With the continuous advancement of medical technology, left atrial appendage closure (LAAC) has become increasingly widespread in clinical applications, bringing hope to many patients with atrial fibrillation. Antithrombotic therapy runs through the entire process of LAAC and is one of the core issues of LAAC. However, there is currently no consensus on how to formulate the best antithrombotic therapy plan after LAAC. For different patients, how to lay a solid foundation for anticoagulation during the perioperative period and prevent device-related thrombus (DRT) after surgery is also a current focus and difficulty of research. At the 18th Oriental Cardiology Conference and World Cardiology Conference (OCC-WCC 2024), Professors Huang He and Liu Yu from Wuhan University People’s Hospital shared the latest research progress on anticoagulation therapy after LAAC.
① Prevent the formation of DRT;
② Prevent thromboembolic events, including bleeding and thrombus risks.
✧ The incidence of DRT varies slightly among different studies, with a common incidence currently believed to be 3%-5%.
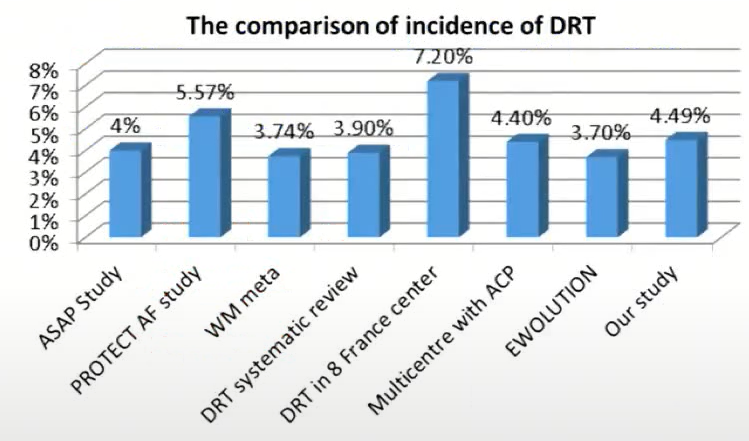
Figure 1 Incidence of DRT
✧ A meta-analysis published in Circulation in 2018, which summarized data from four clinical studies (PROTECT-AF, PREVAIL, CAP, CAP2) involving a total of 1739 patients, found that the incidence of DRT was 3.7%.
✧ The AMPLATZER Amulet global prospective clinical study included 1088 patients and found that its DRT incidence was 1.7% per year.
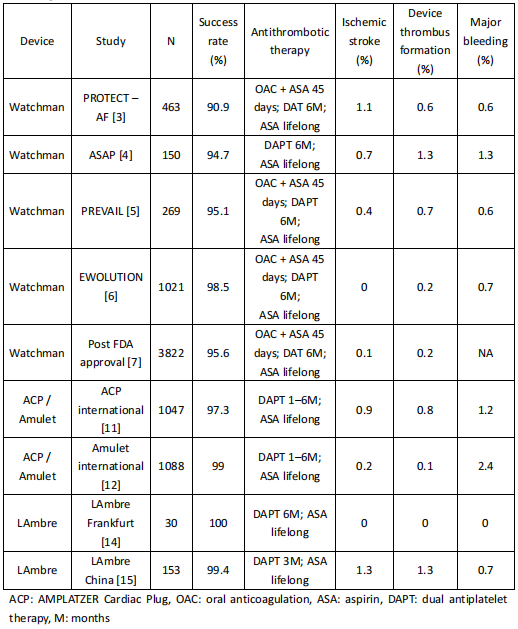
Current guidelines and consensus recommendations for antithrombotic strategies after LAAC are mostly based on regimens from relevant devices in clinical trials. For example, the Watchman device was given oral anticoagulants (OAC) + aspirin (ASA) for 45 days in early clinical trials, followed by dual antiplatelet therapy (DAPT) for 6 months and lifelong ASA. For ACP and LAmbre devices, clinical trials often administered DAPT for 3-6 months, followed by lifelong ASA.
Table 1 Antithrombotic Regimens After LAAC in Clinical Studies
In actual clinical practice, due to factors such as patients’ underlying diseases, postoperative antithrombotic therapy strategies may vary.
✧ In the EWOLUTION study, more than half of the patients received DAPT treatment after surgery without OAC. The EWOLUTION study also suggested that the effects of new oral anticoagulants (NOAC), vitamin K antagonists (VKA), and DAPT seem to be comparable.
