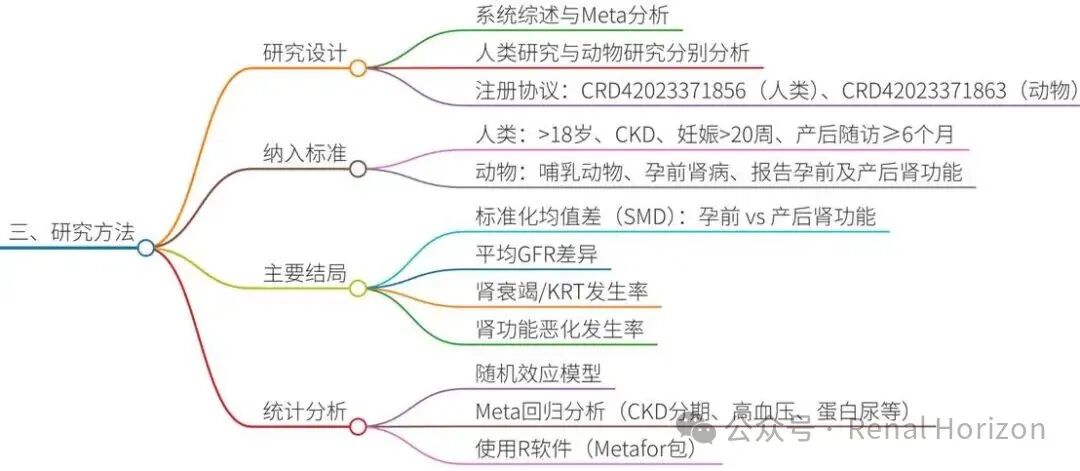
2.1Study Design
-
Following the PRISMA guidelines, a pre-registered protocol (human: CRD42023371856; animal: CRD42023371863) was established.
-
A systematic review and meta-analysis were conducted separately for human and animal studies.
2.2Literature Search and Screening
-
Databases Searched: PubMed and Embase (human studies searched until October 25, 2023, animal studies until April 3, 2024).
-
Inclusion Criteria:
-
Human studies: Adult CKD patients, pregnancy ≥20 weeks, postpartum follow-up ≥6 months. Exclusions included diabetes, SLE, and pregnancies after transplantation.
-
Animal studies: Mammals, pre-pregnancy kidney disease models, reporting kidney function data before and after pregnancy.
-
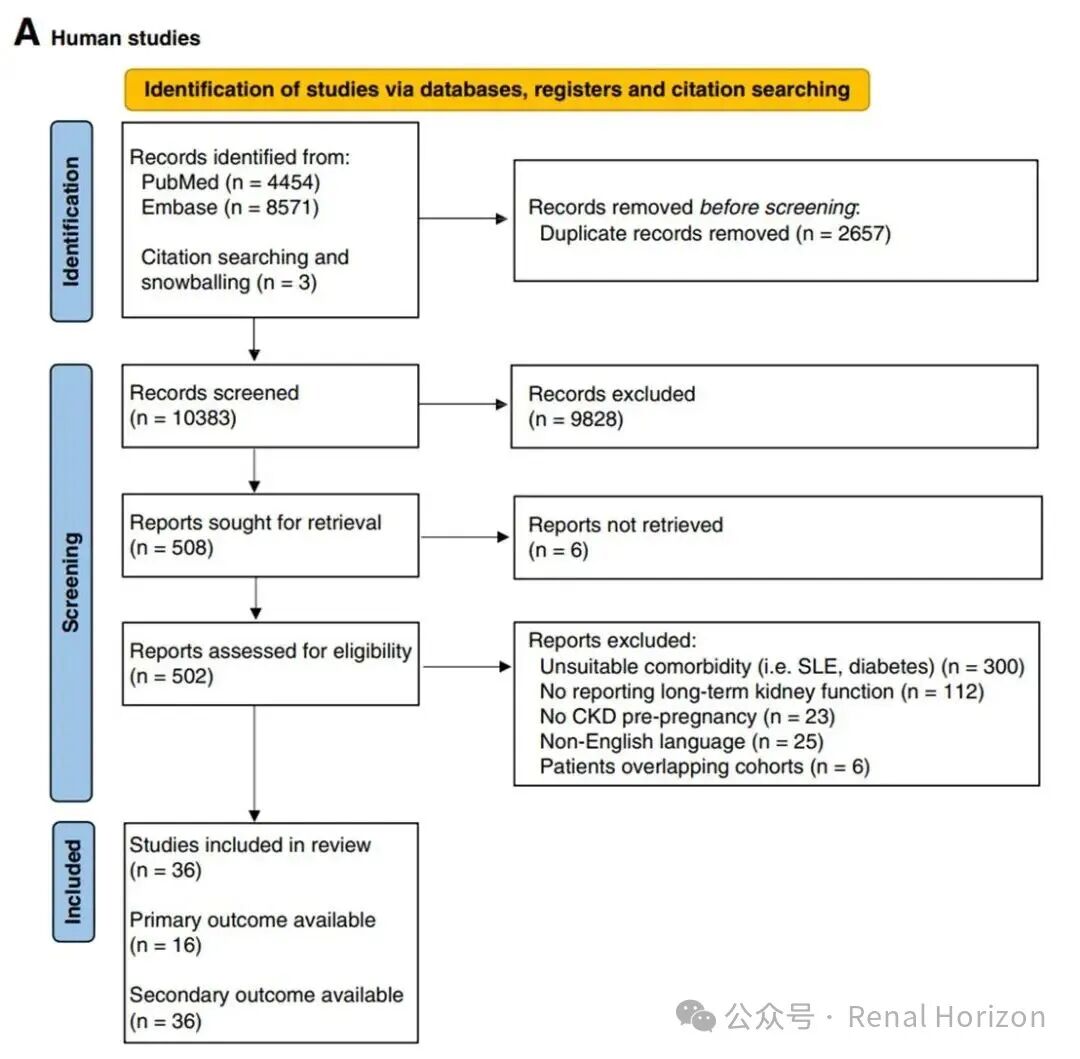
