Chest Window
This is not just a public account….

-
The fourth edition of the Fleischner Society’s compilation of chest imaging terminology is based on the third edition (2008, with the first and second editions released in 1984 and 1996 respectively), with additions, deletions, adjustments, and corrections.
-
In addition to imaging descriptions of terms, it emphasizes anatomical, physiological, and pathological explanations.
-
Term order: Alphabetical by English letters.
Source:
Pleura
The pleura is a double-layered serous membrane that covers the lungs and folds back at the hilum. These two layers are separated by a small amount of viscous lubricant (pleural fluid). The surface tension caused by pleural fluid, combined with negative pressure, pulls the parietal pleura and visceral pleura tightly together. Each layer of pleura consists of a single layer of mesothelial cells and a layer of submesothelial tissue. The two layers of pleura form a virtual “pleural cavity”.
On imaging, the normal pleura is best displayed when the fissures or extrapleural fat are shown.
The parietal pleura lines the inner surface of the thoracic cavity on either side of the mediastinum and can be divided into mediastinal (covering the lateral aspects of the fibrous pericardium, esophagus, and thoracic aorta), diaphragmatic (covering the superior surface of the diaphragm), and costal pleura (covering the inner surface of the thoracic wall). The visceral pleura covers the surface of each lung and extends into the fissures between the lobes, forming the interlobar fissures.
The adjective form (pleural) is commonly used with the following terms:
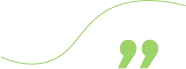
(Pleural) effusion: refers to fluid accumulation in the pleural cavity. Excess pleural fluid can be caused by mechanical factors, edema, infection, inflammation, or malignancy. Radiographically, a small pleural effusion may present as blunting of the costophrenic angle, often crescent-shaped, while a larger pleural effusion appears as a homogeneous high-density shadow in gravity-dependent areas. On CT, the density of pleural effusion varies, and the pleural cavity widens. During enhancement scanning, CT can depict pleural cavity separations and thickening and congestion of the pleura.
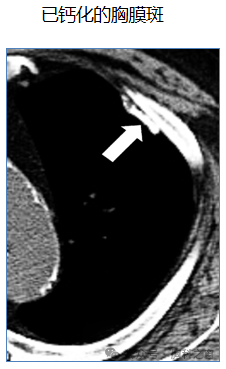
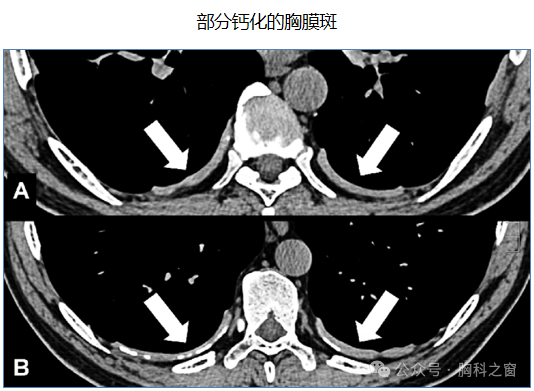
(Pleural) plaques: focal translucent fibrous lesions occurring on the parietal pleura. Pleural plaques are often associated with past exposure to natural fibrous silicates (commonly asbestos). On imaging, pleural plaques appear as sharply defined flat elevations or plateau-like thickening of the pleura, often with calcification.
(Pleural) retraction: one or more thick linear or band-like strands emanating from a lesion (such as a nodule or its components) and directly connecting to the pleura or interlobar fissures. Pathologically, pleural retraction is often associated with thickening of the interlobar septa connecting the lesion and pleura. Although pleural retraction is often nonspecific, it has been described as a potential sign of visceral pleura invasion.
(Pleural) thickening: localized or diffuse increase in pleural thickness, often due to fibrosis secondary to chronic or recurrent mechanical irritation (such as rib fractures) or pleural effusion or pneumothorax.
Pleural thickening can also be caused by asbestos exposure or infection, and tumors such as metastatic tumors, lymphoma, or mesothelioma. On CT, pleural thickening presents as curvilinear soft tissue shadowing extending inward to the ribs and the most inner intercostal muscles. Thickened pleura often enhances, best displayed on intravenous contrast-enhanced scans.
Pneumatocele
A pneumatocele is a thin-walled, gas-filled cystic structure within the lung parenchyma. Pneumatoceles can occur due to pneumonia, trauma (including barotrauma), or inhalation of hydrocarbon liquids (such as in “fire-eating” performances). Pneumatoceles may be transient and can result from necrosis of lung parenchyma and one-way valve airway obstruction.
