Ventricular arrhythmias have always been a challenging peak in the field of arrhythmias due to their high difficulty and risk. In recent years, with advancements in technology and accumulation of experience, the field of catheter ablation for ventricular arrhythmias has made rapid progress.On October 27, the 33rd Great Wall Cardiology Conference and the 2022 Asian Cardiology Conference opened the Ventricular Arrhythmia Forum, where top electrophysiology experts from across the country gathered online to discuss. This forum was divided into five sessions, covering topics from idiopathic ventricular arrhythmias to pathological ventricular tachycardia, from electrophysiological mechanisms to application technologies, providing a detailed academic feast for cardiovascular professionals! Idiopathic Ventricular Arrhythmias (I)
Idiopathic Ventricular Arrhythmias (I)
The first session was hosted by Professor Zhong Jingquan from Shandong University Qilu Hospital and Professor Li Shaolong from Kunming Medical University Affiliated Yan’an Hospital.
Professor Yao Yan from the Fuwai Hospital of the Chinese Academy of Medical Sciences delivered a presentation titled “New Advances in Ventricular Arrhythmias – 2022.” He first introduced the new advancements in catheter ablation strategies for ventricular arrhythmias. Mapping delayed potentials and fragmented potentials followed by substrate ablation can reduce the risks of sustained ventricular tachycardia, asymptomatic ventricular tachycardia, and electrical storm. The PAUSE-SCD study, an international multicenter randomized controlled trial involving Fuwai Hospital, confirmed that early catheter ablation after ICD implantation can reduce the composite outcomes of recurrence, cardiovascular hospitalization, or death in patients with cardiomyopathy ventricular tachycardia compared to antiarrhythmic drugs in the Asian population. The PARTITA study, a multicenter randomized controlled trial conducted in Europe, indicated that catheter ablation immediately after the first ICD discharge can reduce the composite endpoint of all-cause mortality or heart failure hospitalization in patients with cardiomyopathy (mainly ischemic heart disease) and can also reduce the risk