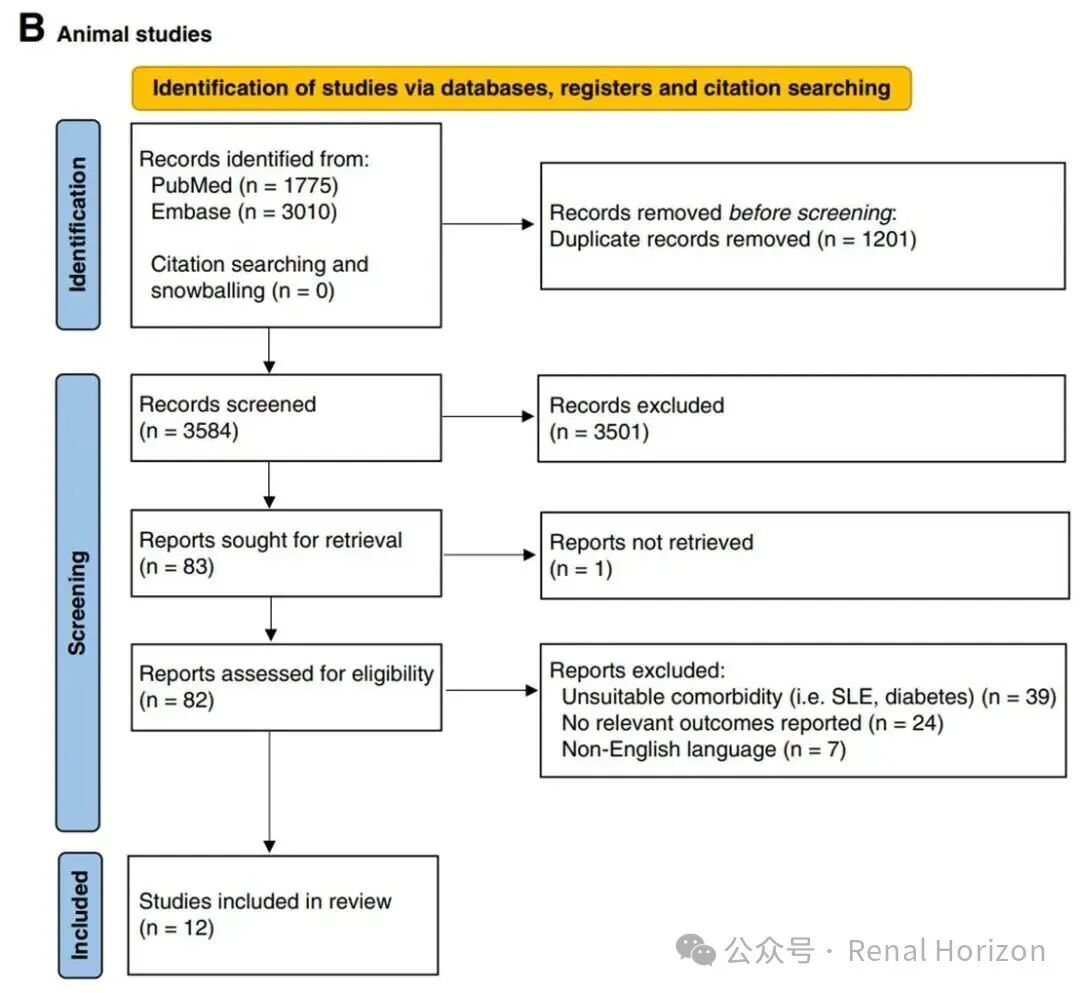
Screening Process: Two researchers independently screened, with discrepancies resolved by a third researcher. A total of 36 human studies (2945 patients, 4623 pregnancies) and 12 animal studies (104 animals, 183 pregnancies) were included.
-
See Figure 1 for the study selection process:
2.3Data Extraction and Quality Assessment
-
Human Studies: Extract baseline characteristics (such as pre-pregnancy kidney function, hypertension, proteinuria), primary outcomes (SMD of GFR/creatinine changes), and secondary outcomes (incidence of kidney failure/KRT). The Newcastle-Ottawa scale was used to assess bias risk, with overall quality rated as moderate.
-
