Guo Rinnan, Tang Wen, Liu Yan
Intensive Care Unit, Xinjiang Uygur Autonomous Region People’s Hospital, Urumqi 830001
International Journal of Anesthesiology and Resuscitation, 2024, 45(12): 1263-1269.
DOI: 10.3760/cma.j.cn321761-20240625‑01168
ORIGINAL ARTICLES
Currently, there are few studies on myocardial injury associated with sepsis after surgery (SIMD) in surgical patients with sepsis. This study aims to evaluate and integrate the risk factors for SIMD occurring after surgery in sepsis patients and to construct a personalized prediction model, which will help in the early identification of high-risk groups for SIMD and provide a theoretical basis for clinical decision-making.

1 Data and Methods

A retrospective analysis was performed on 128 patients who were diagnosed with sepsis and transferred to the intensive care unit after surgical drainage at Xinjiang Uygur Autonomous Region People’s Hospital from January to December 2021. Patient general data and laboratory indicators were collected. Based on whether SIMD occurred during the treatment, the subjects were divided into the myocardial injury group (47 cases) and the control group (81 cases). Inclusion criteria: ① Sepsis diagnosis conforms to the latest definition and diagnostic criteria of Sepsis 3.0; ② Clear infection focus with surgical intervention or drainage; ③ Age ≥ 18 years; ④ Duration of intensive care unit (ICU) treatment ≥ 24 hours. Exclusion criteria: ① History of acute myocardial infarction, coronary heart disease, cardiomyopathy, valvular heart disease, congenital heart disease, etc.; ② Underwent cardiopulmonary resuscitation, defibrillation, and cardioversion; ③ Pulmonary embolism, chronic anemia, trauma, burns; ④ Associated with autoimmune diseases, malignant tumors; ⑤ Pregnancy or lactation.
Multivariate logistic regression analysis was used to determine the independent risk factors for SIMD occurring after surgery in sepsis patients. Based on this, a nomogram prediction model was constructed, and the clinical applicability of the nomogram prediction model was analyzed and internally validated.
2 Results
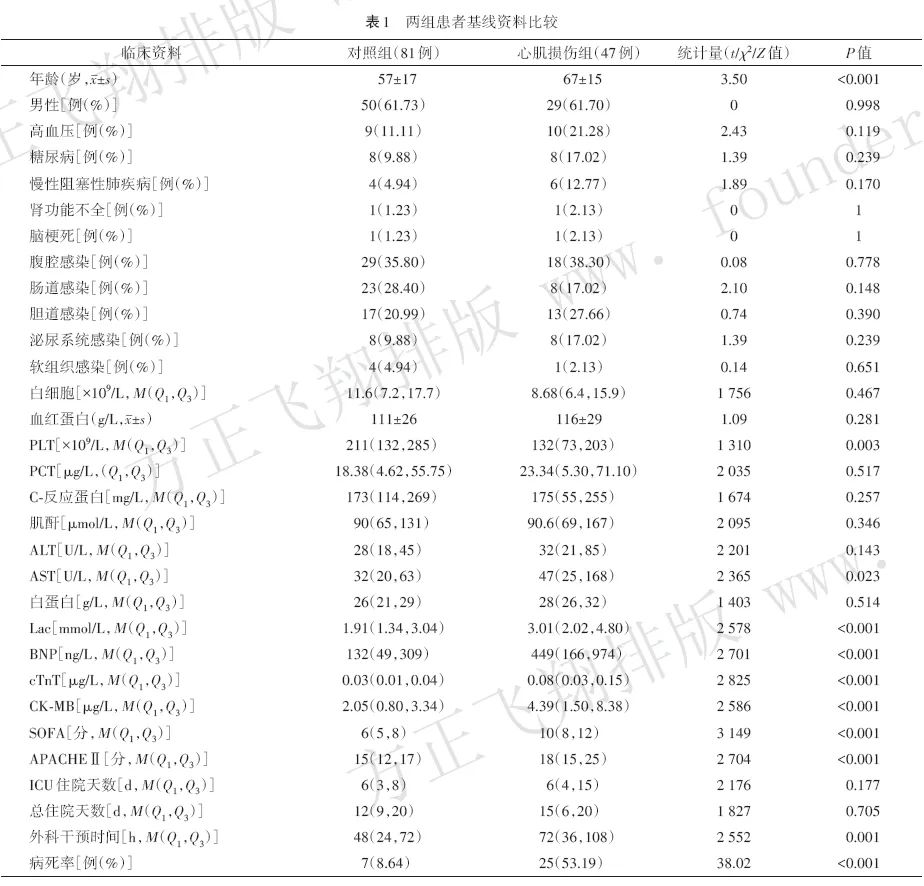
2.1 Comparison of Clinical Data Between the Two Groups
Among the 128 patients, 47 (36.7%) had concurrent myocardial injury. The myocardial injury group had higher age, PLT, AST, Lac, BNP, cTnT, CK-MB, SOFA, APACHE II, and mortality rates compared to the control group (all P < 0.05), and the duration of surgical intervention was longer than that of the control group (P < 0.05). See Table 1.
