Recommended Articles:Collect | “Guidelines for Patients with Primary Liver Cancer by the Chinese Anti-Cancer Association”“Collection of 28 Guidelines for Rational Drug Use in Common Diseases at the Grassroots Level (Download PDF)”
“Collection of 82 Guidelines for Diagnosis and Treatment of Common Diseases at the Grassroots Level”
Protective Equipment Donning and Doffing Video (National Health Commission COVID-19 Medical Treatment Expert Group)
A Systematic Review of 14 HBV-Related Liver Cancer Prediction Models: REAL-B Shows the Best Predictive Ability
 Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2022 Edition)01Overview
Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2022 Edition)01Overview
Primary liver cancer is currently the 4th most common malignant tumor and the 2nd leading cause of cancer-related death in China, posing a serious threat to the lives and health of the Chinese people. Primary liver cancer mainly includes three different pathological types: hepatocellular carcinoma (Hepatocellular carcinoma, HCC), intrahepatic cholangiocarcinoma (Intrahepatic cholangiocarcinoma, ICC), and combined hepatocellular-cholangiocarcinoma (Combined hepatocellular-cholangiocarcinoma, cHCC-CCA). There are significant differences among the three in terms of pathogenesis, biological behavior, histopathology, treatment methods, and prognosis. HCC accounts for 75%-85%, while ICC accounts for 10%-15%. In this guideline, “liver cancer” refers only to HCC.
To further standardize the diagnosis and treatment of liver cancer in China, in June 2017, the former National Health and Family Planning Commission released the “Diagnosis and Treatment Norms for Primary Liver Cancer (2017 Edition)”. The National Health Commission updated it in December 2019. The “Diagnosis and Treatment Norms for Primary Liver Cancer (2019 Edition)” reflected the status of liver cancer diagnosis, multidisciplinary comprehensive treatment, and research at that time in China. It played an important role in standardizing the diagnosis and treatment of liver cancer, improving the prognosis of liver cancer patients, ensuring medical quality and safety, and optimizing medical resources. Since the release of the “Diagnosis and Treatment Norms for Primary Liver Cancer (2019 Edition)”, many high-level evidence consistent with evidence-based medicine principles have emerged in the diagnosis, staging, and treatment of liver cancer, especially research results suitable for China’s national conditions have been published one after another. Therefore, the National Health Commission entrusted the Oncology Branch of the Chinese Medical Association to jointly organize multidisciplinary experts in the field of liver cancer, in conjunction with the Liver Cancer Professional Committee of the Chinese Anti-Cancer Association, the Ultrasound Medicine Branch of the Chinese Medical Association, the Surgical Physicians Branch of the Chinese Physician Association, and the Interventional Physicians Branch of the Chinese Physician Association, to revise and update the “Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2022 Edition)” again, aiming to promote the implementation of and achieve the goal of increasing the 5-year survival rate of liver cancer patients by 15% as outlined in the “Healthy China 2030” planning outline.
The evidence evaluation and recommendation grading methodology (Grading of Recommendations, Assessment, Development and Evaluation, GRADE) is currently the most widely used evidence evaluation and recommendation grading system. The GRADE system consists of two parts: the first part is evidence evaluation, which classifies the quality of evidence into four levels: high, moderate, low, and very low, based on bias risk, inconsistency, indirectness, imprecision, and publication bias in the evidence. The second part is recommendation grading, where the GRADE system considers the balance of benefits and harms of medical interventions, the quality of evidence, values and preferences, and costs and resource use to formulate recommendations, classifying recommendations into strong recommendations and weak recommendations (conditional recommendations). The greater the difference in benefits and harms of medical interventions, the higher the quality of evidence, the clearer and more aligned the values and preferences, and the smaller the costs and resource use, the more strongly a recommendation should be considered. Conversely, weak recommendations (conditional recommendations) should be considered. The evidence grading assessment in this guideline refers to the above GRADE grading guidelines and uses the “Oxford Centre for Evidence-Based Medicine Levels of Evidence 2011 Edition” as an auxiliary tool for specific implementation of evidence grading (Appendix 1). In converting evidence into recommendations, the expert group mainly referred to the aforementioned GRADE guidelines for recommendation grading but also made corresponding modifications to the recommendation grading based on the ASCO guidelines (Appendix 2). Ultimately, the strength of recommendations is divided into three levels: strong recommendation, moderate recommendation, and weak recommendation. A strong recommendation indicates that the expert group reflects high confidence in the recommendation reflecting best clinical practice, and the vast majority, if not all, target users should adopt the recommendation. A moderate recommendation indicates that the expert group reflects moderate confidence in the recommendation reflecting best clinical practice, and most target users will adopt the recommendation, but attention should be paid to shared decision-making between doctors and patients during implementation. A weak recommendation indicates that the expert group reflects some confidence in the recommendation reflecting best clinical practice, but it should be conditionally applied to the target population, emphasizing shared decision-making between doctors and patients.
02Screening and Diagnosis
(1) Screening and Monitoring of High-Risk Groups for Liver Cancer.
Screening and monitoring of high-risk groups for liver cancer is crucial for early detection, diagnosis, and treatment, which is key to improving liver cancer treatment outcomes. Rapid and convenient identification of high-risk groups for liver cancer is a prerequisite for implementing widespread screening, while stratified assessment of the population’s liver cancer risk is the basis for formulating different liver cancer screening strategies. In China, high-risk groups for liver cancer mainly include individuals infected with hepatitis B virus (Hepatitis B virus, HBV) and/or hepatitis C virus (Hepatitis C virus, HCV), excessive alcohol consumption, non-alcoholic fatty liver disease, cirrhosis from other causes, and those with a family history of liver cancer, especially males over 40 years old. Currently, although antiviral treatments for HBV and HCV can significantly reduce the risk of liver cancer, they cannot completely prevent its occurrence. The liver cancer risk assessment model aMAP score (age-Male-AlBi-Platelets score) developed by Chinese scholars can quickly and easily stratify liver disease populations into low-risk (0-50 points), moderate-risk (50-60 points), and high-risk (60-100 points) groups, with annual incidence rates of liver cancer for each group being 0-0.2%, 0.4%-1%, and 1.6%-4%, respectively, which helps identify high-risk groups for liver cancer (evidence level 2, recommendation B). Utilizing liver ultrasound imaging and serum alpha-fetoprotein (Alpha-fetoprotein, AFP) for early screening of liver cancer is recommended for high-risk groups to undergo at least one examination every six months (evidence level 2, recommendation A). By implementing a new integrated screening model in communities and hospitals, it is essential to ensure that screenings are conducted thoroughly and treatments are initiated early.
(2) Imaging Examinations for Liver Cancer.
Various imaging examination methods have their characteristics, and comprehensive application, complementary advantages, and overall assessment should be emphasized.
1. Ultrasound Imaging.
Ultrasound imaging has advantages such as convenience, real-time capability, non-invasiveness, and no radiation exposure, making it the most commonly used imaging method for the liver in clinical practice. Routine grayscale ultrasound imaging can sensitively detect intrahepatic space-occupying lesions early, differentiate whether they are cystic or solid, and preliminarily judge benign or malignant. At the same time, grayscale ultrasound imaging can comprehensively screen for metastases in other organs in the liver or abdominal cavity, as well as assess whether there is intraparenchymal vascular and bile duct invasion. Color Doppler flow imaging can observe the blood supply status of lesions, assist in judging the benignity or malignancy of lesions, show the proximity of lesions to important intrahepatic blood vessels, and assess whether there is vascular invasion, and it can also preliminarily judge the efficacy of local treatments after liver cancer treatment. Ultrasound contrast examination can dynamically observe changes in blood flow perfusion in liver tumors, differentiate between different types of liver tumors, and can sensitively detect hidden small lesions during surgery, dynamically guide local treatment, and assess the efficacy of local treatment for liver cancer postoperatively (evidence level 3, recommendation A). The combination of ultrasound and imaging navigation technology provides effective technical means for precise localization and ablation of liver cancer, especially for hidden liver cancer that cannot be displayed by conventional ultrasound imaging (evidence level 4, recommendation B). Ultrasound shear wave elastography can quantitatively assess the hardness of liver tumors and the degree of fibrosis/scarring in surrounding liver tissue, providing useful information for planning reasonable liver cancer treatment (evidence level 4, recommendation B). The combined application of multimodal ultrasound imaging technology plays an important role in the precise preoperative diagnosis, intraoperative localization, and postoperative assessment of liver cancer.