Animal Studies: Extract types of kidney disease models (such as 5/6 nephrectomy), kidney function indicators (such as GFR, creatinine). The SYRCLE tool was used to assess bias risk, with most studies having unclear risk.
-
Subgroup definition: Advanced CKD is defined as >25% of patients in the cohort being in CKD stages 3-5 (eGFR <60 ml/min or creatinine >1.4 mg/dl).
2.4Statistical Analysis
-
A random-effects model was used for meta-analysis (R software).
-
Primary outcomes: SMD of kidney function changes before and after pregnancy; clinically significant indicators were the mean difference (MD) of GFR.
-
Meta-regression analysis examined moderators (such as CKD stage, hypertension, proteinuria).
3. Study Results
3.1Results from Human Studies
-
3.1.1Primary Outcome: Impact of Pregnancy on Kidney Function (SMD Analysis)
-
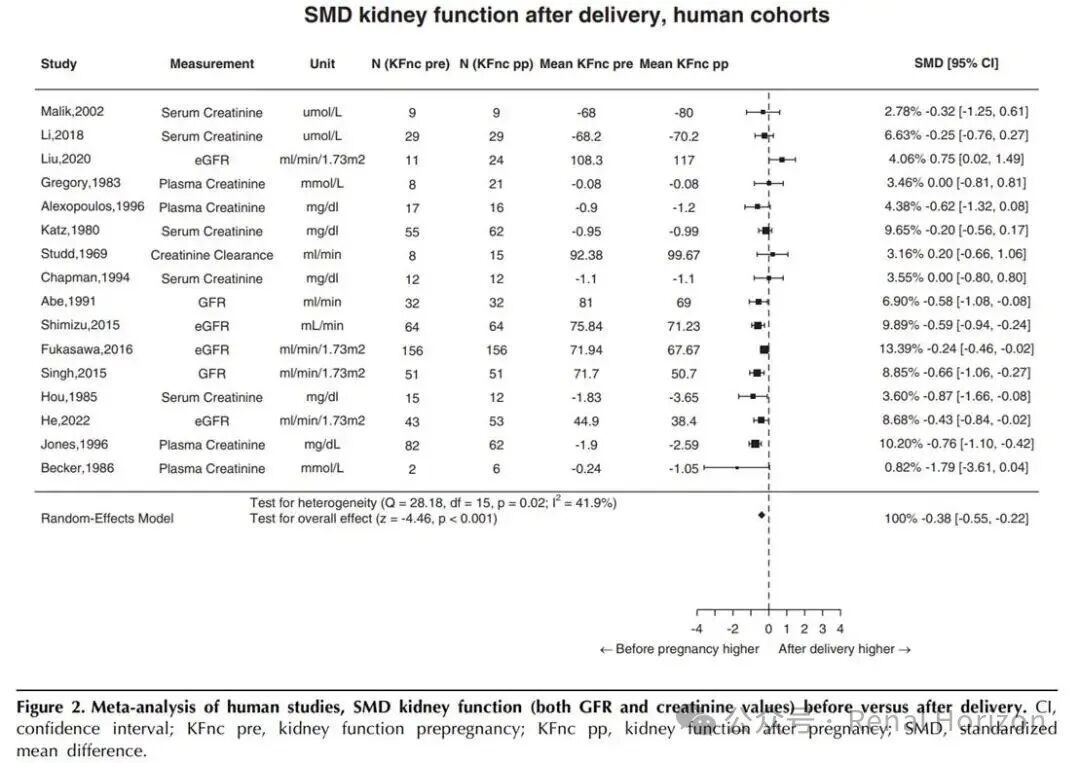