2.2 Logistic Regression Analysis of Risk of SIMD Occurrence
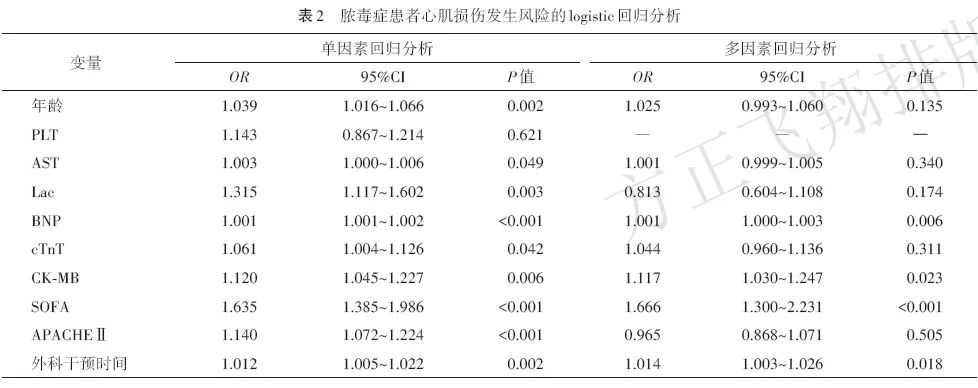
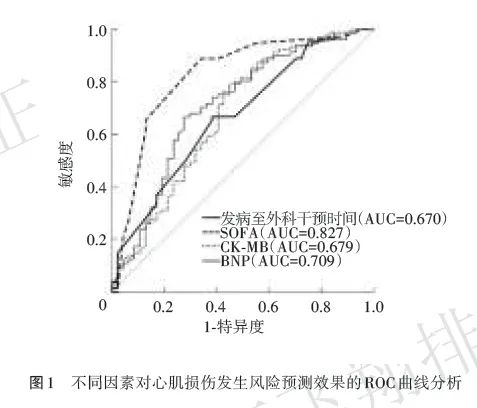
The statistically significant variables from the above results were used as independent variables, with the occurrence of myocardial injury as the dependent variable for univariate logistic regression analysis. The results showed that the difference in PLT was not statistically significant, thus this variable was excluded. The remaining variables were included in the multivariate logistic regression model, which showed that BNP, CK-MB, SOFA, and the duration of surgical intervention were independent risk factors for myocardial injury (all P < 0.05). See Table 2. SOFA had the largest area under the ROC curve (AUC=0.827) for predicting the risk of myocardial injury, followed by BNP (AUC=0.709). See Figure 1.