2. CT and MRI.
Dynamic enhanced CT and multiparametric MRI scanning are the preferred imaging examination methods for confirming the diagnosis of liver cancer in patients with abnormal liver ultrasound and/or serum AFP screening. Dynamic enhancement CT/MR (Gadobenate dimeglumine/Gadobutrol) dynamic enhancement three-phase scans include: arterial late phase (portal vein begins to enhance; usually scanned around 35 seconds after contrast injection), portal phase (portal vein fully enhances; hepatic veins can see contrast filling; liver parenchyma usually reaches peak enhancement; usually scanned 60-90 seconds after contrast injection), and delayed phase (both portal vein and hepatic vein enhance but lower than portal phase; liver parenchyma shows enhancement but lower than portal phase; usually scanned 3 minutes after contrast injection). Hepatocyte-specific magnetic resonance contrast agent (Gadobenate dimeglumine, Gd-EOB-DTPA) dynamic enhancement four-phase scans include: arterial late phase (same as above), portal phase (same as above), transitional phase (liver vascular and liver parenchyma signal intensity is the same; liver enhancement is produced by the synergistic effect of intracellular and extracellular; usually scanned 2-5 minutes after Gd-EOB-DTPA injection), and liver-bile duct specificity (liver parenchyma signal is higher than liver blood vessels; contrast agent is excreted via the bile duct system; usually scanned 20 minutes after Gadobenate dimeglumine injection). Currently, liver CT plain and dynamic enhanced scans are commonly used not only for clinical diagnosis and staging of liver cancer but also for evaluating the efficacy of local treatment for liver cancer, especially advantageous for observing the deposition status of iodinated oil after transcatheter arterial chemoembolization (TACE). Radiomics technology based on preoperative CT can also be used to predict the efficacy of the first TACE treatment. Meanwhile, post-processing CT technology can be used for three-dimensional vascular reconstruction, liver volume and liver tumor volume measurement, and evaluation of metastases in other organ tissues such as lungs and bones, and has been widely used in clinical practice.
Multiparametric MRI of the liver has advantages such as no radiation exposure, high tissue resolution, and the ability to perform multi-parameter imaging from multiple angles and sequences, and it has comprehensive imaging capabilities that combine morphology and function (including diffusion-weighted imaging) and has become the preferred imaging technique for clinical detection, diagnosis, staging, and efficacy evaluation of liver cancer. The detection and diagnostic capability of multiparametric MRI for liver cancer with a diameter of ≤2.0 cm is superior to that of dynamic enhanced CT (evidence level 1, recommendation A). Multiparametric MRI has advantages over dynamic enhanced CT in evaluating whether liver cancer invades the portal vein, major hepatic veins, and their branches, as well as lymph node metastases in the abdominal cavity or retroperitoneal space. When evaluating the efficacy of local treatment for liver cancer using multiparametric MRI scanning, it is recommended to use the modified response evaluation criteria in solid tumors (mRECIST) combined with T2-weighted imaging and diffusion-weighted imaging for comprehensive judgment.
The imaging diagnosis of liver cancer is mainly based on the enhancement pattern of “fast in and fast out” in dynamic enhancement scans (evidence level 1, recommendation A). In the arterial phase (mainly in the arterial late phase), liver tumors show uniform or uneven significant enhancement, while in the portal phase and/or delayed phase, the enhancement of liver tumors is lower than that of liver parenchyma. “Fast in” refers to non-circular enhancement, while “fast out” refers to non-peripheral clearing. “Fast in” is observed in the arterial late phase, while “fast out” is observed in the portal and delayed phases. Gd-EOB-DTPA can only observe the “fast out” sign in the portal phase, while the transitional and liver-bile duct specific phases can serve as auxiliary malignant signs.
Gd-EOB-DTPA enhanced MRI examination shows that liver tumors exhibit significant enhancement in the arterial phase, while enhancement in the portal phase is lower than that of liver parenchyma, and the liver-bile duct specificity phase often shows significantly low signal. In 5%-12% of well-differentiated small liver cancers, the liver-bile duct specificity phase may show slightly higher signal due to contrast agent absorption.
The multiparametric MRI scan for liver cancer, especially for diagnosing tumors with a diameter of ≤2.0 cm/<1.0 cm, emphasizes that it still requires comprehensive judgment in conjunction with other signs (such as capsule-like enhancement, intermediate signal in T2-weighted imaging, and diffusion restriction) and threshold growth [50% increase in maximum diameter of lesions within 6 months (inclusive)] (evidence level 3, recommendation A). Capsule-like enhancement is defined as smooth, uniform, and clearly defined, mostly or entirely surrounding the lesion, especially exhibiting ring-like enhancement in the portal, delayed, or transitional phases.
The combined application of Gd-EOB-DTPA enhanced MRI examination with low signal specificity in the liver-bile duct, arterial phase enhancement, and diffusion restriction signs can significantly improve the diagnostic sensitivity of liver cancer with a diameter of <1.0 cm (evidence level 2, recommendation B), especially for patients with liver cirrhosis, and is strongly recommended for this method, which also helps differentiate high-grade dysplastic nodules (HGDN) and other precancerous lesions (evidence level 3, recommendation B).
Clinical data mining based on liver cancer CT and/or MRI information to establish fusion models can help improve clinical decision-making (patient treatment plan selection, efficacy evaluation, and prediction, etc.). For preoperative prediction of microvascular invasion (MVI) in liver cancer, the specificity of imaging signs is high, but sensitivity is low. Nomograms and imaging models may be potential breakthroughs for preoperative prediction of MVI (evidence level 3, recommendation B).
3. Digital Subtraction Angiography.
Digital subtraction angiography (DSA) is a minimally invasive examination that uses selective or super-selective hepatic artery for DSA examination. This technique is more commonly used in local treatment of liver cancer or treatment of spontaneous rupture bleeding in liver cancer. DSA examination can show the blood vessels of liver tumors and the staining of liver tumors, as well as clearly show the number, size, and blood supply conditions of liver tumors.
4. Nuclear Medicine Imaging Examination.
(1) Positron Emission Tomography-CT (PET-CT), Fluorine-18-Fluorodeoxyglucose (18F-FDG) PET-CT whole-body imaging has the following advantages:
① Staging tumors, evaluating lymph node metastases and distant organ metastases through one examination (evidence level 1, recommendation A);
② Restaging, as PET-CT functional imaging is not affected by anatomical structures, it can accurately show recurrence and metastasis after anatomical structure changes or in complex anatomical areas (evidence level 3, recommendation B);
③ More sensitive and accurate efficacy evaluation for targeted drugs that inhibit tumor activity (evidence level 3, recommendation A);
④ Guiding the delineation of biological target areas for radiotherapy and determining puncture biopsy sites;
⑤ Evaluating tumor malignancy and prognosis (evidence level 1, recommendation B).