of ICD discharges. Another European multicenter randomized controlled trial, the BERLIN VT study, showed that ablation before ICD implantation did not improve all-cause mortality and arrhythmia hospitalization risks in ischemic cardiomyopathy but could reduce the number of ICD discharges postoperatively. Subsequently, Professor Yao introduced research progress in the field of device therapy for ventricular arrhythmias, including percutaneous cardiac ablation, saline-enhanced radiofrequency needle catheter therapy, stereotactic radiotherapy, renal sympathetic nerve ablation, and new tracer techniques for quantitative evaluation of cardiac sympathetic nerve distribution.
Finally, Professor Yao briefly introduced the role of Dapagliflozin in reducing ventricular arrhythmias in patients with HFrEF and related studies.

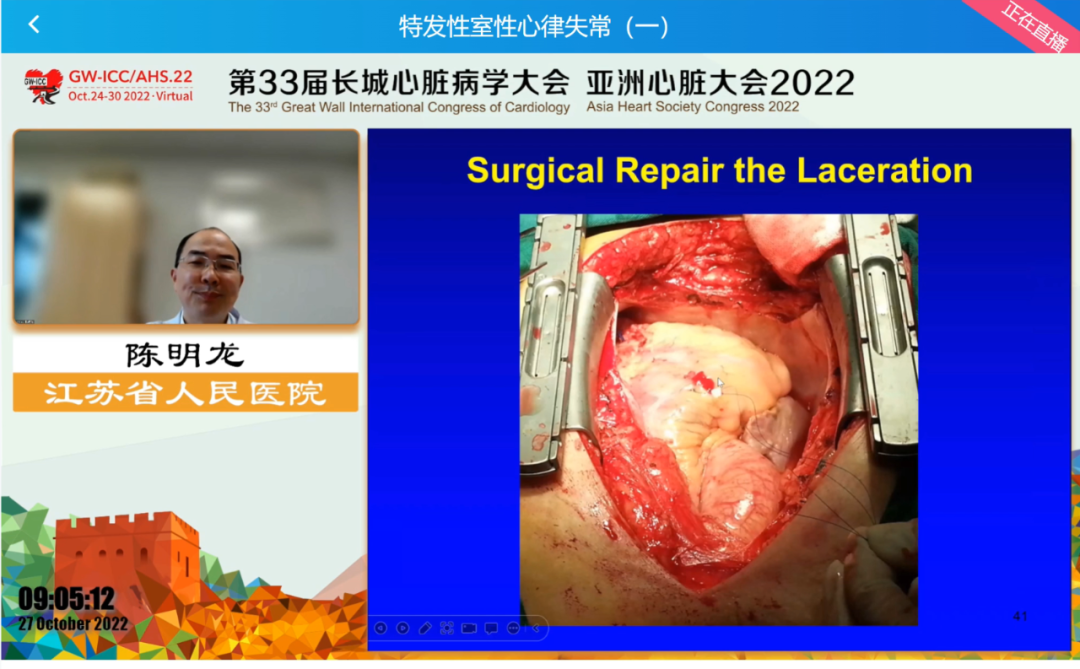
Professor Chen Minglong from Jiangsu Provincial People’s Hospital (Nanjing Medical University First Affiliated Hospital) elaborated on the complications of catheter ablation for ventricular arrhythmias and their prevention and treatment measures. Complications of catheter ablation for ventricular arrhythmias include cardiac perforation, conduction system injury, vascular complications, aortic transvalvular injury, and unique complications of epicardial ablation. Professor Chen introduced the incidence, causes, and details to pay attention to during catheter ablation for each complication, summarizing the response measures after complications based on case studies. Overall, with the application of pressure catheters, intracardiac ultrasound, and other technologies, the understanding of anatomical structures has become clearer, and operators are more cautious during procedures, effectively controlling complications of catheter ablation. Professor Chen emphasized the importance of pre-establishing emergency plans for catheter ablation complications.
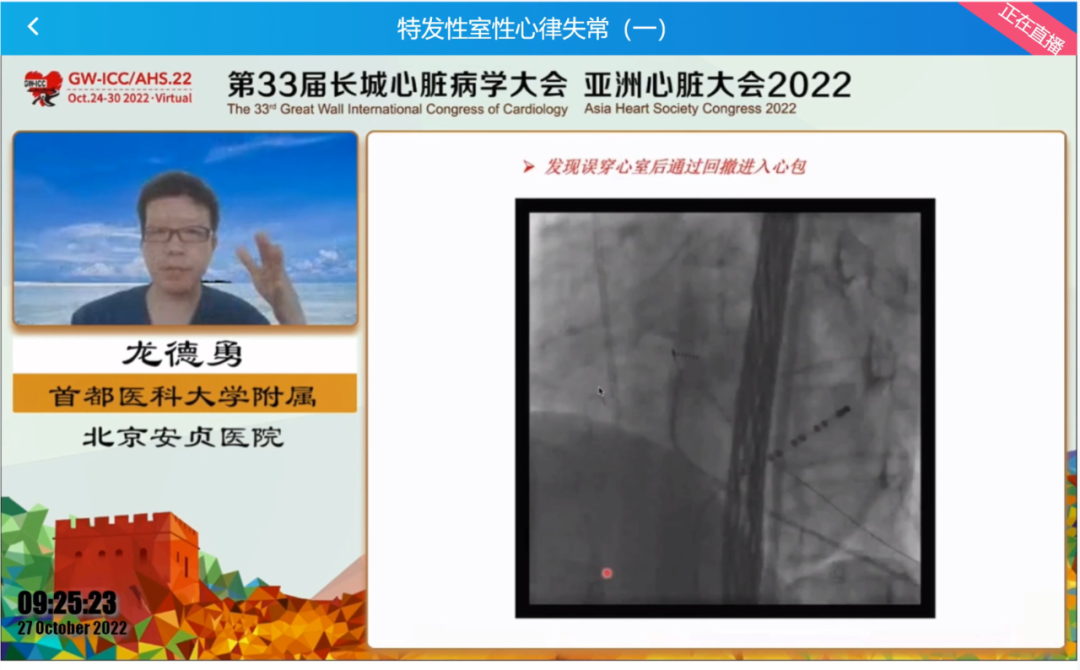