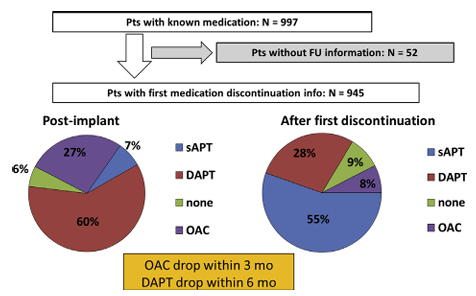 Figure 2 Anticoagulant Drug Use Process After WATCHMAN Implantation at 1 Year
Figure 2 Anticoagulant Drug Use Process After WATCHMAN Implantation at 1 Year
✧ A study published in Am J Cardiol in 2017 showed that levels of coagulation-related biomarkers (prothrombin fragment 1+2 and antithrombin III) increased after LAAC, while platelet-related biomarkers showed no significant changes. Therefore, the anticoagulation requirements after LAAC may be higher.
✧ A study published in Circ Cardiovasc Interv in 2020 also showed that 7 days after LAAC, levels of coagulation-related biomarkers primarily increased, and patients with DRT had significantly higher levels of these biomarkers compared to those without DRT, further confirming coagulation activation after LAAC.
✧ The ADRIFT study showed that administering OAC after LAAC, even at half-dose rivaroxaban, significantly reduced coagulation-related biomarkers.
✧ An observational study published in J Am Coll Cardiol Intv in 2019 explored the effects of OAC and APT after LAAC. The results showed that both treatment strategies had no significant impact on embolic events, but OAC reduced the proportion of DRT. Even excluding patients receiving single antiplatelet therapy (SAPT), OAC still showed benefits compared to DAPT patients.
✧ Results from the NCDR-LAAO registry study showed that the effects of OAC alone and OAC + APT were comparable, but OAC significantly reduced the risk of bleeding.
✧ A study published in N Engl J Med in 2020 explored the effects of OAC alone and OAC + APT after transcatheter aortic valve implantation (TAVI), where 95% of patients had concurrent atrial fibrillation. The results showed that the risk of bleeding events was lower in the OAC group compared to the OAC + APT group.
Early anticoagulants were mainly warfarin, and we have now entered the NOAC era. Multiple clinical studies suggest that NOAC is effective.
NOAC primarily includes factor Xa inhibitors (rivaroxaban and apixaban) and direct thrombin inhibitors (dabigatran). A study by Academician Ge Junbo’s team at Fudan University Zhongshan Hospital showed that factor Xa inhibitors have advantages over direct thrombin inhibitors in preventing DRT after LAAC. The main reason is that dabigatran may activate platelets and promote thrombus formation.
Currently, the percutaneous left atrial appendage occlusion devices available for clinical use mainly include plug-type (Watchman) and disc-type (Amulet).
The Amulet IDE study aimed to explore the safety and efficacy of Watchman and Amulet in preventing stroke in atrial fibrillation. The postoperative antithrombotic regimens for the two groups of patients were different, with OAC primarily used after Watchman and DAPT primarily used after Amulet, and the risk of endpoint events was similar in both groups. In absolute terms, the DRT proportion was lower in the Amulet group. This study suggests that DAPT may be more suitable for disc occlusion devices.
A study published in EuroIntervention in 2024 assessed the long-term safety and efficacy of SAPT strategy using the Amplatzer device after LAAC. The results showed that the incidence of DRT after LAAC was only 1.5%; a study published in Rev Esp Cardiol in 2024 also showed that using the LAmbre device for LAAC with SAPT treatment had a low DRT proportion. It is worth noting that both studies had relatively small sample sizes.
A study by Fauchier et al. published in J Am Coll Cardiol in 2018 explored the incidence and predictive factors of DRT in patients with atrial fibrillation undergoing LAAC. The results showed that the incidence of DRT after LAAC was 7.2%. Predictive factor analysis found that OAC and DAPT were protective factors, while SAPT may increase embolic risk.
At the same time, Professor Lin Yixian’s team from Hong Kong Canossa Hospital compared the baseline characteristics and clinical outcomes of Fauchier et al.’s study and patients from the PWH registry system. The baseline characteristics of the two groups were similar, with no patients (0%) in the PWH registry receiving SATP or not receiving OAC, while this proportion was 44% in Fauchier et al.’s study. The results showed that the proportion of DRT in Fauchier et al.’s study was doubled compared to the PWH registry (7.2% vs 3.3%).