PET-CT has limited sensitivity and specificity for diagnosing liver cancer and can serve as an auxiliary and complementary to other imaging examinations, showing advantages in the staging, restaging, and efficacy evaluation of liver cancer. PET imaging using carbon-11-labeled acetate (11C-acetate) or choline (11C-choline) can improve the sensitivity of diagnosing well-differentiated liver cancer, complementing 18F-FDG PET-CT imaging.
(2) Single Photon Emission Computed Tomography-CT (SPECT-CT):
SPECT-CT has gradually replaced SPECT as the mainstream device for nuclear medicine single-photon imaging. Selecting lesions found in whole-body planar imaging and then conducting local SPECT-CT fusion imaging can significantly improve diagnostic accuracy (evidence level 3, recommendation A).
(3) Positron Emission Tomography-MRI (PET-MRI):
One PET-MRI examination can simultaneously obtain anatomical and functional information about the disease, improving the sensitivity of liver cancer diagnosis (evidence level 4, recommendation C).
(3) Hematological Molecular Markers for Liver Cancer.
Serum AFP is currently a commonly used and important indicator for diagnosing liver cancer and monitoring efficacy. Serum AFP ≥400μg/L, after excluding pregnancy, chronic or active liver disease, germ cell tumors, and gastrointestinal tumors, highly suggests liver cancer; while those with mildly elevated serum AFP should be combined with imaging examinations or monitored dynamically, and analyzed in comparison with liver function changes to aid diagnosis. Abnormal prothrombin (Protein induced by vitamin K absence/antagonist-Ⅱ, PIVKAⅡ; Des-gamma carboxyprothrombin, DCP), plasma free microRNA (microRNA, miRNA), and serum AFP heterogeneity (Lens culinaris agglutinin-reactive fraction of AFP, AFP-L3) can also serve as early diagnostic markers for liver cancer, especially for AFP-negative populations (evidence level 1, recommendation A). The GALAD model based on gender, age, AFP, PIVKAⅡ, and AFP-L3 has a sensitivity of 85.6% and specificity of 93.3% for early diagnosis of liver cancer, aiding early diagnosis of AFP-negative liver cancer (evidence level 2, recommendation A). An optimized GALAD-like model based on large-sample data from the Chinese population has been used for early diagnosis of liver cancer. A detection kit based on 7 miRNAs has a sensitivity and specificity of 86.1% and 76.8% for diagnosing liver cancer, with sensitivity and specificity of 77.7% and 84.5% for AFP-negative liver cancer, respectively (evidence level 2, recommendation A). For other novel hematological molecular markers for early diagnosis and efficacy evaluation of liver cancer, see Appendix 3.
(4) Liver Biopsy.
Patients with liver space-occupying lesions exhibiting typical imaging characteristics of liver cancer and meeting clinical diagnostic criteria for liver cancer usually do not require liver lesion biopsy for diagnostic purposes (evidence level 1, recommendation A), especially for liver cancer patients with surgical indications. For liver cancer patients who can undergo surgical resection or are preparing for liver transplantation, preoperative liver lesion biopsy is not recommended to reduce the risk of tumor rupture, bleeding, and dissemination. For liver space-occupying lesions lacking typical imaging characteristics of liver cancer, liver lesion biopsy can provide a clear pathological diagnosis. Liver lesion biopsy can clarify the nature of the lesion and the molecular typing of liver cancer, providing valuable information for clarifying the cause of liver disease, guiding treatment, assessing prognosis, and conducting research. Therefore, the necessity of biopsy should be comprehensively assessed based on the benefits to patients undergoing liver lesion biopsy, potential risks, and the physician’s operational experience.
Liver lesion biopsy is usually performed under ultrasound or CT guidance, using an 18G or 16G liver puncture needle to obtain tissue from the lesion. The main risks include possible bleeding and tumor needle track seeding. Therefore, preoperative assessments of platelet count and coagulation function should be conducted, and liver lesion biopsy should be avoided in patients with severe bleeding tendencies. The puncture path should ideally pass through normal liver tissue, avoiding direct puncture of the surface nodules of the liver. The puncture site should be selected within the tumor and adjacent to the tumor, and the integrity of the sampled tissue should be observed with the naked eye to improve diagnostic accuracy. Additionally, due to various factors such as lesion size and depth, liver lesion biopsy also has a certain false-negative rate, especially for lesions ≤2 cm in diameter, where the false-negative rate is relatively high. Therefore, negative results from liver lesion biopsy do not completely rule out the possibility of liver cancer, and close monitoring and regular follow-up are still necessary. For patients with insufficient biopsy tissue, negative pathological results but a high clinical suspicion of liver cancer, repeat liver lesion biopsy or close follow-up can be conducted.
Key Points Discussion
(1) Early screening for liver cancer using liver ultrasound imaging combined with serum AFP is recommended for high-risk groups to undergo at least one examination every six months.
(2) Dynamic enhanced CT and multiparametric MRI scanning are the preferred imaging examination methods for confirming the diagnosis of liver cancer in patients with abnormal liver ultrasound and/or serum AFP screening.
(3) The imaging diagnosis of liver cancer is mainly based on the “fast in and fast out” enhancement pattern.
(4) Multiparametric MRI examination is the preferred imaging technique for clinical diagnosis, staging, and efficacy evaluation of liver cancer.
(5) PET-CT scanning helps in the staging and efficacy evaluation of liver cancer.
(6) Serum AFP is a commonly used and important indicator for diagnosing liver cancer and monitoring efficacy. For AFP-negative populations, early diagnosis can be aided by PIVKAⅡ, miRNA detection kits, AFP-L3, and GALAD-like models.
(7) Patients with liver space-occupying lesions exhibiting typical imaging characteristics of liver cancer and meeting clinical diagnostic criteria usually do not require liver lesion biopsy for diagnostic purposes.
(5) Pathological Diagnosis of Liver Cancer.
1. Terminology for Pathological Diagnosis of Liver Cancer.
Primary liver cancer refers to malignant tumors originating from hepatocytes and intrahepatic bile duct epithelial cells, mainly including HCC, ICC, and cHCC-CCA.
(1) HCC: refers to malignant tumors occurring in hepatocytes. The pathological diagnostic names “hepatocellular carcinoma” or “hepatocellular carcinoma” are not recommended.
(2) ICC: refers to malignant tumors arising from the epithelial cells lining the intrahepatic bile duct branches, with adenocarcinoma being the most common.
Histologically, it can be divided into:
① Bold duct type: originating from larger bile ducts above the interlobular bile ducts to the adjacent hepatic portal area, with large and irregular ductal diameters;
② Small duct type: originating from smaller bile ducts or fine ducts below the interlobular bile ducts, with smaller and more regular ductal diameters, or may present as solid strands with closed lumens.
Studies have shown that the biological behavior and genetic phenotype characteristics of the above two subtypes of ICC also differ, with patients with small duct type having better clinical prognosis than those with bold duct type.
Regarding the clinical and pathological significance of molecular typing of HCC and ICC, many are still in research and demonstration stages, but recent studies indicate that EB virus-associated ICC has unique clinical, pathological, immune microenvironment, and molecular characteristics, with better prognosis and benefits from immune checkpoint therapy, which is expected to become a new subtype; while high expression of phosphofructokinase 1 in ICC tissues is a useful indicator for assessing postoperative recurrence risk, etc. The 2019 edition of the WHO classification of digestive system tumors no longer recommends using the pathological diagnostic name “cholangiocellular carcinoma” for ICC.
The gross sampling and microscopic examination requirements for ICC mainly refer to those for HCC.