Professor Long Deyong from Capital Medical University Affiliated Beijing Anzhen Hospital began with the pioneers of epicardial ablation, introducing the development of epicardial ventricular tachycardia ablation, and clearly describing the approach, mapping, and ablation of epicardial ventricular tachycardia using anatomical images. Professor Long introduced an innovative modified pericardial puncture method: during puncturing the pericardium, the left lateral position can clearly display the triangle behind the xiphoid process, and without using contrast agents, after entering the triangle behind the xiphoid process, keeping the puncture needle still, pushing the guide wire to feel the heart’s pulsation to roughly locate the pericardial position, retracting the guide wire and then pushing the needle tip to the fibrous pericardium edge, feeling the pericardial pulsation or experiencing a sense of emptiness before pushing the guide wire into the parietal pericardium. Additionally, Professor Long provided detailed explanations of common misconceptions and difficulties encountered during pericardial puncture. Finally, he introduced the characteristics of ventricular tachycardia caused by different etiologies, drag mapping, sinus rhythm sub-potential mapping methods, and the postoperative handling process during epicardial ablation.
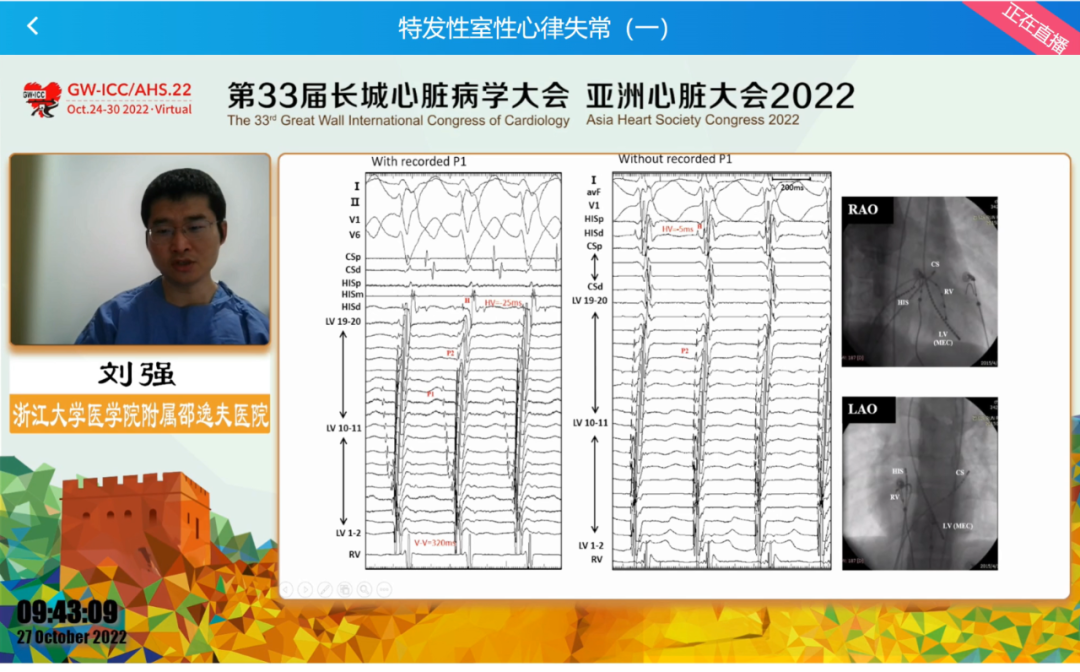
Professor Liu Qiang from Zhejiang University School of Medicine Affiliated Sir Run Run Shaw Hospital introduced a re-understanding of left posterior fascicular ventricular tachycardia based on intracardiac ultrasound. Left posterior fascicular ventricular tachycardia is closely related to the left-sided His-Purkinje system. Professor Liu’s team recorded P1 and P2 potentials during ventricular tachycardia by placing high-density mapping catheters in the left posterior fascicular region, analyzing the activation sequence of P1 and P2 and the HV interval, elucidating the reentrant mechanism and ablation targets of left posterior fascicular ventricular tachycardia, and speculating on the reentrant circuit formation of left posterior fascicular ventricular tachycardia based on the anatomical characteristics of the left posterior fascicle, left posterior septum, and papillary muscles. Finally, Professor Liu concluded that understanding the mechanism of left posterior fascicular ventricular tachycardia, combined with precise mapping under intracardiac ultrasound, can better achieve ablation.