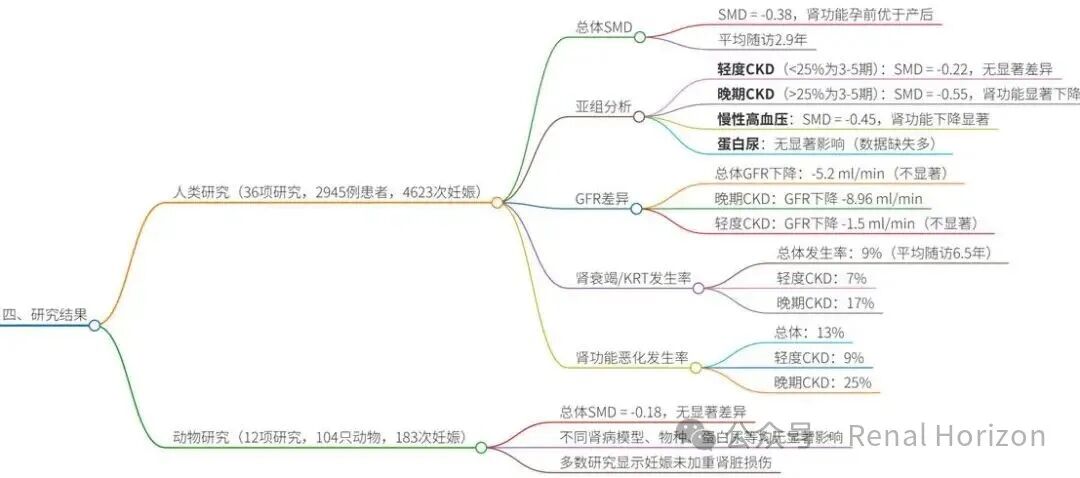
A summary of 16 studies showed that kidney function significantly declined after pregnancy (SMD = -0.38, 95% CI: -0.55 to -0.22, p<0.001), with a mean follow-up of 2.9 years.
-
However, subgroup analysis revealed key differences:
-
Mild CKD (≤25% of the cohort with advanced CKD): Pregnancy had no significant impact (SMD = -0.22, 95% CI: -0.56 to 0.13, p=0.22), with a mean follow-up of 4.4 years.
-
Advanced CKD (>25% of the cohort with advanced CKD): Kidney function significantly declined (SMD = -0.55, 95% CI: -0.80 to -0.30, p<0.001), with a mean follow-up of 2.2 years.
-
Meta-regression showed that chronic hypertension was a significant moderator (β=-0.01, p=0.03), while proteinuria and follow-up time had no significant impact.