On imaging, a pneumatocele appears as a round, thin-walled cystic lesion within the lung, sometimes accompanied by an air-fluid level.

Pneumomediastinum
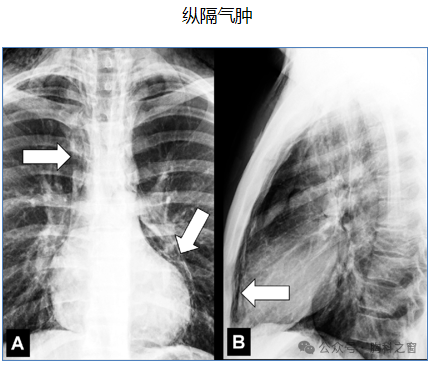
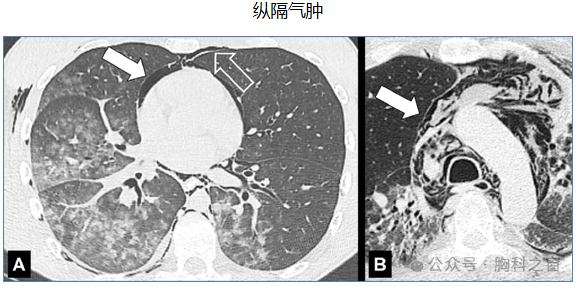
Pneumomediastinum is the abnormal accumulation of air or gas in the mediastinum (outside the esophagus and tracheobronchial tree). It can be caused by spontaneous alveolar rupture, trauma, or esophageal rupture (subsequently allowing air to enter the mediastinum along the axial space). It is most commonly seen in surgical trauma, barotrauma, or diseases associated with chronic coughing such as asthma or interstitial lung disease.
On imaging, pneumomediastinum appears as one or more low-density linear or band-like areas of air outlining the structures of the mediastinum.
Pneumonia
Pneumonia is a commonly used diagnostic term, usually referring to lung parenchymal infection. Pneumonia can be caused by bacteria, viruses, fungi, parasites, or other microorganisms and can be focal or multifocal. Pneumonia may present as opaque shadows, possibly accompanied by air bronchograms, tree-in-bud signs, or pleural effusions.
Pneumonitis is a diagnostic term referring to inflammation of the lung parenchyma, including both infectious and non-infectious causes. Infectious pneumonia is usually referred to as pneumonia, while non-infectious pneumonia can be caused by various conditions including aspiration, allergies, radiation, autoimmune diseases, and medications.
The terms “pneumonia” and “pneumonitis” are sometimes used interchangeably, but it is best to adhere to the definitions above.
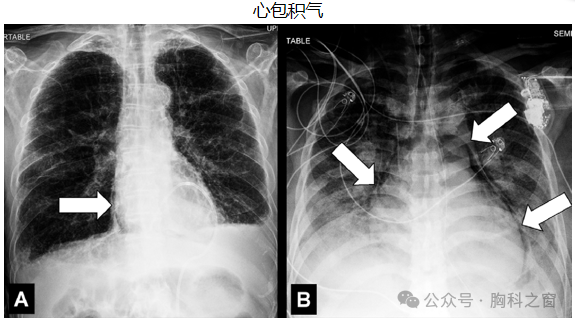
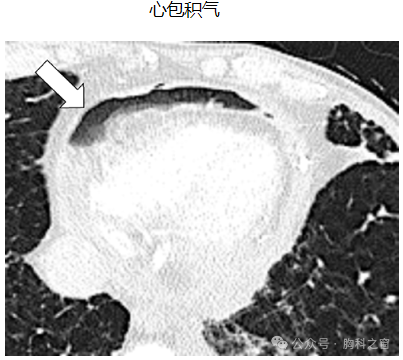
Pneumopericardium
Pneumopericardium is the accumulation of air in the pericardial cavity. Pneumopericardium has been described in premature infants or mechanically ventilated children. In adults, it is usually due to trauma or cardiac surgery. It can occur concurrently with other pathological gas accumulations, such as pneumomediastinum or pneumothorax. On imaging, pneumopericardium appears as air or gas density within the unstructured space (pericardial cavity), separating the two layers of the pericardium.