Idiopathic Ventricular Arrhythmias (II)
This session was hosted by Professor Lu Zhibing from Zhongnan Hospital of Wuhan University and Professor Chen Ke from Fuwai Huazhong Cardiovascular Hospital.
Professor Yi Pu from the Air Force Military Medical University Xijing Hospital lectured on the application of intracardiac ultrasound in ventricular arrhythmias. Intracardiac ultrasound has advantages such as non-contact modeling, rapid modeling; different structures superimposed and combined, three-dimensional structures are clear at a glance; clearer display of anatomical details; guiding catheter positioning and contact. Professor Yi detailed the recognition of anatomical details by intracardiac ultrasound, pointing out its important role in the precise mapping of arrhythmias originating from papillary muscles, understanding the anatomy and electrophysiological mechanisms of false tendons, recognizing the folding structure of valve rings, the connection points of pulmonary valve, and the evidence of irregular thickening of ventricular myocardium in arrhythmogenic right ventricular cardiomyopathy. During ablation, intracardiac ultrasound combined with pressure catheters can achieve more precise catheter contact.

Professor Tao Hailong from Zhengzhou University First Affiliated Hospital introduced the electrical anatomical mapping, electrocardiographic localization, and catheter operation techniques for early ventricular ectopic beats originating from the valve ring. He particularly detailed the distribution, electrocardiographic characteristics, catheter positioning methods, and ablation power for early ventricular ectopic beats originating from the mitral and tricuspid valve rings.

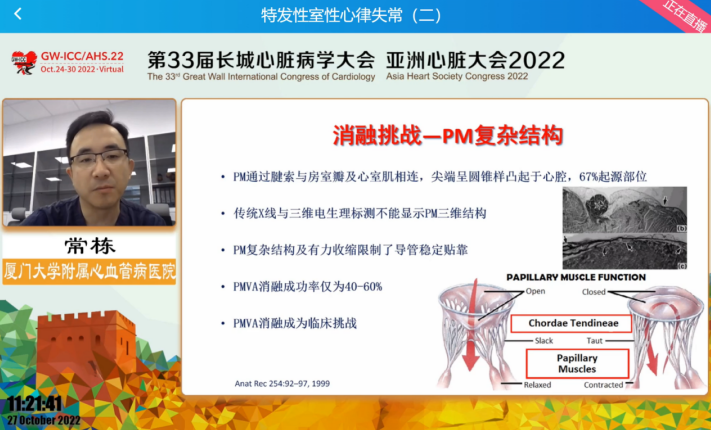
Professor Chang Dong from Xiamen University Affiliated Cardiovascular Hospital shared insights on false tendons and ventricular arrhythmias. The anatomy of the ventricles is complex, and the structure of false tendons was discovered over 100 years ago, with a high incidence and often multiple occurrences. False tendons contain Purkinje fibers, and increased automaticity may be a mechanism for their ventricular arrhythmias. Due to the complex structure of false tendons, their fine pathways, and multiple exits, ultrasound assistance is often required to complete ablation. Special manifestations such as P potentials and inverted potentials during mapping and ablation help determine ablation targets. Finally, Professor Chang further analyzed the electrical characteristics of ventricular arrhythmias at the false tendon site and the differentiation methods from papillary muscle-related ventricular arrhythmias based on case studies.