-
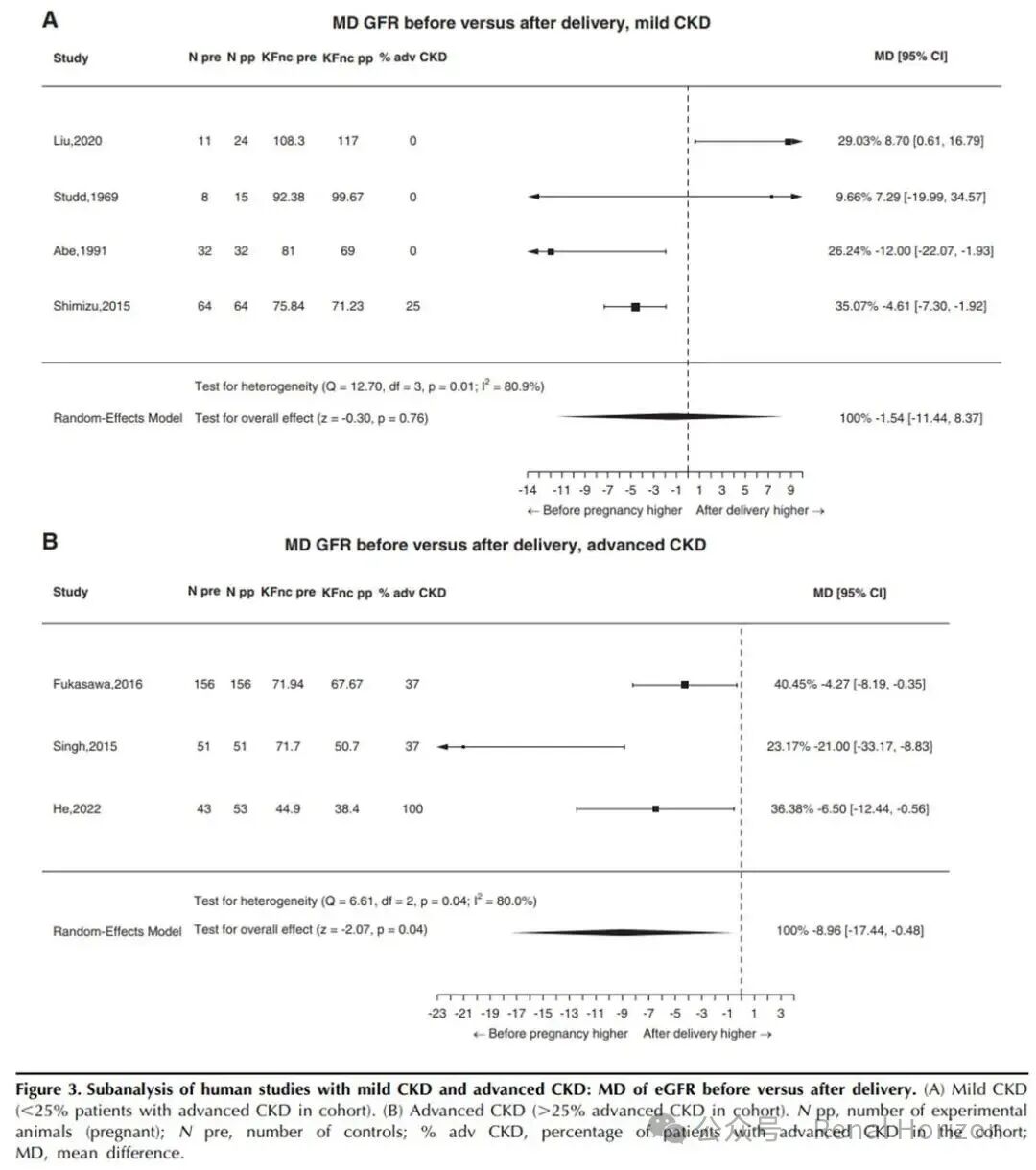
3.1.2Clinical Indicators: Changes in GFR and Creatinine (MD Analysis)
-
The summary of GFR differences showed that overall, the decline in GFR after pregnancy was not significant (MD = -5.2 ml/min, 95% CI: -11.7 to 1.2, p=0.11), but in the advanced CKD subgroup, the decline in GFR was significant (MD = -8.96 ml/min, 95% CI: -17.4 to -0.48, p=0.04), while there was no change in mild CKD (MD = -1.5 ml/min, p=0.76).