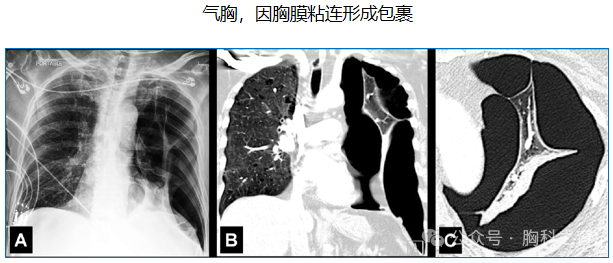
Pneumothorax
Pneumothorax refers to the presence of gas or air in the pleural cavity, separating the visceral and parietal pleura. As a result, the lung may partially or completely collapse. Pneumothorax can be caused by the rupture of a spontaneous pulmonary bulla or by mechanical trauma (including iatrogenic injury).
The diagnosis of tension pneumothorax relies on clinical and physiological criteria, typically manifesting radiographically as mediastinal shift to the opposite side and ipsilateral diaphragm collapse. Tension pneumothorax is often due to a one-way valve mechanism. Ultimately, the definitive diagnosis of tension pneumothorax depends on clinical and/or physiological criteria.
Pneumothorax is generally identifiable on an upright chest X-ray, appearing as a curvilinear visceral pleural line, indicating the boundary between air in the pleural cavity and an inflated lung. However, on a supine chest X-ray, when the separated pleural surfaces are not tangent to the X-ray beam, pneumothorax may be difficult to detect. In these cases, ancillary findings (such as an abnormally sharp interface between the lung and mediastinal or cardiac structures) may be helpful. The “deep sulcus sign” refers to an abnormally deep costophrenic angle, decreased density, and an unusually sharp boundary.
Saber-sheath Trachea
The saber-sheath trachea refers to an abnormal shape of the trachea, where the anteroposterior diameter is increased and the transverse diameter is decreased, resembling a saber sheath. To meet the definition, at the same anatomical level, the coronal inner diameter of the trachea must equal or be less than 2/3 of the anteroposterior diameter, without any external compressive cause.
The saber-sheath trachea is most commonly seen in patients with chronic obstructive pulmonary disease and is believed to be the result of chronic inflammation and subsequent remodeling of the tracheal wall.

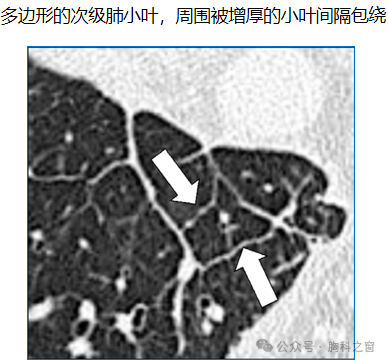
Secondary Pulmonary Lobule
The secondary pulmonary lobule is the smallest structural unit of lung parenchyma surrounded by a connective tissue sheath. It is irregularly polyhedral or conical in shape, with edge lengths ranging from 5 mm to 25 mm, containing 3 to 25 acini. The central structure (core structure) of the secondary pulmonary lobule includes bronchioles and accompanying pulmonary arteries and lymphatics. The connective tissue sheath of the secondary pulmonary lobule accommodates veins and lymphatics. The secondary pulmonary lobule also has an internal supporting structure, known as the intralobular stroma.
CT can display the three basic components of a normal secondary pulmonary lobule, namely the central structure, the area where acini are located, and the connective tissue sheath (forming the interlobular septa).
Segment
A segment is the structural unit of a lobe of the lung, supplied by a segmental bronchus for air, a segmental pulmonary artery for blood supply, and drained by segmental pulmonary veins. The right lung has 10 segments: 3 in the upper lobe, 2 in the middle lobe, and 5 in the lower lobe. The left lung has 8 or 10 segments, depending on whether the apico-posterior segment of the upper lobe and the antero-medial segment of the lower lobe are considered one or two segments.
Radiographically, the segment can be inferred based on the position of the bronchus and artery supplying the segment. Occasionally, segments may be separated by accessory fissures.
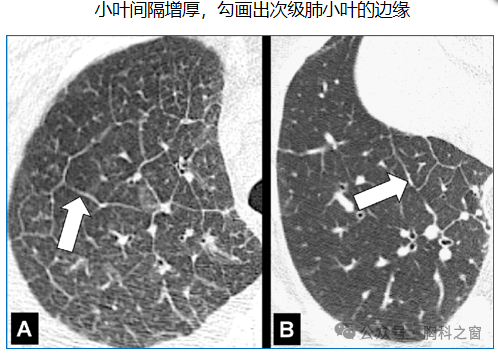
Septum
The septum is a sheath-like connective tissue structure surrounding the secondary pulmonary lobule. Because they separate the pulmonary lobules, they are also referred to as “interlobular septa,” containing veins and lymphatics.