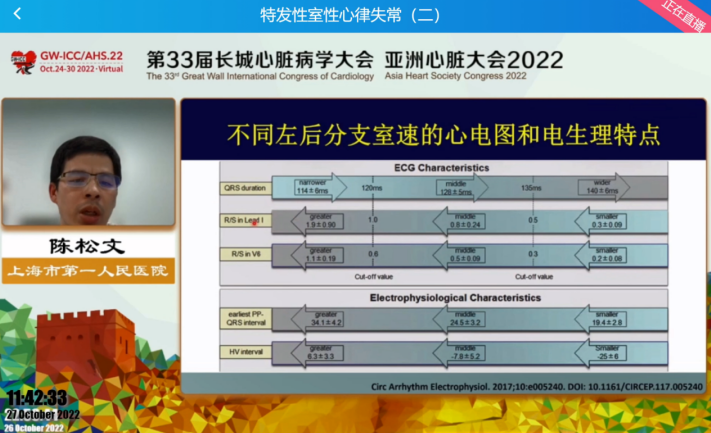
Professor Chen Songwen from Shanghai First People’s Hospital shared the mapping and ablation of left posterior fascicular ventricular tachycardia. Professor Chen first introduced the anatomy of the His-Purkinje system and the mechanisms of ventricular arrhythmias originating from the His-Purkinje system, then detailed the electrocardiographic characteristics and electrophysiological features of left posterior fascicular ventricular tachycardia at proximal, mid, and distal exits. Professor Chen also summarized the current understanding of P1 and P2 potentials based on research by Professor Liu Qiang and others. P2 is the left posterior fascicular potential activated by P1 during ventricular tachycardia, which transmits activation to the apex and retroactively activates the proximal bundle branch and His. P1 is the late diastolic potential recorded during ventricular tachycardia, which is connected to the ventricular myocardium at the proximal end (with slow conduction characteristics) and connected to P2 at the distal end, serving as a key component of the reentrant circuit and ablation target. Finally, Professor Chen illustrated the ablation strategy for left posterior fascicular ventricular tachycardia based on cases and research from his team, emphasizing the need to conduct ablation based on a deep understanding of its electrophysiological mechanisms to avoid unnecessary complications such as left bundle branch block due to blind ablation.
Pathological Ventricular Tachycardia (I)
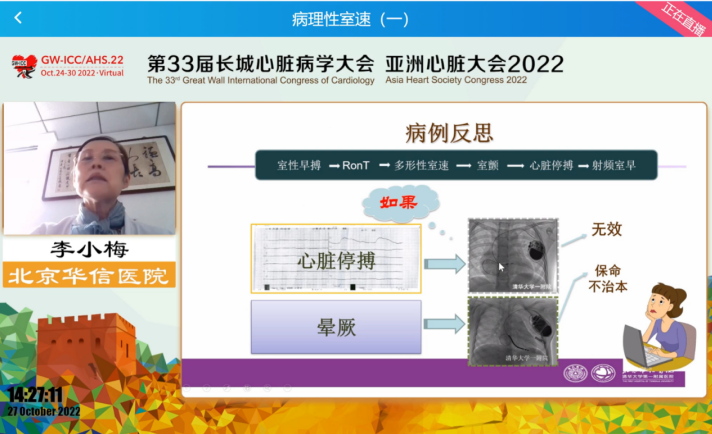
This section was hosted by Professor Zheng Lihui from Fuwai Hospital of the Chinese Academy of Medical Sciences and Professor Li Kang from Peking University First Hospital. Professor Li Xiaomei from Beijing Huaxin Hospital (Tsinghua University First Affiliated Hospital) began by discussing the incidence of ventricular arrhythmias in children, introducing comprehensive management of pediatric ventricular arrhythmias and correcting misconceptions regarding treatment. Ventricular premature beats are common in children, with an incidence ranging from 10% to 30% depending on age. For children, the total number of heartbeats varies at different stages, thus defining frequent ventricular premature beats as >10% burden. Most idiopathic ventricular arrhythmias have a good prognosis, may self-resolve in infancy, and may persist for a long time in childhood. However, since arrhythmias in children are usually benign, most do not require treatment. The need for treatment should be determined based on the child’s age, symptoms, specific diagnosis, and the hemodynamic impact of the arrhythmia. It is particularly important to note that antiarrhythmic drugs do not provide sustained improvement, so they are generally not recommended; some children may consider catheter ablation for a cure. Subsequently, Professor Li Xiaomei shared practical experiences in catheter ablation for arrhythmias in children at outflow tracts, tricuspid valve rings, and left posterior papillary muscles, and shared a case of ablation for ventricular tachycardia induced by “R on T” leading to syncope. As there are no catheters specifically designed for children, Professor Li Xiaomei and her team had to overcome numerous difficulties during the ablation process, but they remain committed to fighting on the front lines for the children, paying tribute to pediatric electrophysiology experts!