(3) cHCC-CCA: refers to tumors that simultaneously exhibit both HCC and ICC components within the same tumor nodule, excluding collision tumors. Although some scholars suggest using a pathological diagnostic standard for cHCC-CCA based on the proportion of the two tumor components being ≥30%, there is currently no internationally unified pathological diagnostic standard for the proportion of the two tumor components in cHCC-CCA. Therefore, it is recommended to annotate the proportion of the two tumor components when diagnosing cHCC-CCA pathologically, for clinical evaluation of tumor biological characteristics and development of treatment plans.
2. Standards for Pathological Diagnosis of Liver Cancer.
The standards for pathological diagnosis of liver cancer consist of specimen handling, specimen sampling, pathological examination, and pathological reporting.
(1) Key points of specimen handling:
① The surgical physician should clearly indicate the site, type, and quantity of the specimen on the pathological examination application form. Important lesions can be marked with dye or sutures;
② Tumor specimens should be sent to the pathology department for cutting and fixation within 30 minutes of being excised. When retaining specimens for tissue banks, it should be done under the guidance of the pathology department to ensure accurate sampling and should primarily meet the needs of pathological diagnosis;
③ Fixation is done in 4% neutral formaldehyde (10% neutral buffered formalin) solution for 12-24 hours.
(2) Key points of specimen sampling:
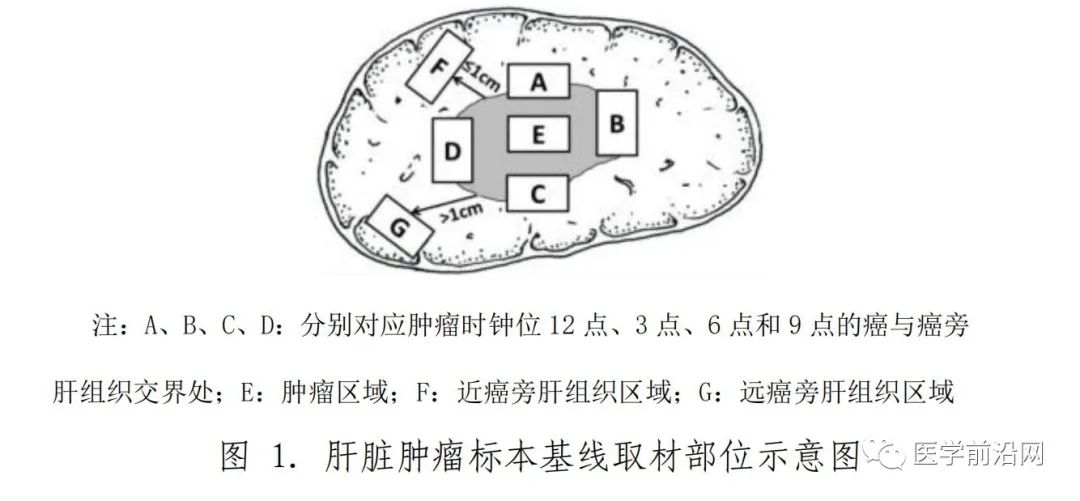
The area surrounding the liver cancer is representative of the tumor’s biological behavior. Therefore, a 7-point baseline sampling method is required (Figure 1), sampling at the 12 o’clock, 3 o’clock, 6 o’clock, and 9 o’clock positions at the interface between cancer and adjacent liver tissue at a 1:1 ratio; at least one block should be sampled from within the tumor; one block should be sampled from liver tissue within ≤1 cm (near cancer) and >1 cm (far from cancer) ranges. For a single tumor with a maximum diameter of ≤3 cm, all should be sampled for examination. The actual sampling site and quantity should also consider factors such as tumor size and number (evidence level 3, recommendation A).
3. Key Points of Pathological Examination for Liver Cancer.
(1) Gross specimen observation and description: A comprehensive observation of all surgical specimens sent for examination should be conducted, focusing on describing the tumor’s size, number, color, texture, relationship with blood vessels and bile ducts, capsule condition, surrounding liver tissue lesions, type of liver cirrhosis, distance from the tumor to the cut margin, and the condition of the cut margin.
(2) Microscopic observation and description: A comprehensive observation of all sampled tissues should be conducted. The pathological diagnosis of liver cancer can refer to the 2019 edition of the WHO classification of digestive system tumors, focusing on describing the following: the degree of differentiation of liver cancer: the commonly used Edmondson-Steiner four-grade (I-IV) grading method or WHO recommended high, medium, and low differentiation. Histological morphology of liver cancer: common types include trabecular type, large trabecular type, pseudo-glandular type, and sheet-like type; special subtypes of liver cancer: such as fibrolamellar type, sclerosing type, clear cell type, fatty type, giant trabecular type, chromophobic type, neutrophilic type, lymphocytic type, and undifferentiated type; tumor necrosis (e.g., after transarterial chemoembolization treatment), the extent and degree of lymphocytic infiltration and interstitial fibrosis; growth patterns of liver cancer: including peritumoral infiltration, capsule invasion or breakthrough, MVI, and satellite nodules; chronic liver disease assessment: liver cancer often accompanies varying degrees of chronic viral hepatitis or liver cirrhosis, and the simplified Scheuer scoring system and Chinese chronic viral hepatitis histological grading and staging standards are recommended.
(3) Diagnosis of MVI: MVI refers to the presence of cancer cell nests in blood vessels lined by endothelial cells observed microscopically, with portal vein branch invasion (including intramural vascular invasion) being the most common in liver cancer, while lymphatic invasion may occur in ICC. The pathological grading method is as follows: M0: no MVI found; M1 (low-risk group): ≤5 MVI, all occurring in adjacent liver tissue (≤1 cm); M2 (high-risk group): >5 MVI, or MVI occurring in distant liver tissue (>1 cm). MVI and satellite lesions can be seen as different evolutionary stages of intrahepatic metastasis of liver cancer. When it is difficult to distinguish between satellite nodules or lesions in adjacent liver tissue and MVI, they can be counted together in the pathological grading of MVI. MVI is an important reference for assessing the risk of liver cancer recurrence and selecting treatment plans and should be included as an indicator in routine histopathological examinations (evidence level 2, recommendation A).
4. Immunohistochemical Examination.
The main purposes of liver cancer immunohistochemical examination are:
① Differentiating between benign and malignant liver cell tumors;
② Differentiating between HCC and ICC as well as other special types of liver tumors;
③ Differentiating between primary liver cancer and metastatic liver cancer.
Due to the high heterogeneity of liver cancer histological types, existing liver cancer cell protein markers have certain limitations in specificity and sensitivity for diagnosis, often requiring reasonable combinations and objective assessments, and sometimes needing to be used in conjunction with markers from other systemic tumors.
(1) HCC:
The following markers are positive for hepatocyte markers, which help indicate tumors of hepatic origin, but cannot serve as the basis for distinguishing between benign and malignant liver tumors.
① Arginase-1: cytoplasmic/nuclear staining of hepatocytes.
② Hepatocyte antigen: cytoplasmic staining of hepatocytes.
③ Antibodies specific for bile canaliculi on hepatocyte membranes: such as CD10, polyclonal carcinoembryonic antigen, and bile salt export pump protein, which can show specific staining on the canalicular surface of hepatocyte membranes, helping to confirm hepatocellular tumors.
The following markers help differentiate between benign and malignant liver cell tumors.
① Phosphatidylinositol protein-3: cytoplasmic and cell membrane staining of hepatocellular carcinoma.
② CD34: Although CD34 immunohistochemical staining does not directly mark liver parenchymal cells, it can display the microvascular density and distribution patterns of different types of liver tumors: hepatocellular carcinoma shows a diffuse pattern, cholangiocarcinoma shows a sparse pattern, hepatocellular adenoma shows a patchy pattern, and focal nodular hyperplasia shows a cord-like pattern, which, combined with tumor histological morphology, helps in differential diagnosis.
