Detection Items
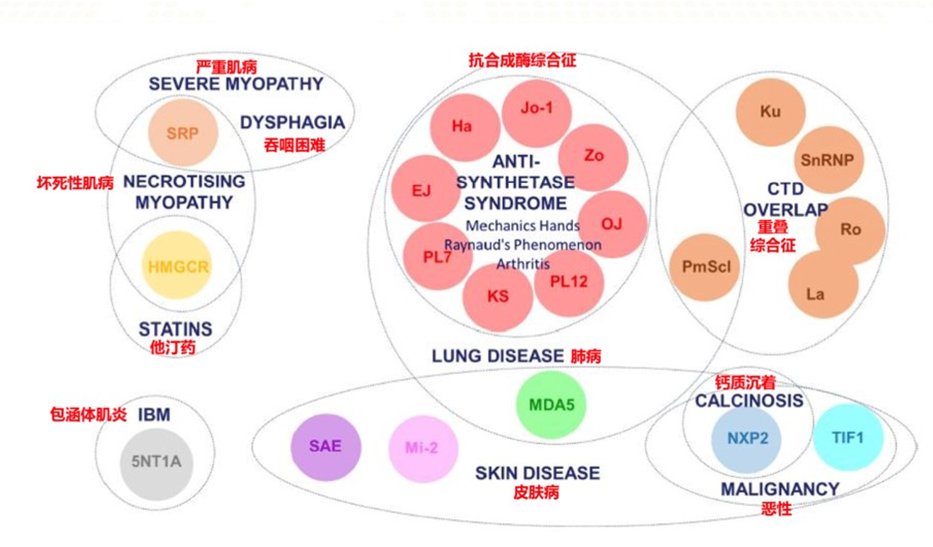
Myositis Antibody Spectrum 19 items (Mi-2, Ku, PM-Scl100, PM-Scl75, Jo-1, SRP, PL-7, PL-12, EJ, Ro-52, TIF1γ, MDA5, NXP2, HMGCR, SAE, OJ, KS, ZO, HA)
Why Detect Myositis Antibody Spectrum?
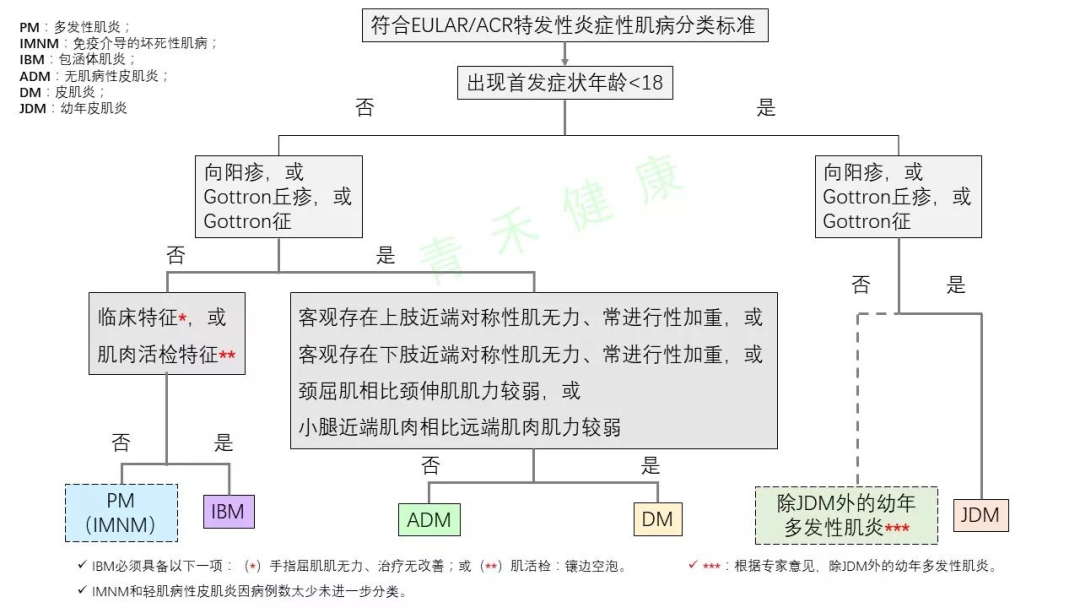
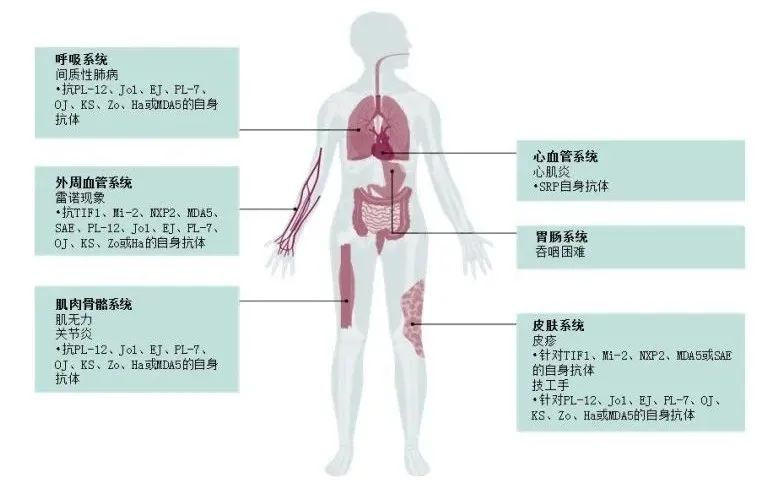
Idiopathic inflammatory myopathy (IIM) is a T cell-mediated autoimmune disease primarily attacking muscle fibers expressing major histocompatibility complex I (MHCI). The clinical manifestations are diverse and highly heterogeneous, mainly divided into five types: (1) dermatomyositis; (2) anti-synthetase syndrome; (3) immune-mediated necrotizing myopathy; (4) polymyositis; (5) sporadic inclusion body myositis. The first three subtypes are the most common in clinical practice.