-
3.1.3Secondary Outcome: Incidence of Kidney Failure/KRT
- A summary of 36 studies showed that the incidence of kidney failure/KRT after pregnancy was 9% (95% CI: 6% to 13%), with a mean follow-up of 6.5 years.
- Subgroup analysis: The incidence in mild CKD was 7%, while in advanced CKD it was 17%. Chronic hypertension was a significant moderator (p<0.001).
- Compared to non-pregnant CKD patients, pregnancy did not increase the risk of kidney failure/KRT (RR=1.07, p>0.05).
3.2 Results from Animal Studies
-
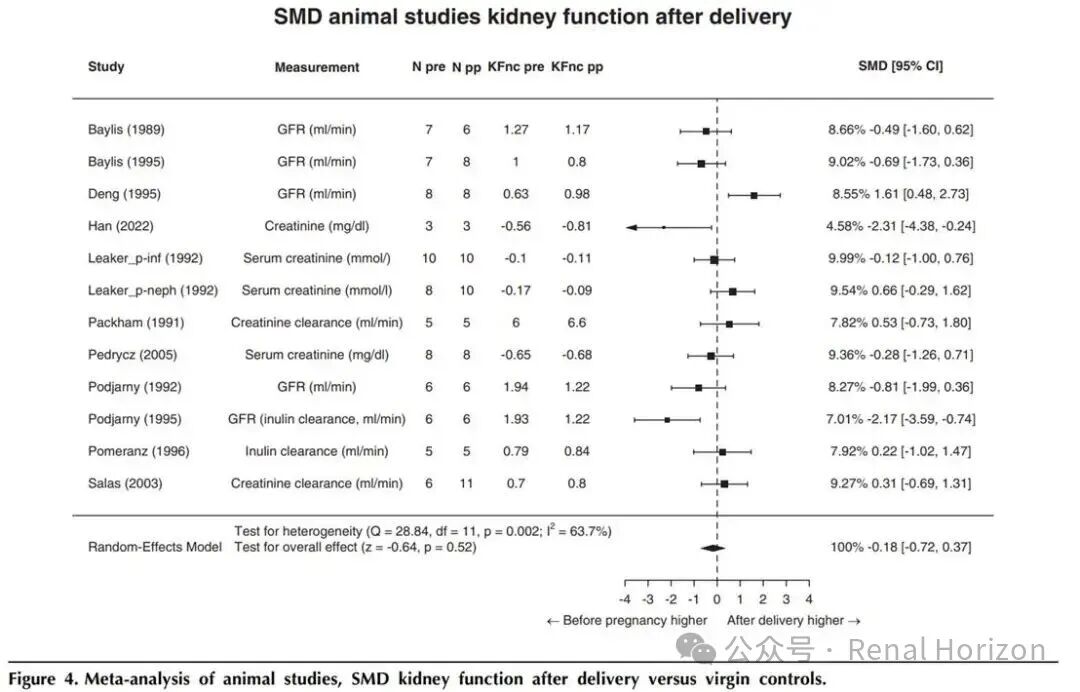
3.2.1Primary Outcome: Impact of Pregnancy on Kidney Function
-
12 animal studies (primarily rat models) showed no significant difference in kidney function after pregnancy compared to non-pregnant controls (SMD = -0.18, 95% CI: -0.72 to 0.37, p>0.05), suggesting that pregnancy does not have negative effects in animal models (possibly simulating mild CKD).
-
Factors such as type of kidney disease model and species had no significant moderating effects.
-
3.2.2Mechanistic Insights
- Kidney puncture experiments showed that glomerular pressure in pregnant animals did not increase, and histological examination showed no damage, supporting the mechanism that pregnancy does not exacerbate glomerulosclerosis.
