Click the blue text below the title to follow us
This article was published in: Chinese Physician Magazine, 2022, 24(4): 496-499, 504.
Cite this article: Pan Xingbang, Zhong Jie, Li Zhao, et al. Meta-analysis of the correlation between sepsis-induced myocardial dysfunction and hypertension [J]. Chinese Physician Magazine, 2022, 24(4): 496-499, 504.
Authors
Pan Xingbang (Department of Emergency, Tsinghua University Affiliated Chuiyangliu Hospital, Beijing 100022)
Zhong Jie (Department of Emergency, Tsinghua University Affiliated Chuiyangliu Hospital, Beijing 100022)
Li Zhao (Department of Emergency, Tsinghua University Affiliated Chuiyangliu Hospital, Beijing 100022)
Gu Wei (Corresponding Author) (Department of Emergency, Tsinghua University Affiliated Chuiyangliu Hospital, Beijing 100022)
Abstract
Objective To systematically evaluate the correlation between sepsis-induced myocardial dysfunction (SIMD) and hypertension. Methods Clinical studies on the correlation between SIMD and hypertension were searched from PubMed, Embase, Cochrane Library, CNKI, CBM, and Wanfang database from inception to January 2022 using Chinese and English search terms. The quality of the literature was evaluated using the Newcastle-Ottawa Scale (NOS), and meta-analysis was performed using Stata 12.0 software on the included literature. Results A total of 16 articles were included after screening, with 3,758 subjects. The meta-analysis results showed that patients with a history of hypertension had a higher incidence of SIMD, and the difference was statistically significant. Subgroup analysis and sensitivity analysis indicated that the results were stable. Conclusion Hypertension is a risk factor for the occurrence of SIMD, and the results are statistically significant. Early intervention in septic patients with a history of hypertension may improve prognosis.
Sepsis is a syndrome of organ dysfunction caused by an inappropriate response of the body to bacterial, fungal, or viral infections [1]. Approximately 19 million patients are diagnosed with sepsis globally each year, with a mortality rate of >30%, making it the most common cause of death in intensive care units, and multiple organ dysfunction is the most direct cause of death in septic patients [2]. Among the multiple organ dysfunctions associated with sepsis, myocardial injury is the most common and severe complication. In 1984, Parker et al. first reported the existence of sepsis-induced myocardial dysfunction (SIMD) [3]. Data indicate that nearly 50% of septic patients will develop SIMD, with a mortality rate as high as 68% [4]. It can be said that the occurrence of SIMD to some extent determines the prognosis of septic patients. Effectively predicting the occurrence of SIMD and intervening early may improve clinical outcomes. However, effective research evidence on the risk factors for SIMD is still lacking [5]. Previous studies have suggested that hypertension seems to be a significant predictor of the occurrence of SIMD, but some studies have reached opposite conclusions, and the validity of this claim remains unverified. Therefore, this study intends to conduct a meta-analysis of the currently published related literature to provide effective references for the clinical diagnosis and treatment of SIMD.
1 Materials and Methods
1.1 Literature Search Strategy The English databases searched include PubMed, Embase, and Cochrane Library, while the Chinese databases include CNKI, CBM, and Wanfang Data Knowledge Service Platform. The literature search was conducted until January 2022. The English search terms included sepsis, bloodstream infection, pyemia, pyohemia, septicemia, myocardial dysfunction, myocardial infarction, myocardial damage, etc.; the Chinese search terms included 脓毒症, 脓毒血症, 败血症, 心肌损害, 心肌损伤, 心肌障碍, etc.
1.2 Inclusion and Exclusion Criteria
1.2.1 Inclusion Criteria (1) Age ≥ 18 years; (2) Diagnosis of sepsis based on international sepsis diagnostic criteria; (3) Clear diagnostic criteria for SIMD; (4) Data in the original literature such as mean, standard deviation, sample size, etc., can be directly extracted or derived after conversion.