The epidemiology of IIM is not well studied with large-scale clinical data available. The prevalence of polymyositis and dermatomyositis is between 0.5-1.0/100,000. Females are more affected than males, and it can occur at any age. Without treatment, it usually does not improve on its own, but can benefit from immunotherapy.
The mortality rate is estimated to be 20-30%, with the highest mortality rate occurring in the first year of illness. Adult patients often die due to severe progressive muscle weakness, swallowing difficulties, malnutrition, and respiratory failure caused by aspiration pneumonia or recurrent lung infections.
Laboratory testing is crucial for early diagnosis and treatment of the disease. Abnormal electromyography, inflammatory presence in muscle biopsy, elevated muscle injury markers in blood, the presence of autoantibodies, and response to glucocorticoid treatment are significant.IIMrelated autoantibody testing aids in early diagnosis and differential diagnosis, providing strong evidence for guiding treatment.
Clinical Significance of Autoantibodies
AntiJo-1 Antibody:Has strong specificity for diagnosing polymyositis and dermatomyositis, with a positive rate of about 25% in polymyositis and 7.1% in dermatomyositis. In patients with PM/DM combined with interstitial lung disease, the positive rate can be as high as 60%. Typical symptoms of antiJo-1 positive patients include polyarthritis, arthralgia, non-invasive degenerative arthritis, tenosynovitis, alveolar fibrosis, or pulmonary fibrosis, and symptoms related to scleroderma are also occasionally seen. This syndrome is named anti-synthetase syndrome, derived from other antibodies against aminoacyl-tRNA synthetases that share similar clinical symptoms, of which 75% have interstitial lung disease, 70% have polyarthritis, 60% have Raynaud’s phenomenon, 71% have mechanic’s hands, 87% have fever, occasionally associated with subacute onset and rapidly progressive hypoxemia, responding well to treatment but prone to relapse.
AntiPL-7 Antibody:Recognized as a serum marker antibody for polymyositis (PM) and dermatomyositis (DM), with a positive rate of 3%~4% in myositis patients, having significant clinical value for the diagnosis of PM/DM, primarily seen in the anti-synthetase syndrome subtype of myositis.
AntiPL-12 Antibody:Also a serum marker antibody for polymyositis (PM) and dermatomyositis (DM), with a positive rate of 3% in myositis patients, having significant clinical value for the diagnosis of PM/DM, primarily seen in the anti-synthetase syndrome subtype of myositis, and rare in non-myositis patients.
AntiEJ Antibody:Anti-glycyl-tRNA synthetase antibody, present in myositis, interstitial lung disease, arthritis, Raynaud’s disease, mechanic’s hands, and fever.
AntiSRP Antibody:Appears in 5% of Caucasian adult polymyositis/ dermatomyositis, 8%~13% of Asian adult polymyositis/ dermatomyositis, and 2% of JDM patients, primarily seen in IMNM. Related diseases include necrotizing autoimmune myopathy.
AntiMi-2 Antibody:AntiMi-2 antibody is an antitRNA synthetase antibody that is only found in the serum of adult DM, juvenile DM, PM/DM, and PM patients, especially highly specific for DM. The positive rate of this antibody in adult dermatomyositis is 11%~59%, and in juvenile dermatomyositis (JDM) is 4%~10%. Patients with antiMi-2 antibody positivity typically have milder disease, presenting with arthralgia, arthritis, Raynaud’s phenomenon, and ILD among other clinical manifestations.