Previously, clinical attention focused on the occurrence rate of DRT at 45 days and within the first 3 months after LAAC. However, actual clinical observations found that the occurrence rate of DRT remained high after six months (during the SAPT phase).
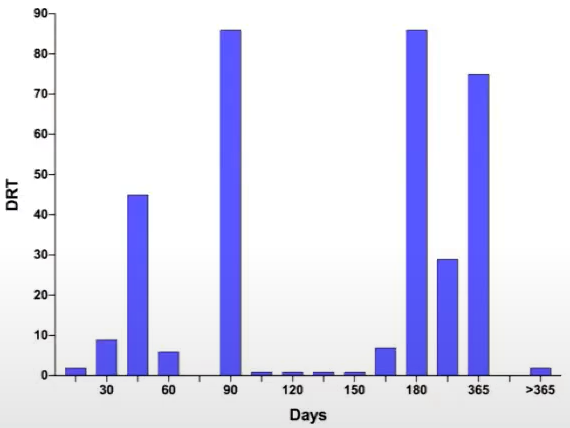 Figure 3 Incidence of DRT
Figure 3 Incidence of DRT
A study published in JACC Cardiovasc Interv in 2021 explored the long-term efficacy of half-dose direct oral anticoagulant therapy (DOAC) compared to standard antithrombotic therapy after LAAC. The results showed that, after LAAC, long-term half-dose DOAC significantly reduced the composite endpoint risk of DRT, thromboembolism, and major bleeding events compared to standard antithrombotic therapy based on APT.
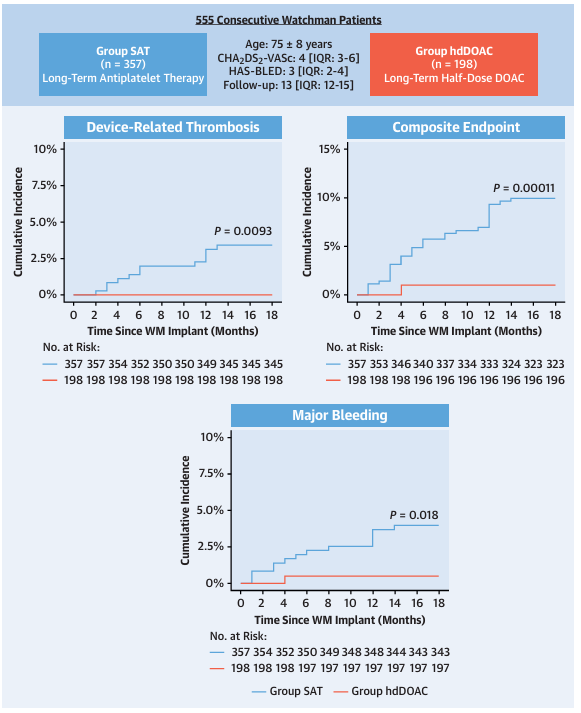 Figure 4 Major Endpoints
Figure 4 Major Endpoints
A meta-analysis published in J Am Coll Cardiol in 2023 included 41 studies with a total of 12,451 patients, aiming to explore the best antithrombotic strategy after LAAC. The results showed that the embolic risk and major bleeding risk were lowest with the use of NOAC alone; the DAPT group had a lower embolic risk compared to the SAPT group.
Some experts believe that antithrombotic therapy after LAAC should be tailored to the individual characteristics of patients. An article published in Circ Cardiovasc Interv in 2023 suggested that if a patient can tolerate full-dose DOAC for a short term, DOAC should be the first choice, with VKA as the second choice; if a patient cannot tolerate full-dose DOAC for a short term, DAPT or low-dose DOAC can be chosen; if a patient has contraindications to anticoagulation, SAPT can be administered or no treatment can be performed.