1.2.2 Exclusion Criteria (1) Duplicate publications or translations; (2) Review articles, systematic reviews, and meta-analyses; (3) Commentaries or case reports; (4) Irrelevant literature; (5) Literature with low quality scores that cannot obtain valid data.
1.3 Data Extraction Method Two researchers screened relevant literature based on the above literature search strategy and inclusion-exclusion criteria, independently during the process, and cross-checked simultaneously. If necessary, a third researcher was consulted for further evaluation to determine whether to include it. Information required for the study was extracted from the selected original literature: first author, publication year, basic patient information, sample size, number of patients with hypertension.
1.4 Literature Quality Evaluation Case-control studies and cohort studies were evaluated using the Newcastle-Ottawa Scale (NOS) quality assessment method. Each included study was comprehensively assessed with a total score of 0-9, with studies scoring ≥7 considered high-quality studies eligible for meta-analysis.
1.5 Statistical Processing Meta-analysis was performed using Stata 12.0. The number of patients with hypertension was compared between the SIMD group and the non-SIMD group. Heterogeneity analysis was conducted on the included studies, and the I2 index was used to quantify heterogeneity. If I2 < 50%, it indicates low heterogeneity, and a fixed-effect model was used for analysis; if I2 ≥ 50%, a random-effects model was used. P < 0.05 indicates a statistically significant difference.
2 Results
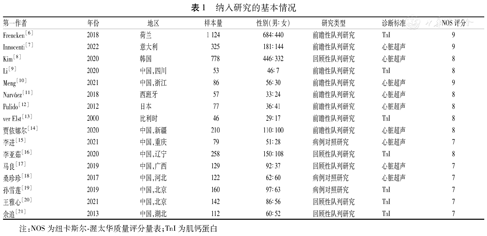
2.1 Summary of Literature Screening A total of 647 articles were retrieved from the database, with 5 from other sources. After further screening according to the inclusion-exclusion criteria, 16 studies were included [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. The diagnostic criteria for SIMD in all studies were based on echocardiography or troponin I (TnI). The included studies comprised 13 cohort studies and 3 case-control studies, with a total of 3,758 subjects. All included studies were high-quality studies, with NOS scores ranging from 7 to 9. See Figure 1 and Table 1.
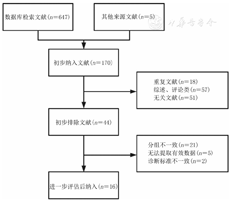
Figure 1 Literature screening process and results
2.2 Meta-analysis Results Heterogeneity analysis of the included studies showed significant heterogeneity (I2 = 60.9%, P = 0.001), and a random-effects model was used for analysis, with subgroup analysis based on different diagnostic criteria. The results showed that patients with a history of hypertension in the SIMD group had a statistically significant difference compared to the non-SIMD group (OR = 1.54, 95% CI: 1.17-2.03). Subgroup analysis suggested that SIMD defined by TnI was the main source of study heterogeneity (I2 = 76.8%, P < 0.001), while SIMD diagnosed by echocardiography had lower heterogeneity (I2 = 16.5%, P = 0.295). Both subgroups indicated that hypertension might be a clear risk factor for SIMD (TnI group OR = 1.75, 95% CI: 1.04-2.93; echocardiography group OR = 1.35, 95% CI: 1.04-1.74). See Figure 2. Sensitivity analysis of the original literature showed that there was no significant difference between the fixed-effect model and the random-effects model results, indicating that the results of this meta-analysis are stable and reliable. See Figures 3 and 4. Begg’s test for publication bias indicated no significant publication bias in this study (Z = 0.39, P = 0.703). See Figure 5.