AntiMDA-5 Antibody:Anti-melanoma differentiation-associated gene 5, commonly associated with dermatomyositis and interstitial lung disease. This antibody has high diagnostic value for rapidly progressive ILD associated with myositis, with a sensitivity of 77% (95%Cl, 64%~87%), specificity of 86% (95%Cl, 79%~90%), and an area under the curve of 0.89 (95%Cl, 0.63~0.98). Patients with myositis who are positive for this antibody have poorer lung disease outcomes and significantly lower cumulative survival rates compared to those who are antibody negative (P=0.007). Furthermore, the positive rate of antiMDA5 antibody shows regional differences, with a significantly higher positive rate in the Chinese population compared to the Japanese population.
AntiTIF1-γ Antibody:Serum anti-transcription intermediary factor 1-γ antibody, commonly associated with dermatomyositis and malignancies. It is a specific antibody for dermatomyositis, appearing in both adult and pediatric patients, with a frequency of 13%~31% in adult polymyositis/ dermatomyositis and 22%~29% in JDM. Given the role of theTIF1 protein in tumorigenesis, these antibodies may arise due to abnormal anti-tumor immunity in the body.
AntiHMGCR Antibody:3-Hydroxy-3-methylglutaryl-CoA reductase, associated with necrotizing autoimmune myopathy. The positive rate of this antibody is 5.4%, with most patients showing gradual onset, presenting with muscle weakness. This antibody can serve not only as a diagnostic marker but also as a prognostic marker for the disease. Patients positive for antiHMGCR antibody typically present with muscle weakness and swallowing difficulties; clinical management should include tumor screening and long-term immunosuppressive therapy for these patients.
AntiSAE1/2 Antibody:The target antigen is small ubiquitin-like modifier-1 (SUMO-1) activating enzyme (SAE) heterodimerSAE1 andSAE2, found in 8% of dermatomyositis patients. Most positive patients initially present with skin lesions, which can subsequently progress to severe swallowing difficulties.
AntiNXP-2 Antibody:Anti-nuclear matrix protein 2 antibody, recently identified to be associated with adult dermatomyositis with severe skin calcification. Common diseases include dermatomyositis and malignancies. Initially reported in juvenile dermatomyositis, where they are associated with calcinosis, severe muscle weakness, polyarthritis, joint contractures, and intestinal vasculitis. The positive rate in serum of children with juvenile myositis is 23%~25%, and in adult myositis patients is 1%~17%.
AntiOJ Antibody:Anti-isoleucyl-tRNA synthetase antibody, clinical manifestations include interstitial lung disease, arthritis, Raynaud’s phenomenon, mechanic’s hands, less common in myositis, more frequent in dermatomyositis.
AntiKS Antibody:Asparaginyl-tRNA synthetase, clinical manifestations include interstitial lung disease, arthritis, Raynaud’s phenomenon, mechanic’s hands, less common in myositis, some only with interstitial lung disease.
AntiZo Antibody:Anti-phenylalanyltRNA synthetase antibody, related diseases include Antisynthetase syndrome, namely anti-thyroid hormone (anti-synthetase) syndrome.
AntiHA Antibody:Anti-tyrosyl-tRNA synthetase antibody, related diseases include Antisynthetase syndrome, namely anti-thyroid hormone (anti-synthetase) syndrome.
AntiSSA/Ro52kD Antibody:Anti-SSA antibody is mainly seen in primary Sjögren’s syndrome, with a positive rate as high as 60%~75%. Additionally, anti-SSA antibodies are often associated with subacute cutaneous lupus erythematosus, anti-nuclear antibody negative lupus, neonatal lupus, etc. (anti-SSA antibodies can cross the placenta to cause neonatal lupus syndrome).Anti-SSA antibodies are associated with widespread photosensitive dermatitis symptoms.
AntiPM-SCl100 Antibody:Commonly seen in overlapping symptoms of polymyositis and systemic sclerosis, with a positive rate of 50%; it can also appear only in polymyositis patients and diffuse scleroderma.
AntiPM-SCl75 Antibody:Commonly seen in overlapping symptoms of polymyositis and systemic sclerosis, with a positive rate of 50%; it can also appear only in polymyositis patients and diffuse scleroderma.
AntiKu Antibody:Systemic sclerosis, polymyositis, and other connective tissue diseases such as rheumatoid arthritis(RA), mixed connective tissue disease(MCTD), and Sjögren’s syndrome.
Main References:
1.Oldroyd AGS, Lilleker JB, Amin T, et al. British Society for Rheumatology guideline on management of paediatric, adolescent and adult patients with idiopathic inflammatory myopathy.Rheumatology 2022;61(5):1760-1768.
2. Guidelines for the diagnosis and treatment of idiopathic inflammatory myopathy, Chinese Rheumatology Society 2022.5
Source: Medical Laboratory Department, Chongqing Medical University First Affiliated Hospital
The content of this article is copyright of the original author, if there is any infringement, please contact us (or leave a message below this article), thank you!