③ Heat shock protein 70: cytoplasmic or nuclear staining of hepatocellular carcinoma cells.
④ Glutamine synthetase: often shows diffuse strong positivity in hepatocellular carcinoma; some hepatocellular adenomas, especially β-catenin mutation-activated hepatocellular adenomas, may also exhibit diffuse positivity; in HGDN, moderate focal staining is observed, with positive cell counts <50%; in focal nodular hyperplasia, characteristic irregular map-like staining is observed; in normal liver tissue, only hepatocytes around central veins are stained, which helps in differential diagnosis.
(2) ICC:
① Mucins (MOC31): membrane staining of cholangiocarcinoma cells.
② Cytokeratin (CK) 7/CK19: cytoplasmic staining of cholangiocarcinoma cells.
③ Mucins-1 (muc-1): membrane staining of cholangiocarcinoma cells.
Although the positivity of the above markers can suggest tumors of biliary epithelial origin, they can also express positivity in non-tumorous biliary epithelium, necessitating careful differentiation.
(3) cHCC-CCA:
Both HCC and ICC components express their respective tumor markers. In addition, positive expression of markers such as CD56, CD117, and epithelial cell adhesion molecule (EpCAM) may suggest tumor features associated with stem cell differentiation and stronger invasiveness.
5. Pathological Assessment of Liver Cancer Specimens after Conversion/New Adjuvant Therapy.
(1) Specimen Sampling.
For liver cancer resection specimens marked for conversion/new adjuvant therapy preoperatively, the following processing procedures can be followed: at the maximum diameter of the tumor bed (the original location of the tumor before treatment), cut and measure the three-dimensional dimensions. For small liver cancers with a maximum diameter of ≤3 cm, all should be sampled; for tumors >3 cm, the tumor should be cut at intervals of 0.5-1 cm at the maximum diameter, selecting the most representative sections of tumor necrosis and residual tissue for sampling, ensuring that tumor bed and surrounding liver tissue are also retained for comparison, and photographs of the gross specimens can be taken for histological observation comparison.
(2) Microscopic Assessment.
The assessment mainly involves evaluating the proportions of three components in the tumor bed of liver cancer resection specimens:
① Necrotic tumor;
② Viable tumor;
③ Tumor stroma (fibrous tissue and inflammation).
The sum of these three areas in the tumor bed equals 100%. The number of samples taken should be indicated in the pathological report, and the average percentage of the three components should be calculated based on the assessment of each slice to determine the total percentage of residual tumor.
(3) Evaluation of Complete Pathological Response and Major Pathological Response: These are important pathological indicators for evaluating the efficacy of preoperative treatment and exploring the best timing for surgery.
Complete pathological response (CPR) refers to the absence of viable tumor cells in the histological assessment of tumor bed specimens after preoperative treatment.
Major pathological response (MPR) refers to the reduction of viable tumor cells to below the threshold that can affect clinical prognosis after preoperative treatment. In lung cancer research, MPR is often defined as the reduction of residual tumor cells in the tumor bed to ≤10%, which also correlates with the degree of tumor necrosis and prognosis in liver cancer after TACE treatment. The specific threshold for MPR needs further clinical research confirmation. It is recommended to further expand the sampling range for tumor specimens initially diagnosed as MPR.
(4) Histological Assessment Method for the Degree of Necrosis in Liver Cancer Specimens after Treatment with Immune Checkpoint Inhibitors can refer to some tumor types that have undergone related research, deepening understanding of histological characteristics of liver cancer while observing for any immune-related liver injury in the surrounding liver tissue, including hepatocyte damage, lobular hepatitis, and cholangitis.
6. Pathological Diagnosis Report for Liver Cancer.
The report mainly consists of gross specimen description, microscopic description, immunohistochemical examination, and pathological diagnosis name, and can also provide explanations and recommendations to clinicians if necessary (Appendix 4). In addition, it may include molecular pathological examination results related to the clonal origin detection of liver cancer, drug target detection, biological behavior assessment, and prognosis judgment for clinical reference.
Key Points Overview
(1) Standardized handling and timely submission of liver cancer resection specimens are crucial for preserving tissue and cell integrity and accurate pathological diagnosis.
(2) The sampling of liver cancer specimens should follow the standardized “seven-point baseline sampling” method, which is conducive to obtaining representative pathological biological characteristic information of liver cancer.
(3) The content of the pathological diagnosis report for liver cancer should be standardized and comprehensive, with particular attention to the diagnosis and pathological grading assessment of MVI, an important factor affecting the prognosis of liver cancer.
(6) Clinical Diagnosis Standards and Roadmap for Liver Cancer.
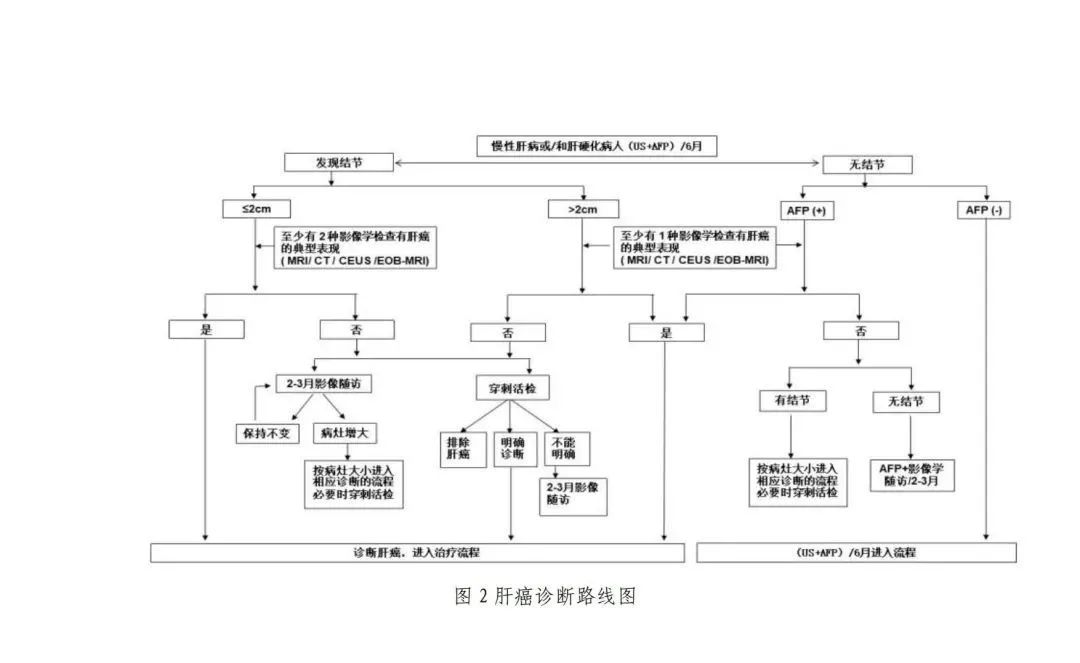
Combining high-risk factors for liver cancer, imaging characteristics, and serological molecular markers, clinical diagnosis of liver cancer can be based on the steps of the roadmap (Figure 2).
1. For individuals with HBV or HCV infection, or any cause of liver cirrhosis, ultrasound examinations and serum AFP tests should be performed at least every 6 months. If liver nodules with a diameter ≤2 cm are found, at least 2 of the four imaging examinations (multiparametric MRI, dynamic enhancement CT, contrast-enhanced ultrasound, or hepatocyte-specific contrast agent Gd-EOB-DTPA enhanced MRI) show significant enhancement in the arterial phase and lower enhancement in the portal and/or delayed phase compared to liver parenchyma, indicating the typical features of liver cancer, a clinical diagnosis of liver cancer can be made; for liver nodules with a diameter >2 cm, a clinical diagnosis of liver cancer can be made as long as one of the four imaging examinations shows typical liver cancer features.