Due to the vertical orientation of the interlobular septa towards the pleura, in otherwise healthy patients, isolated septal lines may occasionally be seen on CT scans at the apex and base of the lungs, appearing as fine linear structures separating the secondary pulmonary lobules. When the interlobular septa are thickened (as in interstitial pulmonary edema), they are more easily discernible.
The adjective form “septal” is commonly used with the following terms:
(Septal) line: represents linear structures of the interlobular septa.
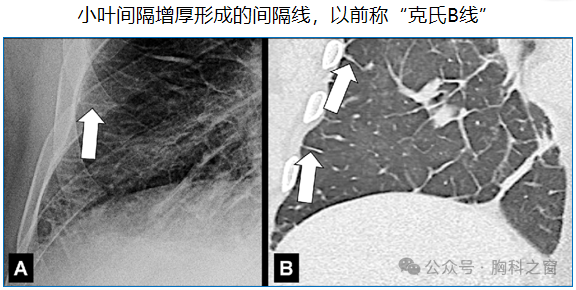
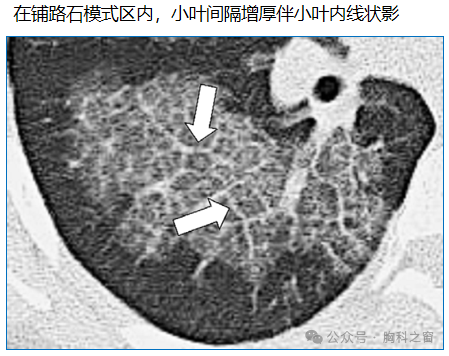
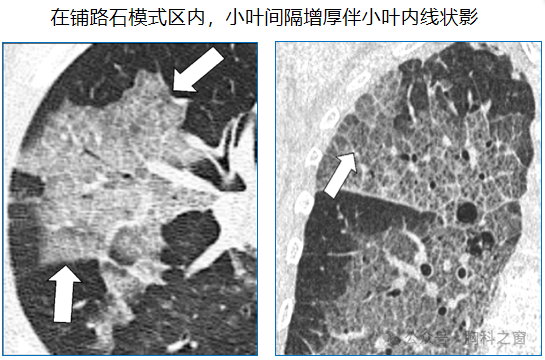
(Septal) thickening: visible on chest X-rays and CT, appearing as fine linear structures perpendicular to and connecting with the lateral pleural surface.
The term “Kerley line” previously used on chest X-rays is an outdated and not recommended term, reflecting the accumulation of fluid or tumor in the lung interstitium (such as pulmonary edema, lymphatic metastatic cancer, and/or mechanical lymphatic obstruction). On CT, interlobular septal thickening may appear smooth or nodular, aiding in the differentiation between pulmonary edema and lymphangitic infiltration or obstruction.
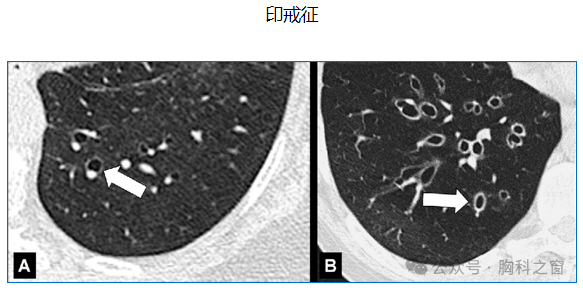
Signet Ring Sign
The signet ring sign refers to the cross-section of an expanded bronchus appearing as a ring-like structure, closely accompanied by a smaller round dense structure (representing the accompanying pulmonary artery), resembling a signet ring.
This sign is considered a typical manifestation of bronchiectasis but can also be seen in diseases with decreased pulmonary arterial blood flow (chronic thromboembolic disease or proximal pulmonary artery interruption).
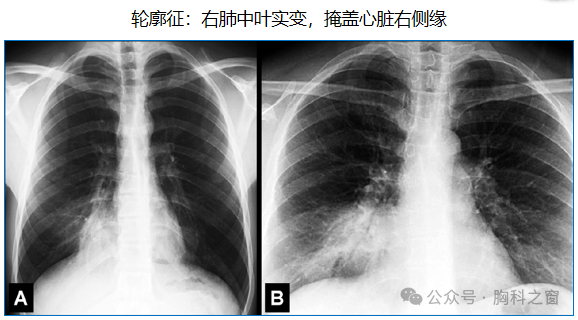
Silhouette Sign
The silhouette sign refers to the normal outline or surface being obscured (often incorrectly described as silhouetting) due to similar radiographic attenuation of adjacent structures, resulting in the normal anatomical boundary or surface being obscured.