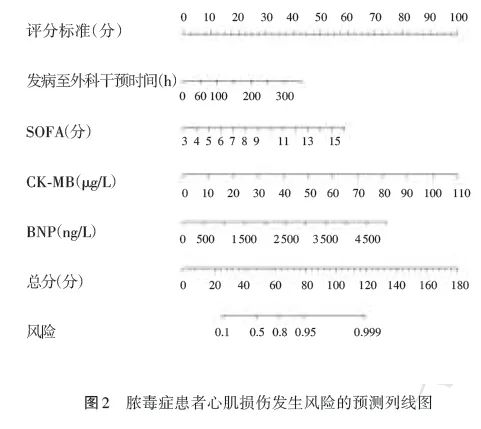
2.3 Nomogram Prediction Model for Risk of Myocardial Injury in Sepsis Patients
The four statistically significant variables from the multivariate logistic regression model were included in the nomogram prediction model for the risk of myocardial injury in sepsis patients (Figure 2). Interpretation of the nomogram: Each variable is represented on the horizontal axis, and a vertical line is drawn upward to find the corresponding score on the “scoring criteria”; the scores of the four variables are summed to obtain the total score; the total score is then traced downward to find the corresponding value on the “risk” axis, which is the predicted risk value for that patient. For example, for a newly admitted sepsis patient, if the time from onset to surgical intervention is 48 hours, SOFA is 10 points, laboratory results indicate CK-MB is 30 μg/L, and BNP is 800 ng/L, the total score for this patient would be 6 + 32 + 28 + 18 = 84 points, with the nomogram risk prediction value approximately 96%, indicating a high risk of myocardial injury.
2.4 Clinical Applicability Analysis of the Nomogram Prediction Model
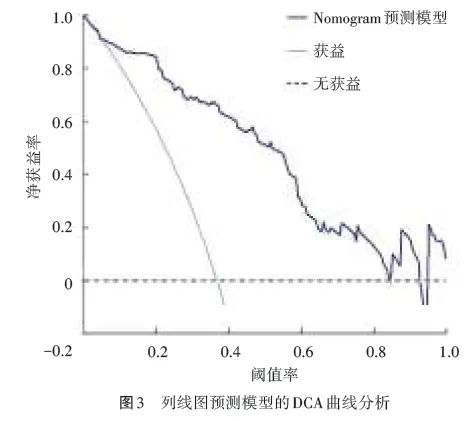
The occurrence of myocardial injury in sepsis patients was taken as the dependent variable, and the risk prediction values obtained from the nomogram prediction model were taken as independent variables to draw the DCA curve of the nomogram prediction model. As shown in Figure 3, when the prediction threshold is between 0.02 and 0.83, the DCA curve does not intersect with the two extreme curves, indicating that the net benefit rate of the nomogram prediction model is higher than that of both full intervention and no intervention, suggesting that the nomogram model has good clinical applicability.
2.5 Internal Validation of the Nomogram Prediction Model
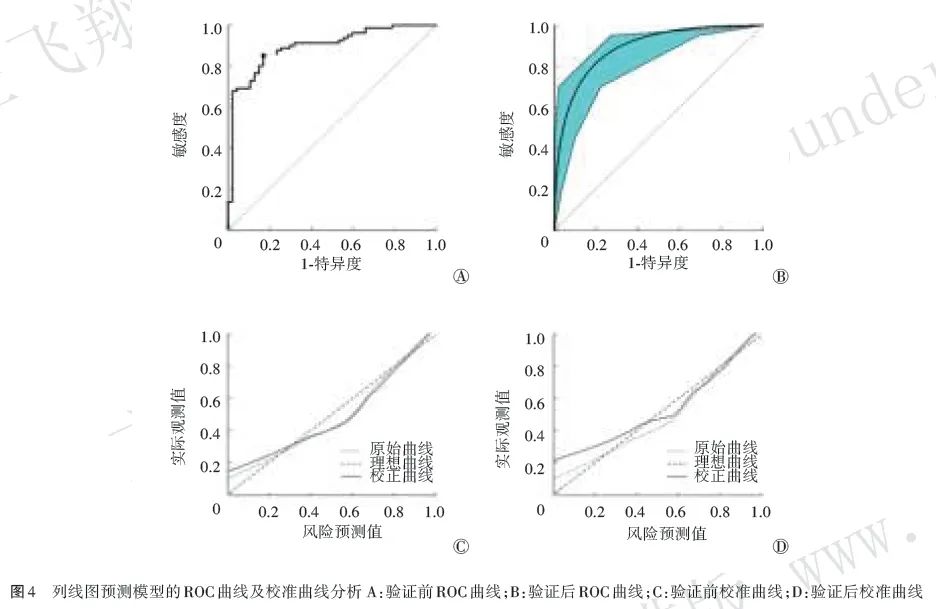
Bootstrap resampling was performed 1,000 times to internally validate the nomogram prediction model to evaluate its stability and reliability. The Hosmer-Lemeshow test found no statistically significant difference between the predicted values and actual values of the model (χ2=4.58, P=0.802). Figure 4 shows that the AUC values before and after internal validation of the nomogram were 0.895 (95% CI 0.838~0.952) and 0.891 (95% CI 0.826~0.941), respectively, both greater than the AUC value of any single variable prediction shown in Figure 1. The sensitivity before and after internal validation was 0.852 and 0.812, and the specificity was 0.830 and 0.803, respectively, indicating good discrimination ability of the model. The calibration curve indicated that the average absolute error of the nomogram prediction model was small before and after internal validation, being 0.049 and 0.051, respectively, suggesting good calibration and consistency of the model.
3 Discussion
3.1 Analysis of Risk Factors for Myocardial Injury After Surgery in Sepsis Patients