2. For individuals with HBV or HCV infection, or any cause of liver cirrhosis, if liver nodules with a diameter ≤2 cm are found during follow-up and only 1 or none of the four imaging examinations show typical liver cancer features, liver lesion biopsy or imaging follow-up every 2-3 months combined with serum AFP levels should be conducted for definitive diagnosis; for liver nodules with a diameter >2 cm, if none of the four imaging examinations show typical liver cancer features, liver lesion biopsy or imaging follow-up every 2-3 months combined with serum AFP levels should also be conducted for definitive diagnosis.
3. For individuals with HBV or HCV infection, or any cause of liver cirrhosis, if serum AFP levels are elevated, especially persistently elevated, imaging examinations should be performed to confirm the diagnosis of liver cancer; if any of the four imaging examinations show typical liver cancer features, a clinical diagnosis of liver cancer can be made; if no liver nodules are found, serum AFP changes should be closely monitored, and imaging re-examinations should be conducted every 2-3 months while excluding pregnancy, chronic or active liver disease, germ cell tumors, and gastrointestinal tumors.
Staging
Staging of liver cancer is crucial for selecting treatment plans and assessing prognosis. Various staging systems exist abroad, such as BCLC, TNM, JSH, and APASL. Based on China’s specific national conditions and practical experience, a staging system for liver cancer in China (China liver cancer staging, CNLC) has been established, including: CNLC stage I a, I b, II a, II b, III a, III b, and IV, with specific staging descriptions provided in Figure 3.
CNLC stage I a:
PS 0-2 points, liver function Child-Pugh A/B grade, single tumor with a diameter ≤5 cm, no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC stage I b:
PS 0-2 points, liver function Child-Pugh A/B grade, single tumor with a diameter >5 cm, or 2-3 tumors with a maximum diameter ≤3 cm, no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC stage II a:
PS 0-2 points, liver function Child-Pugh A/B grade, 2-3 tumors with a maximum diameter >3 cm, no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC stage II b:
PS 0-2 points, liver function Child-Pugh A/B grade, ≥4 tumors, regardless of tumor size, no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC stage III a:
PS 0-2 points, liver function Child-Pugh A/B grade, regardless of tumor situation, with radiologically visible vascular cancer thrombus but no extrahepatic metastasis;
CNLC stage III b:
PS 0-2 points, liver function Child-Pugh A/B grade, regardless of tumor situation, with or without radiologically visible vascular cancer thrombus and extrahepatic metastasis;
CNLC stage IV:
PS 3-4 points, or liver function Child-Pugh C grade, regardless of tumor situation, with or without radiologically visible vascular cancer thrombus and extrahepatic metastasis.
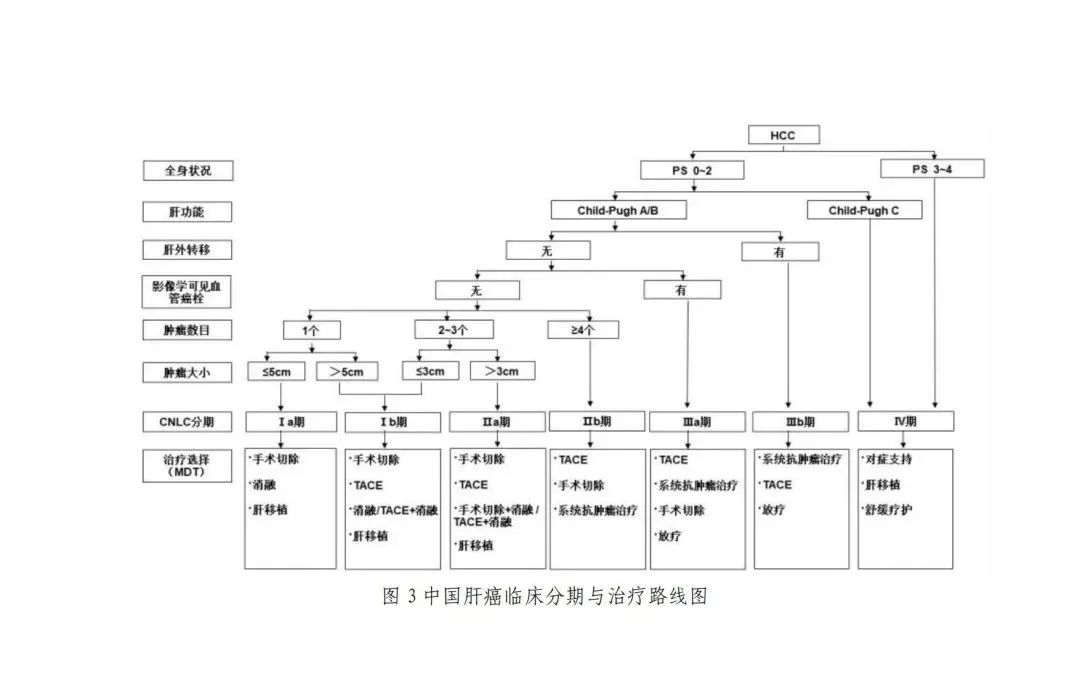
Note: Systemic anti-tumor treatment includes: first-line treatment: Atezolizumab + Bevacizumab, Sintilimab + Bevacizumab similar (Dabrafenib); Donafenib, Lenvatinib, Sorafenib; FOLFOX4 second-line treatment: Regorafenib, Apatinib, Carrelizumab, Tislelizumab
06Treatment
The treatment of liver cancer is characterized by multidisciplinary involvement and coexistence of various treatment methods. Common treatment methods include liver resection, liver transplantation, ablation therapy, TACE, radiotherapy, and systemic anti-tumor therapy. Choosing appropriate treatment methods for patients with different stages of liver cancer can maximize efficacy. The choice of reasonable treatment methods requires support from high-level evidence-based medical evidence. Currently, the long-term efficacy of standardized combined therapies for liver cancer is best, but there are certain contradictions between the existing specialized treatment system based on different treatment methods and the realization of standardized combined therapies. Therefore, the diagnosis and treatment of liver cancer must emphasize the multidisciplinary team (MDT) treatment model, especially for the treatment of difficult and complex cases, to avoid the limitations of single-specialty treatment, promote interdisciplinary communication, and improve overall efficacy. It is recommended that the management of liver cancer MDT should focus on the core indicators of quality control in liver cancer diagnosis and treatment established by the National Health Commission, but it should also consider the differences in regional economic levels and the medical capabilities and conditions of each hospital.
(1) Surgical Treatment.
Surgical treatment of liver cancer is an important means for liver cancer patients to achieve long-term survival, mainly including liver resection and liver transplantation.
1. Basic Principles of Liver Resection.
(1) Completeness: complete resection of the tumor with no residual tumor at the cut margin;
(2) Safety: retaining enough volume and functional liver tissue (with good blood supply and good blood and bile reflux) to ensure postoperative liver function compensation, reduce surgical complications, and lower mortality.