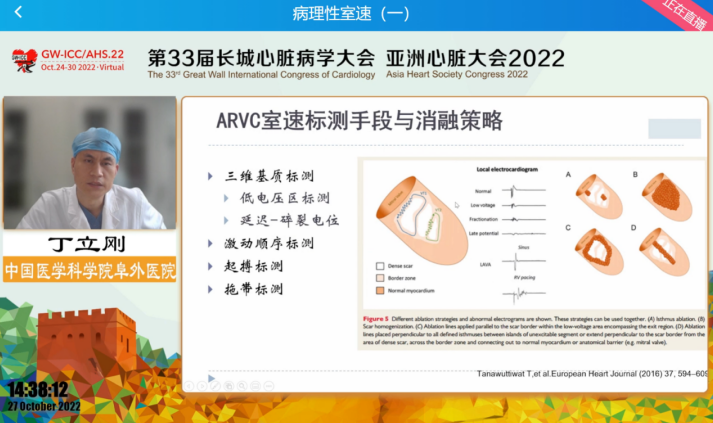
Professor Ding Ligang from Fuwai Hospital of the Chinese Academy of Medical Sciences introduced the ablation strategies and evaluations for arrhythmogenic right ventricular cardiomyopathy (ARVC). The challenges of mapping ventricular tachycardia in ARVC mainly lie in the difficulty of inducing tachycardia and hemodynamic instability after induction. Key issues during ablation include whether to choose linear or planar ablation, how to judge ablation endpoints, and how to balance safety and efficacy. Rapid burst stimulation helps induce ARVC ventricular tachycardia. The lesion range of endocardial and epicardial mapping differs, and multiple meta-analyses show that combined endocardial and epicardial mapping and ablation are superior to purely endocardial mapping and ablation. However, due to the thin ventricular walls in ARVC, care should be taken during pericardial puncture to avoid accidental puncture of the ventricle. In addition to voltage substrate mapping, fragmented potentials and delayed potentials should also be recorded. The delayed potentials mapped under sinus rhythm are key isthmuses for ventricular tachycardia and can serve as ablation targets. Some hemodynamically stable patients may combine drag mapping. The key to determining ablation strategies is to find the critical isthmus, and planar ablation is usually required to achieve complete block. The current recognized endpoint for ablation is when ventricular tachycardia can no longer be induced and delayed potentials are completely ablated.
