
Methods and Detection Rates for DRT Post-LAAC
Research related to DRT has always been a key topic of interest in the field of LAAC. Studies have confirmed that there is a risk of DRT occurrence with devices such as ACP, WATCHMAN, LAmbre, or Amulet. Imaging techniques can help doctors clearly and intuitively identify DRT in patients.
Currently, transesophageal echocardiography (TEE) remains the classic imaging tool for discovering and monitoring DRT, with guidelines from Europe and America recommending that TEE imaging should include at least three planes (0°-30°, 60°-90°, and 120°-180°). However, with the increasing use of TEE in recent years, clinicians have gradually become aware of some issues: on one hand, TEE is a semi-invasive method, and performing TEE without sedation or general anesthesia poses dual physiological and psychological challenges for patients; on the other hand, TEE is subject to significant operator influence. If the operator lacks proficiency, image acquisition may be insufficiently comprehensive. If artifacts are detected during the procedure, other methods must be used for differentiation, which usually leads to prolonged examination times and increased discomfort for the patient. However, with advancements in imaging technology, CT has also gradually become an important tool for discovering and monitoring DRT alongside TEE.
The detection rate of DRT is a primary concern for clinicians, and the data and results will influence clinical decision-making. Many studies and reports have mentioned the detection rate of DRT. A study conducted across eight centers in France over five years with 469 patients post-LAAC showed an average follow-up of 13 months, with a DRT incidence of 7.2%. DRT events increase the risk of postoperative stroke; however, it is noteworthy that in this study, the DRT event rate for the Amulet device was as high as 25%, and there were issues with incomplete postoperative follow-up and nearly half of the patients not receiving standardized anticoagulation treatment, leading to questionable results. A study published in Circulation included 1,739 patients who underwent LAAC using the WATCHMAN device, with a total follow-up of 7,159 patient-years, reporting a DRT incidence of 3.7% (65/1739), with a total of 74 DRT events occurring. The EWOLUTION study also elaborated on the detection of DRT, enrolling 1,020 patients, primarily using TEE for follow-up. Among the 875 patients followed up, the DRT incidence was 3.7% at one year and 4.1% at two years. Additionally, studies on the DRT incidence with ACP and Amulet devices have yielded corresponding results: one follow-up study on the ACP device indicated a DRT incidence of 4.4% (28/632); another study on the Amulet device reported a DRT incidence of 1.6%. Based on numerous pieces of evidence, a meta-analysis on DRT post-LAAC proposed that the occurrence rate of DRT is approximately 3.8%, and DRT increases the risk of stroke in patients by 4 to 5 times. Furthermore, studies have shown that the occurrence of DRT is mainly concentrated at 90 days, 180 days, and one year post-surgery (Figure 1). Therefore, timely monitoring of DRT occurrence through imaging tools such as TEE postoperatively will help reduce the risk of thrombosis and stroke in patients.
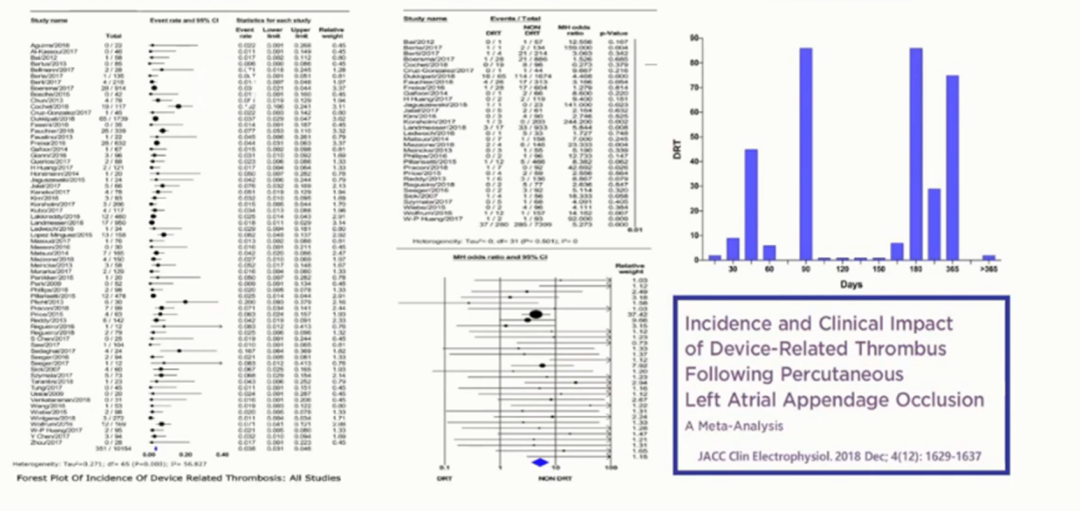
Figure 1. Results of the Meta-Analysis on LAAC DRT
Studying the influencing factors of DRT occurrence can help in formulating and modifying clinical decisions to ensure better prognoses for patients and to avoid DRT occurrence as much as possible. A recent study published in Circulation confirmed that patient factors are one of the triggering factors for DRT occurrence, with high-risk factors including high CHA₂DS₂-VASc scores, history of TIA/stroke, permanent atrial fibrillation, vascular disease, left atrial enlargement, and decreased EF.