2. Preoperative Evaluation of Patients’ Overall Condition and Liver Reserve Function.
Before surgery, a comprehensive evaluation of the patient’s overall condition, liver reserve function, and liver tumor status (staging and location) should be conducted. The functional status score proposed by the Eastern Cooperative Oncology Group (ECOG PS) is commonly used to evaluate the patient’s overall condition; the Child-Pugh score for liver function, indocyanine green (ICG) clearance test, or transient elastography to assess liver stiffness are used to evaluate liver reserve function. Research results indicate that selected liver cancer patients with portal hypertension can still undergo liver resection, and their postoperative long-term survival is better than that of patients receiving other treatments. Therefore, more accurate evaluation of the degree of portal hypertension (such as measuring the hepatic venous pressure gradient) is helpful in selecting patients suitable for surgical resection. If the expected volume of remaining liver tissue is small, CT, MRI, or three-dimensional reconstruction of the liver can be used to measure the volume of the remaining liver and calculate the percentage of remaining liver volume relative to the standardized liver volume. Generally, it is considered necessary to have liver function Child-Pugh A grade and ICG 15-minute retention rate (ICG-R15) <30% as necessary conditions for surgical resection; the remaining liver volume must account for more than 40% of the standardized liver volume (in cases with chronic liver disease, liver parenchyma damage, or cirrhosis) or more than 30% (in cases without liver fibrosis or cirrhosis), which are also necessary conditions for surgical resection. In cases of liver function impairment, more remaining liver volume should be preserved.
3. Indications for Liver Resection.
(1) The preferred treatment method for liver cancer in CNLC stage I a, I b, and II a patients with good liver reserve function is surgical resection. Previous research results show that for liver cancers ≤3 cm in diameter, there is no significant difference in efficacy between surgical resection and radiofrequency ablation treatment (evidence level 1, recommendation B), but recent studies indicate that the local recurrence rate after surgical resection is significantly lower than that after radiofrequency ablation, and the long-term efficacy of surgical resection is better (evidence level 1, recommendation A). Even for recurrent liver cancer, the prognosis of surgical resection is still better than that of radiofrequency ablation (evidence level 2, recommendation B).
(2) For patients with CNLC stage II b liver cancer, surgical resection is usually not the first choice, and non-surgical treatment based on TACE is preferred. If the tumor is limited to the same segment or the same side of the liver, or if intraoperative ablation can be performed on lesions outside the resection range, even if the number of tumors is >3, surgical resection may achieve better results than other treatments, hence surgical resection is also recommended (evidence level 2, recommendation B), but a more cautious preoperative multidisciplinary evaluation is required.
(3) For patients with CNLC stage III a liver cancer, the vast majority are not suitable for surgical resection, and non-surgical treatment based on systemic anti-tumor treatment is the preferred option.
However, if the following conditions are met, surgical resection may also be considered:
① Patients with portal vein branch cancer thrombus (Cheng classification type I/II) (Appendix 5), if the tumor is limited to half of the liver or the same side of the liver, surgical resection of the tumor and portal vein thrombectomy can be considered, followed by TACE treatment, portal vein chemotherapy, or other systemic anti-tumor treatments; patients with main portal vein cancer thrombus (Cheng classification type III) have a high short-term recurrence rate after surgery, and most patients’ postoperative survival is not ideal, hence it is not an absolute indication for surgical resection (evidence level 3, recommendation B). For liver cancer patients who can be resected with portal vein cancer thrombus, preoperative three-dimensional conformal radiotherapy can improve postoperative survival (evidence level 2, recommendation C).
② Patients with cancer thrombus in the bile duct but liver lesions that can also be resected. ③ Patients with partial hepatic vein involvement but liver lesions that can be resected.
(4) For patients with lymph node metastases at the hepatic hilum (CNLC stage III b), surgical resection of the tumor with simultaneous hepatic hilum lymphadenectomy or postoperative external radiotherapy can be considered. If surrounding organs can be resected, surgical resection may also be considered. Additionally, for liver cancer found unsuitable for surgical resection during intraoperative exploration, intraoperative arterial and portal vein catheterization chemotherapy or other local treatment measures may be considered, or subsequent TACE treatment, systemic anti-tumor treatment, etc., may be conducted after the surgical trauma has healed.
4. Standards for Radical Resection of Liver Cancer.
(1) Intraoperative judgment criteria:
① No visible cancer thrombus in hepatic veins, portal veins, bile ducts, or inferior vena cava;
② No invasion of adjacent organs, no lymph node metastases at the hepatic hilum, or distant metastases;
③ The distance from the liver cut margin to the tumor boundary is ≥1 cm; if the margin is <1 cm, histological examination of the resection surface must show no residual tumor cells, indicating a negative margin.
(2) Postoperative judgment criteria:
① Ultrasound, CT, or MRI examination (at least two of these must be performed) should be conducted 1-2 months after surgery to check for tumor lesions;
② If preoperative serum AFP, DCP, and other serum tumor markers were elevated, the serum tumor markers should be quantitatively measured two months after surgery, and their levels should fall within the normal range. The rate of decline in serum tumor markers after surgery can predict the completeness of the surgical resection early.
5. Surgical Techniques for Resection.
The commonly used surgical techniques for liver resection mainly include blood flow control techniques for entering and exiting the liver, liver dissection techniques, and hemostatic techniques. Preoperative three-dimensional visualization technology for individualized liver volume calculation and virtual liver resection can help design a more precise resection range and path to protect the remaining liver while achieving the goal of radical resection of the tumor (evidence level 2, recommendation A).
In recent years, laparoscopic liver surgery has rapidly developed. Laparoscopic liver resection has advantages of less trauma and faster postoperative recovery, and its oncological effect is comparable to open liver resection in selected patients (evidence level 3, recommendation C). Although the indications and contraindications for laparoscopic liver resection are generally similar to those for open surgery, it is still recommended to conduct a comprehensive assessment based on tumor size, location, number, underlying liver diseases, and the technical level of the surgical team. For large liver cancers, multiple liver cancers, liver cancers located in difficult positions, and central liver cancers adjacent to important vessels, it is recommended that this treatment be performed by experienced physicians after strict selection. Utilizing laparoscopic ultrasound combined with indocyanine green fluorescence tumor imaging can help detect small lesions and mark resection ranges to obtain negative tumor margins.
Both anatomical and non-anatomical resections are commonly used liver resection techniques, both requiring adequate margins to achieve good oncological outcomes. Anatomical resection for liver cancer cases with MVI, compared to non-anatomical resection, shows no difference in overall survival, but has a lower local recurrence rate (evidence level 3, recommendation B). Studies have found that wide margins (≥1 cm margins) in liver resection are superior to narrow margins (evidence level 1, recommendation A), especially for patients with predictable MVI before surgery. For giant liver cancers, the anterior approach for liver resection is recommended. For multiple liver cancers, surgical resection combined with intraoperative ablation treatment is recommended (evidence level 4, recommendation C). For patients with portal vein cancer thrombus, portal vein thrombectomy should temporarily block blood flow from the healthy side of the portal vein to prevent cancer thrombus dissemination. For patients with hepatic vein cancer thrombus or inferior vena cava cancer thrombus, total hepatic blood flow blockage can be performed to remove cancer thrombus as completely as possible. For liver cancers with bile duct cancer thrombus, simultaneous resection of liver tumors and bile duct is recommended to strive for radical resection opportunities (evidence level 3, recommendation C).
For liver cancers found to be severe cirrhosis, deep tumors, or multiple nodules after abdominal exploration, consideration can be given to performing only intraoperative ablation treatment to reduce surgical risks.
6. Comprehensive Treatment Strategy Focused on Surgery.
Based on previous large-scale case data, the overall survival of patients with advanced liver cancer (CNLC II b, III a, III b stages) after surgery is not satisfactory, but in the absence of other effective treatment methods, surgical resection can still benefit some patients (evidence level 4, recommendation C). Current systemic anti-tumor treatment and comprehensive treatment have made significant progress, and the effects of systemic anti-tumor treatment and/or local treatment in controlling tumors can provide more possibilities for radical resection, reducing postoperative recurrence, and improving prognosis (evidence level 4, recommendation B). Therefore, the strategy of direct surgical resection for patients with advanced liver cancer needs to be re-evaluated. Exploring new strategies for comprehensive treatment of advanced liver cancer focused on surgery has become a recent focus of attention.