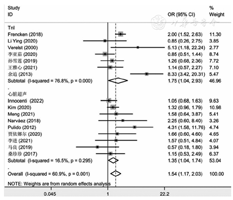
Figure 2 Forest plot of the number of patients with hypertension in the SIMD group versus non-SIMD group
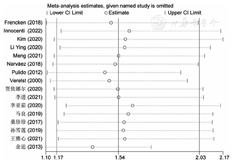
Figure 3 Sensitivity analysis of the random-effects model
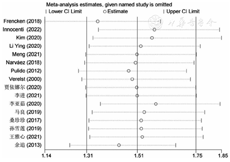
Figure 4 Sensitivity analysis of the fixed-effects model
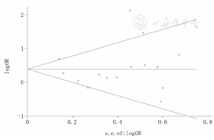
Figure 5 Begg’s test for publication bias
3 Discussion
The pathophysiological mechanisms of SIMD are still not fully understood. Broadly speaking, SIMD is considered to be the result of the complex interactions of numerous factors such as genetics, metabolism, molecular, and structural changes after the occurrence of sepsis. Based on the current diagnostic criteria for SIMD, its mechanisms can be summarized as follows: First, from a structural perspective, infection by pathogenic bacteria can trigger the body’s immune response, releasing a large number of inflammatory factors. When these inflammatory factors reach the myocardium via the bloodstream and act on myocardial cells, they induce inflammatory responses within the myocardium, increase the permeability of cardiac capillaries, and affect the concentration gradient of calcium ions inside and outside myocardial cells, thereby impairing mitochondrial function in myocardial cells, leading to cardiac microvascular dysfunction and inducing myocardial cell apoptosis, resulting in the release of myocardial enzymes into the blood [22,23]. Thus, TnI becomes an important indicator for the diagnosis of SIMD, and the increase in TnI during SIMD may not be related to myocardial ischemia [24]. Secondly, from a functional perspective, myocardial edema can lead to a decrease in myocardial contractility, limiting the ability of the ventricles to eject blood at the end of systole, thereby reducing stroke volume, which compensatorily increases end-diastolic volume, resulting in varying degrees of impairment in myocardial diastolic function [25]. This change is evident in both the left and right heart systems, but is particularly pronounced in the left heart, thus the evaluation of left ventricular ejection function by echocardiography also holds diagnostic value for SIMD.
This study conducted a meta-analysis of the currently published literature, and the analysis results suggest that hypertension may be a risk factor for the occurrence of SIMD, with statistically significant results. Hypertension, as a clinical syndrome that can significantly affect hemodynamics, has been confirmed to cause organic damage and functional impairment to multiple organs such as the heart, brain, and kidneys. Previous studies have found that hypertension has inflammatory effects on myocardial cells [26]. The activation of the renin-angiotensin-aldosterone system (RAAS) is the primary cause of hypertension, where competitive binding of the AT-1 receptor reduces the binding capacity of the AT-2 receptor with angiotensin II, leading to increased blood pressure. Castoldi et al. [27] found that activation of the AT-2 receptor or Mas receptor can not only dilate blood vessels and lower blood pressure but also reduce myocardial inflammatory cell infiltration. Therefore, it can be speculated that hypertension may exacerbate the inflammatory response of the myocardium during sepsis, promoting the occurrence of SIMD. At the same time, the relationship between hypertension and myocardial remodeling can also be further elucidated by the activation of RAAS, as hypertension-mediated myocardial hypertrophy can exacerbate the myocardial contractile and diastolic dysfunction during sepsis-induced tissue edema, thereby triggering SIMD.
The limitations of this study are as follows: First, the overall heterogeneity of the 16 included articles remains high, which may introduce certain errors into the analysis results; second, in the subgroup analysis, due to the differences in instruments, equipment, and physician qualifications among various original studies, there may be certain errors in the diagnostic criteria for echocardiography and TnI, which could affect the final research results.
Research has found that SIMD is reversible and often returns to normal within 1-3 weeks after occurrence [28]. Therefore, timely and effective intervention for patients with risk factors for SIMD can significantly reduce mortality, which is of positive significance. This study systematically evaluated the currently published relevant literature through a meta-analysis, concluding that hypertension is a risk factor for the occurrence of SIMD, with statistically significant results, which can provide references for the clinical prevention and treatment of SIMD in the future.
Conflict of Interest All authors declare no conflict of interest
References (omitted)

Chinese Physician Magazine
Phone: 0731-84470811
WeChat: 18108455060
Website: www.zgyszz.com