Postoperative medication factors also influence DRT occurrence. A multicenter study in France showed that the DRT occurrence rate among patients was 7.6%, with 90% of patients having a history of bleeding, and over 70% had contraindications to anticoagulation, resulting in nearly half of the patients post-LAAC not receiving anticoagulation treatment. Therefore, it is speculated that postoperative medication factors also affect DRT occurrence. Additionally, a comparison of data from numerous studies reveals that the surgical instruments significantly impact DRT occurrence, with the surface thrombosis rate of WATCHMAN generally maintained between 1% and 6%; however, the surface thrombosis rate of ACP fluctuates more significantly (Figure 2). The endothelialization of the occluder is also one of the influencing factors for DRT occurrence; if endothelialization is complete, it can reduce the DRT incidence and the occurrence of device embolization complications. Furthermore, the implantation position of the occluder, the effectiveness of the occlusion, residual shunting, and clopidogrel resistance are also surgical instrument-related factors that influence DRT occurrence.
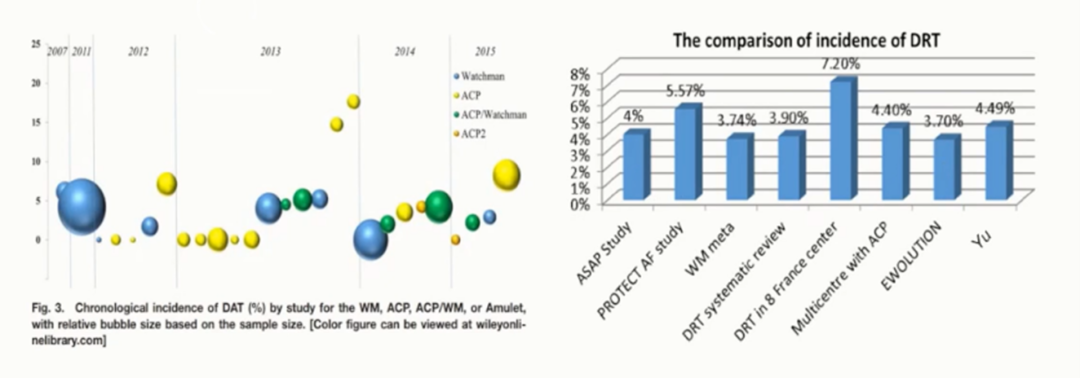
Figure 2. Impact of Device Types on DRT Occurrence
The treatment strategies for DRT are relatively clear. The JACC 2019 treatment recommendations for DRT state:
a. For patients diagnosed with DRT who have not received OAC treatment, warfarin treatment for 8 to 12 weeks (International Normalized Ratio (INR) of 2-3);
b. For patients already on warfarin, it is recommended to raise the INR to 2 to 3.5;
c. If the bleeding risk is low, consider adding a low dose of aspirin to warfarin;
2. Oral Anticoagulants (OAC):
Use full-dose direct OAC for 8 to 12 weeks, regardless of whether low-dose aspirin is added;
3. Low Molecular Weight Heparin (LMWH):
If the thrombus is very large (>15 mm) and mobile, the risk of embolism may increase, requiring treatment with LMWH, and TEE/CT should be repeated within two weeks to ensure treatment response. Intravenous heparin can replace LMWH in patients with renal failure.
4. Surgical Intervention:
In cases of very large device thrombus, recurrent embolism of DRT, or OAC treatment failure, surgical removal of the thrombus and the left atrial appendage closure device is required.
However, overall, prevention of postoperative DRT occurrence is still greater than treatment. By improving the clinical design of occluders, strictly screening patient indications preoperatively, optimizing device placement during surgery, formulating reasonable anticoagulation strategies postoperatively, and closely monitoring with TEE, the occurrence of DRT in patients can be effectively reduced. Additionally, targeted adjustments to risk factors for patients prone to DRT can also be effective preventive strategies.
Conclusion
DRT is closely related to device treatment and is not only present after LAAC. Based on currently known research results, the overall occurrence rate of DRT post-LAAC is still within an acceptable range; the harm caused by DRT is also controllable, with related stroke occurrence rates approximately 1/10 to 1/15. Therefore, it is essential to conduct standardized anticoagulation treatment postoperatively and to eliminate modifiable factors that trigger DRT in patients as much as possible. In summary, DRT will persist long-term, and clinicians must remain vigilant and proactive in prevention and treatment to help patients achieve better prognostic outcomes.
Further Reading
This content is original from the “Outpatient” magazine. Reproduction must be authorized and please indicate the source.


Official WeChat of “Outpatient” magazine
Long press to identify the QR code and follow