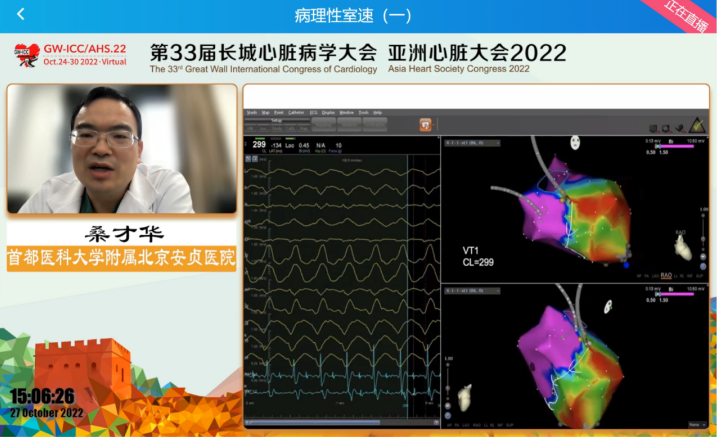
Professor Sang Caihua from Capital Medical University Affiliated Beijing Anzhen Hospital introduced the mapping and ablation strategies for post-myocardial infarction ventricular tachycardia. Although post-myocardial infarction ventricular tachycardia and cardiomyopathy ventricular tachycardia have differences, both are reentrant mechanisms, so clearly mapping the reentrant circuit is a prerequisite for ablation. Except for inferior wall myocardial infarction, post-myocardial infarction ventricular tachycardia mainly involves the endocardium. Classic electrophysiology textbooks have clearly stated that the reentrant circuit of ventricular tachycardia consists of exit, entrance, isthmus, outer loop, and inner loop. Late diastolic potentials, and the proximity of S-QRS and EGM-QRS during drag mapping suggest that the mapping point is located at the critical isthmus. Mapping the reentrant circuit and determining the critical isthmus, followed by planar ablation of possible critical isthmuses, is the strategy for ablation of post-myocardial infarction ventricular tachycardia.
Professor Wang Jing from Fuwai Hospital of the Chinese Academy of Medical Sciences summarized the mechanisms of ventricular tachycardia associated with ventricular aneurysms and the management strategies during mapping and ablation. Ventricular tachycardia associated with ventricular aneurysms is scar-mediated and mainly involves reentrant mechanisms involving the endocardium. First, electroanatomical mapping should be performed under sinus rhythm to identify dense scar areas, scar margins, fragmented potentials, and late potentials within the heart cavity. The scar margin is the critical isthmus for reentry formation, while late potentials are the blind ends of reentry, and isolated late diastolic potentials indicate slow conduction areas, thus the location of late diastolic potentials is the critical pathway for reentry formation. Additionally, pacing mapping S-QRS intervals are also important methods for determining the entrance, exit, and critical isthmus of the reentry pathway. During ablation, it is necessary to block and isolate the channel, and late potentials within the scar area should also be homogenized during ablation.

Pathological Ventricular Tachycardia (II)
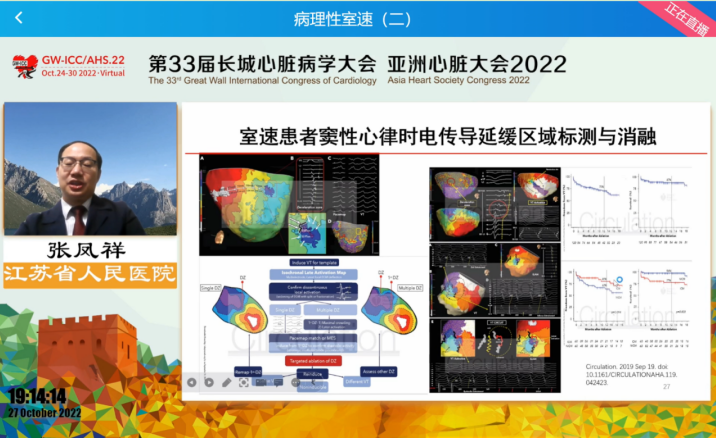
This session was hosted by Professor Wang Xuezhong from Ningxia Medical University General Hospital and Professor Zhang Zhiguo from Jilin University First Hospital. Professor Zhang Fengxiang from Jiangsu Provincial People’s Hospital (Nanjing Medical University First Affiliated Hospital) reviewed the latest research on mapping and ablation of ventricular tachycardia associated with structural heart disease. He introduced methods such as scar channel mapping, local abnormal ventricular activation, scar nucleus isolation, homogenized ablation, S2 stimulation decremental activation mapping, ultra-high-density mapping, three-dimensional mapping of ventricular tachycardia, and MRI-guided mapping of ventricular tachycardia, showcasing the applications of alcohol ablation, radiotherapy, needle-tip ablation catheters, renal sympathetic nerve ablation, hybrid surgery, and cardiac transplantation when necessary in the treatment of ventricular tachycardia associated with structural heart disease.