(1) Conversion Treatment for Potentially Resectable Liver Cancer.
Conversion treatment aims to convert unresectable liver cancer into resectable liver cancer and is one of the pathways for patients with advanced liver cancer to achieve radical resection and long-term survival. For potentially resectable liver cancer, it is recommended to adopt a multimodal, high-intensity anti-tumor treatment strategy to promote conversion while ensuring the safety and quality of life of the treatment.
1) Conversion Treatment Targeting Tumors
① Systemic Anti-Tumor Treatment: The standalone or combined application of systemic anti-tumor treatment is one of the main methods for conversion treatment of advanced liver cancer (evidence level 4, recommendation B). The depth, speed, and duration of liver cancer remission, as well as organ-specific remission, are important factors affecting subsequent treatment decisions. More exploration is needed regarding the effects of different drug combinations on liver tissue and the safety of subsequent surgery.
② Local Treatment: Including TACE [120] (evidence level 3, recommendation B), hepatic arterial infusion chemotherapy (HAIC) (evidence level 4, recommendation C) and other local treatment methods create potential surgical resection opportunities for initially unresectable liver cancer patients and can translate into survival benefits. Combined radiotherapy with HAIC, HAIC combined with TACE [123] can further improve conversion rates. The combination of systemic anti-tumor treatment and local treatment is expected to achieve higher tumor remission and higher conversion resection rates (evidence level 4, recommendation B).
2) Conversion Treatment Targeting Insufficient Remaining Liver Volume:
① Portal vein embolization (PVE) of the affected half of the liver can induce compensatory hyperplasia of the remaining liver before tumor resection. The success rate of PVE is 60%-80%, with a complication rate of about 10%-20%. The time for hyperplasia of the remaining liver after PVE is relatively long (usually 4-6 weeks), and more than 20% of patients may lose the opportunity for surgery due to tumor progression or insufficient volume of remaining liver (evidence level 3, recommendation B).
② Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is suitable for patients expected to have remaining liver volume less than 30%-40% of the standardized liver volume. In recent years, various improved surgical techniques for ALPPS have emerged, mainly focusing on the first-stage surgical liver sectioning (partial sectioning and using radiofrequency ablation, microwave, hemostatic techniques) and employing laparoscopic minimally invasive approaches for ALPPS. Preoperative assessment is very important and should comprehensively consider the degree of liver cirrhosis, patient age, and short-term ability to withstand two surgeries. ALPPS can enhance the resection rate of liver cancer in a short time, with a rapid ability to induce hyperplasia of the remaining liver, superior to PVE (evidence level 2, recommendation A); due to the short interval between the two surgeries, it can minimize the risk of tumor progression, achieving a tumor resection rate of 95%-100%. Research results indicate that ALPPS treatment for giant or multiple liver cancers shows better results than TACE (evidence level 3, recommendation B). Careful and reasonable selection of surgical candidates by experienced surgeons is recommended for ALPPS surgery, especially for elderly liver cancer patients.
3) Neoadjuvant Treatment.
According to the definition by the National Cancer Institute, neoadjuvant treatment is treatment to shrink tumors before the main treatment (usually surgical resection). Common neoadjuvant treatments include systemic anti-tumor treatment, interventional treatment, radiotherapy, etc., aiming to reduce postoperative recurrence and prolong postoperative survival. For resectable advanced liver cancer (CNLC II b, III a stages), neoadjuvant treatment can convert liver cancer with poor oncological characteristics into liver cancer with better oncological characteristics, thereby reducing postoperative recurrence and prolonging survival. For liver cancer with portal vein cancer thrombus that can be surgically resected, preoperative three-dimensional conformal radiotherapy can improve efficacy (evidence level 2, recommendation C). However, for liver cancer that can be surgically resected, preoperative TACE does not prolong patient survival (evidence level 2, recommendation A). Strategies using immune therapy combined with targeted drugs, or single-agent or combination immunotherapy for preoperative or perioperative treatment of resectable liver cancer are expected to further improve surgical efficacy (evidence level 2, recommendation B). However, for earlier stages of liver cancer (CNLC I a, I b, II a stages), whether preoperative treatment can improve patient survival and reduce recurrence still requires clinical research confirmation.
(3) Adjuvant Treatment.
The recurrence and metastasis rate of tumors after liver cancer resection can be as high as 40%-70%, which is related to the possible presence of micro-disseminated lesions or multicentric occurrences before surgery. Therefore, all patients require close follow-up after surgery. For patients at high risk of recurrence, two randomized controlled studies have confirmed that postoperative TACE treatment can reduce recurrence and prolong survival (evidence level 1, recommendation A). Another randomized controlled study showed that treatment with Huai’er granules after liver resection can reduce recurrence and prolong patient survival (evidence level 2, recommendation A). For liver cancer patients infected with HBV, antiviral treatment with nucleoside analogs not only controls the underlying liver disease but also helps reduce postoperative tumor recurrence (evidence level 1, recommendation A). For liver cancer patients infected with HCV, direct-acting antiviral agents (DAAs) can achieve sustained virological response, and currently, there is no conclusive data indicating that DAA treatment is related to increased or decreased risk of postoperative tumor recurrence, differences in recurrence time, or aggressiveness of recurrent liver cancer (evidence level 3, recommendation C). In addition, for patients with portal vein cancer thrombus, postoperative catheterization chemotherapy combined with TACE can also prolong patient survival (evidence level 2, recommendation A). Although some clinical randomized studies suggest that α-interferon can reduce recurrence and prolong survival (evidence level 1, recommendation B), there is still controversy. Reports have indicated that the expression of miR-26a in liver cancer is related to the efficacy of α-interferon treatment, and this result requires further validation through multi-center randomized controlled trials. The exploration of strategies using immunotherapy, targeted drugs, and HAIC alone or in combination after recurrence is actively underway. Once tumor recurrence is detected, based on the characteristics of the recurrent tumor, options such as re-surgical resection, ablation therapy, interventional treatment, radiotherapy, or systemic anti-tumor treatment can be selected to prolong patient survival.
Key Points Discussion
(1) Liver resection is an important means for liver cancer patients to achieve long-term survival.
(2) The principle of liver resection is to completely remove the tumor while preserving adequate volume and functional liver tissue; thus, comprehensive preoperative evaluation of liver reserve function and oncological assessment is very important.
(3) It is generally considered that liver function Child-Pugh A grade and ICG-R15 <30% are necessary conditions for surgical resection; the remaining liver volume must account for more than 40% of the standardized liver volume (for those with chronic liver disease, liver parenchyma damage, or cirrhosis) or more than 30% (for those without liver fibrosis or cirrhosis), which are also necessary conditions for surgical resection. Patients with liver function impairment should preserve more remaining liver volume.
(4) The preferred treatment for liver cancer in CNLC stage I a, I b, and II a patients with good liver reserve function is surgical resection.
(5) The principles of surgical resection include thoroughness and safety, ensuring adequate margins during resection to achieve good oncological outcomes.
(6) For potentially resectable liver cancer, multimodal, high-intensity treatment strategies are recommended to promote conversion.
(7) Postoperative adjuvant treatment aims to reduce recurrence.
(8) Systemic anti-tumor treatment, local treatment, and supportive care should be integrated into the treatment plan.
(9) The treatment of spontaneous rupture of liver cancer requires individualized treatment plans based on comprehensive assessments of hemodynamics, liver function, and tumor resectability.
(10) The preparation of this guideline is independent of any sponsors, and all authors have committed that the content of the writing is unrelated to funding.