4. Discussion and Clinical Significance
-
4.1Interpretation of Results
-
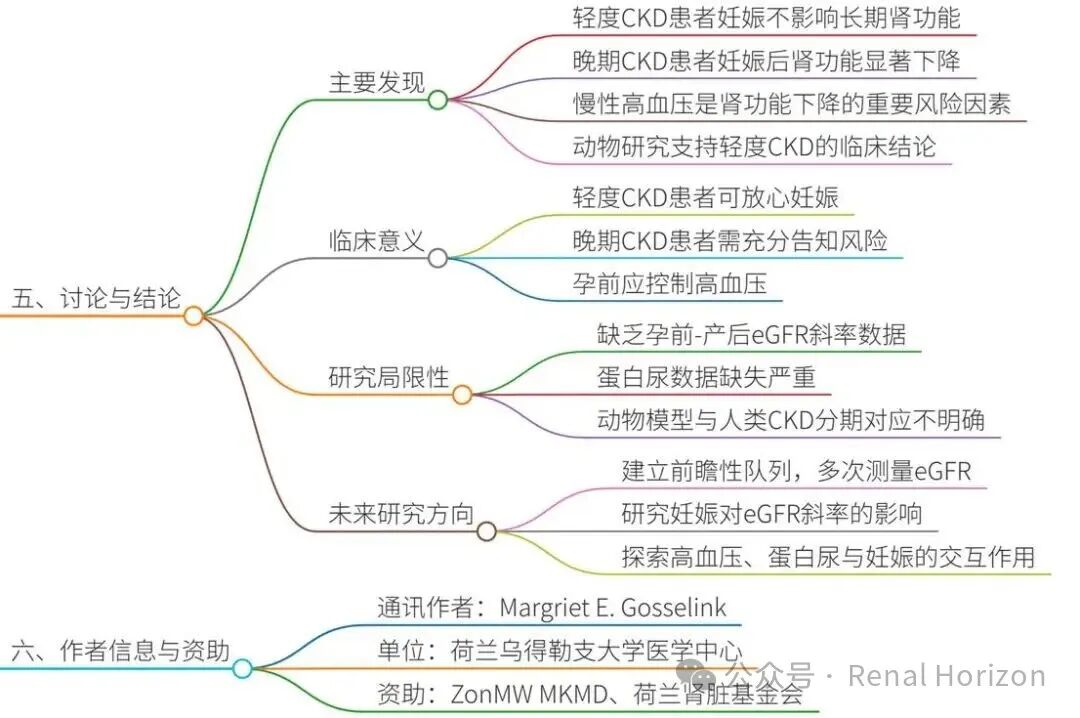
Pregnancy is safe for patients with mild CKD: Consistent with previous studies, pregnancy does not accelerate the decline in kidney function, possibly due to physiological hyperfiltration being reversible under preserved nephron units.
-
Significant risks in advanced CKD: The average decline in GFR is approximately 9 ml/min, equivalent to a loss of kidney function over 2.5 years of natural disease progression, consistent with studies by Wiles et al.
-
Animal studies validate: The models lack characteristics of advanced CKD, but provide mechanistic evidence (such as stable glomerular pressure).
-
4.2Limitations
-
High heterogeneity in human studies (e.g., varying definitions of CKD), short follow-up in advanced CKD limits long-term conclusions.
-
Missing proteinuria data affects the reliability of subgroup analyses.
-
The correspondence between animal models and human CKD stages is unclear.
-
4.3Clinical Recommendations
-
Patients with mild CKD: Pregnancy can be pursued without concern for kidney function.
-
Patients with advanced CKD: Should be informed of the risk of kidney function decline and receive individualized counseling.
-
Future research should be prospective, with multiple eGFR measurements to distinguish between pregnancy and natural progression.
5.Conclusion
-
5.1Key Conclusions
-
Pregnancy has no impact on long-term kidney function in patients with mild CKD, but there is a significant decline in kidney function in patients with advanced CKD.
-
Chronic hypertension is a key risk moderator.
-
Animal studies support clinical findings and suggest that pregnancy does not cause glomerular injury.
-
5.2Research Value
-
Provides evidence-based guidance for pre-pregnancy counseling, emphasizing risk stratification.
-
Calls for more studies on eGFR slopes to accurately quantify the contribution of pregnancy.
Mind Map
Note: This article is for academic exchange only and not for any commercial use. Copyright belongs to the original authors and the original publication.
Gosselink ME, Sluijters JMM, Snoek R, van Eerde AM, Wever KE, Lely AT. Pregnancy and Long-Term Kidney Function in CKD: A Systematic Review and Meta-Analysis. Clin J Am Soc Nephrol. 2025 Jul 14;20(9):1190-1205. doi: 10.2215/CJN.0000000769. PMID: 40658982; PMCID: PMC12445387.