However, this sign does not always indicate lung disease; for example, the cardiac border may be obscured, sometimes due to anatomical variations such as pectus excavatum.
Small Airways Disease
Small airways disease is a general term for peripheral airway diseases. The definition of this term is not uniform. Some radiologists consider small airways to have a diameter of ≤2 mm and a wall thickness of less than 0.5 mm. Others consider the boundary between central and peripheral airways to be at the level of the bronchioles. Despite the inconsistency in these two definitions, the first viewpoint is more practical and more commonly used in the literature.
On CT, these diseases may present as peribronchial and/or bronchiolar diseases, including tree-in-bud signs, centrilobular micronodules, air trapping, bronchiolar dilation, decreased pulmonary blood flow, or a combination of the aforementioned findings.
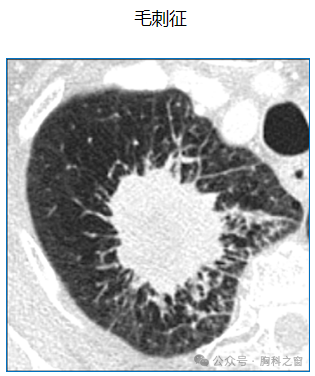
Spiculation
Spiculation is a descriptive term referring to multiple fine linear shadows emanating from a lesion (such as a nodule or its components) and radiating into the surrounding lung parenchyma. Pathologically, spiculation is often associated with a process of connective tissue proliferation within a nodule (such as invasive malignancy), leading to fibrous strands radiating into the surrounding lung parenchyma. Spiculation is also associated with direct infiltration into adjacent bronchial or vascular structures, or focal lymphatic dilation. The presence of spiculation in lung nodules increases the likelihood of lung cancer, although it is not specific.
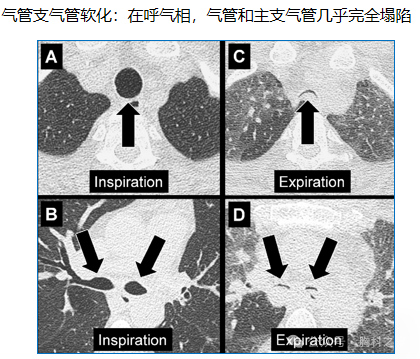
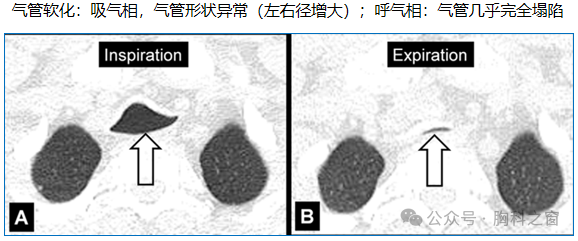
Tracheomalacia, Tracheobronchomalacia
Tracheomalacia and tracheobronchomalacia are terms used when the trachea and/or main bronchi excessively move inward during expiration due to pathological weakness of the cartilaginous airway walls.
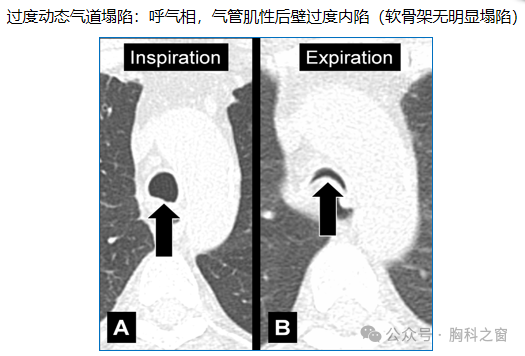
When the collapse of the tracheobronchial tree is due to excessive inward motion of the posterior muscular wall of the trachea or main bronchi during expiration, the closely related term “dynamic airway collapse” is used.
Both conditions can be diagnosed using dynamic expiratory CT. However, it is important to note that healthy individuals can have tracheal collapse of ≧70% during forced expiration.
Author: Xuanyong Bu Shenzhen Longgang District Maternity and Child Health Hospital, Radiology Department

END
Click the lower left corner “Read the original text” to view the original text of this article or participate in the discussion. Log in to the Chest Window website (www.tbwindow.com) or download the Chest Window APP to access a wealth of chest medicine academic materials. The Chest Window family welcomes your participation.

 Chest Window APP Long press the left QR code to download.
Chest Window APP Long press the left QR code to download.