Professor Sun Yaxun from Zhejiang University School of Medicine Affiliated Sir Run Run Shaw Hospital brought us insights into the diagnosis and management of hereditary arrhythmias. He provided detailed explanations on the etiology, risk stratification, pharmacological and non-pharmacological treatment options, and prevention strategies for malignant arrhythmias in hereditary arrhythmias such as Long QT syndrome, Brugada syndrome, catecholaminergic polymorphic ventricular tachycardia, and Short QT syndrome. Professor Sun pointed out that hereditary arrhythmias can lead to sudden cardiac death, and it is essential to avoid or reduce triggers; in addition to accessible pharmacological treatments, ICD therapy should be considered for high-risk patients, and surgical interventions should be actively pursued for patients with indications.

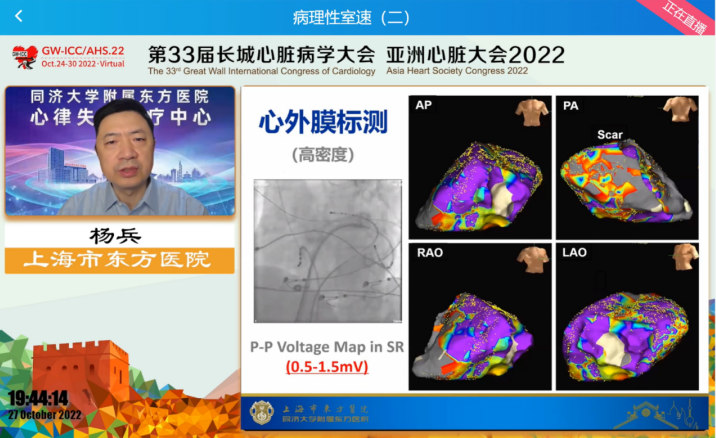
Professor Yang Bing from Shanghai East Hospital (Tongji University Affiliated East Hospital) shared insights on high-density mapping of ventricular tachycardia associated with structural heart disease. Starting from a case of ablation for a storm of ventricular tachycardia associated with structural heart disease, Professor Yang introduced the main mechanisms, mapping, and ablation strategies for ventricular tachycardia associated with structural heart disease. High-density or ultra-high-density mapping can reveal the substrate and reentrant pathways of ventricular tachycardia associated with structural heart disease. It is important to note that the reentrant circuits of ventricular tachycardia associated with structural heart disease usually involve the endocardium, mid-myocardium, and epicardium, and analyzing mapping solely from the endocardial or epicardial surface cannot fully explain the mechanisms of ventricular tachycardia. Therefore, three-dimensional mapping combined with high-density mapping may better reveal the specific mechanisms of myocardial mid-layer and subepicardial myocardium involved in the occurrence of ventricular tachycardia.
Professor Jiang Chenxi from Capital Medical University Affiliated Beijing Anzhen Hospital introduced the techniques of dry pericardial puncture. He provided detailed explanations on the necessity of dry pericardial puncture, puncture approaches, specific operational processes, and the issues and solutions that need attention at each stage. Professor Jiang compared the guide wire guidance methods during dry pericardial puncture with the characteristics of contrast agent visualization during ordinary pericardial puncture, pointing out the unique advantages of dry pericardial puncture.

From anatomy to mechanisms, from basic to clinical, from the rich and diverse idiopathic ventricular arrhythmias to the complex and high-risk pathological ventricular tachycardia, five sessions, 21 speakers, and 10 expert hosts, this forum provided a wealth of electrophysiological academic content for cardiovascular doctors! The Ventricular Arrhythmia Forum concluded successfully! Thanks to all the hardworking experts and actively participating clinicians, and to all the staff of the conference organizing committee!
In October, there is an appointment in the “air”!