This study determined the independent risk factors for SIMD occurring after surgery in sepsis patients based on retrospective cohort study data and using multivariate logistic regression analysis. SOFA can accurately reflect the prognosis of multiple organ dysfunction syndrome and sepsis. In this study, SOFA was identified as an independent risk factor for SIMD after surgery in sepsis patients, and SOFA had the highest predictive value for the risk of myocardial injury (AUC=0.827), suggesting good predictive value for SIMD. The subjects of this study were all sepsis patients who underwent surgical intervention, and by analyzing the time of surgical intervention for the infection focus in sepsis patients, it was found that delayed surgical intervention time is an independent risk factor for SIMD after surgery in sepsis patients. Timely surgical drainage can reduce the risk of myocardial injury in sepsis.
3.2 Nomogram Model for Myocardial Injury After Surgery in Sepsis Patients
This study identified four independent risk factors affecting the occurrence of SIMD after surgery in sepsis patients through logistic regression and constructed a personalized nomogram prediction model based on this. The model was tested to have good applicability. The nomogram prediction model for predicting the risk of SIMD after surgery in sepsis patients has high predictive value and clinical application value. Clinical personnel can use it to screen high-risk SIMD patients after surgery and develop targeted preventive measures to reduce the occurrence of myocardial injury due to sepsis.
In summary, this study selected variables through the LASSO regression model, and multivariate logistic regression analysis determined that BNP, CK-MB, SOFA, and duration of surgical intervention are independent risk factors for SIMD occurring after surgery in sepsis patients, ultimately establishing a nomogram prediction model. The ROC curve, calibration curve, and DCA curve confirmed that this model has good discrimination and predictive efficacy, allowing for a quantitative assessment of the risk level of SIMD occurrence after surgery in sepsis patients, demonstrating clinical practicality and aiding in the early identification of high-risk groups to improve prognosis.
If you are interested in this article, you can log in to our journal’s submission system platform (www.gjmzyfs.com), and download the full text for free in real-time in the “Journal Browsing” section.
International Journal of Anesthesiology and Resuscitation
International Journal of Anesthesiology and Resuscitation
Supervisor: National Health Commission of the People’s Republic of China
Sponsored by: Chinese Medical Association, Xuzhou Medical University
ISSN: 1673-4378 CN: 32-1761/R
Phone: (0516) 85708135 (Consultation); 85807157 (Editorial); 85802018 (Fax)
Email: [email protected]; [email protected]
Online Submission: www.gjmzyfs.com
Address: No. 99 Huaihai West Road, Xuzhou City
Long press the QR code
One-click follow

Quickly view the “International Journal of Anesthesiology and Resuscitation” by following the Gu Ma Jin Zui website.