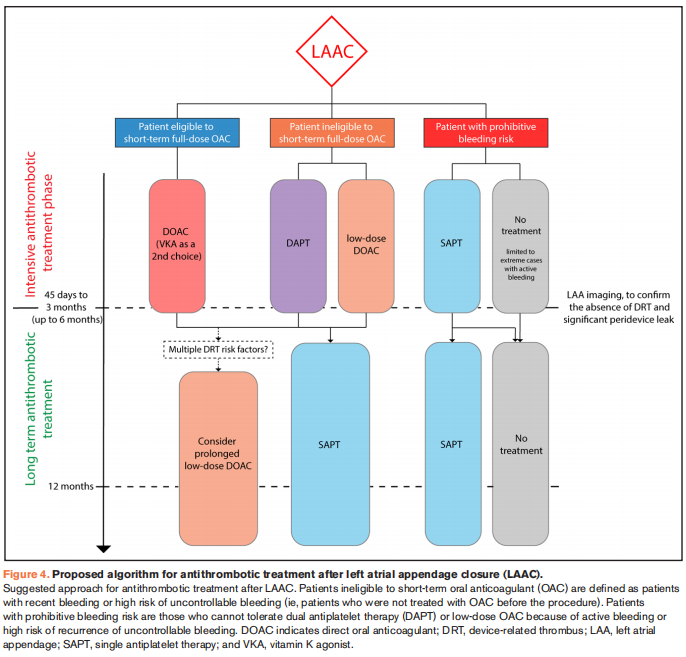 Figure 5 Antithrombotic Treatment Strategy After LAAC
Figure 5 Antithrombotic Treatment Strategy After LAAC
Professor Liu Yu stated that in the long run, for populations at extremely high risk of DRT, extending the duration of low-dose OAC may be appropriate.
The “Intervention for Left Atrial Appendage to Prevent Thromboembolic Events in Patients with Atrial Fibrillation: Current Understanding and Recommendations (2023)” emphasizes:
✧ Antithrombotic strategies should be individualized based on the schemes from different occluder clinical studies and the patient’s bleeding/thrombus risk, and adjusted according to imaging follow-ups after LAAC to check for residual shunts (PDL) or DRT.
✧ For patients without contraindications to anticoagulation: anticoagulation treatment for 45 days (standard dose NOAC or warfarin alone or in combination with ASA), followed by discontinuation of OAC after transesophageal echocardiography (TEE) to exclude DRT and PDL >5mm, changing to postoperative DAPT for 3-6 months, and then long-term ASA.
✧ For patients with contraindications to anticoagulation: DAPT is recommended as the basic scheme for antithrombotic therapy after LAAC, considering bleeding risks and using DAPT for 3-6 months, followed by long-term ASA.
✧ For LAAC combined with catheter ablation in a one-stop procedure: OAC for 2 months, and after TEE to exclude DRT and PDL, switch to DAPT for 3-6 months, followed by long-term ASA.
Currently, there is still a lack of high-quality clinical evidence for antithrombotic strategies after LAAC, and multiple ongoing clinical trials are exploring the best antithrombotic strategies. Professor Liu believes that in the future, there will be more clinical data on antithrombotic strategies after LAAC, which will answer some difficult questions.
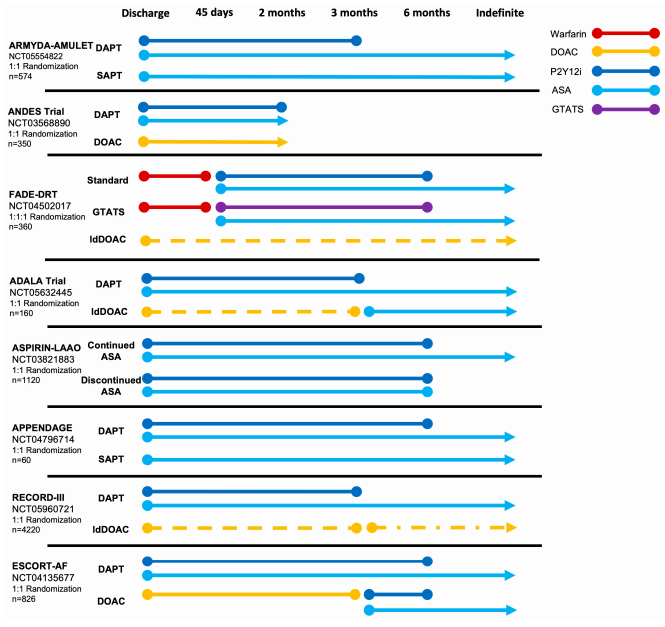 Figure 6 Ongoing Randomized Trials Exploring Antithrombotic Strategies After LAAC
Figure 6 Ongoing Randomized Trials Exploring Antithrombotic Strategies After LAAC
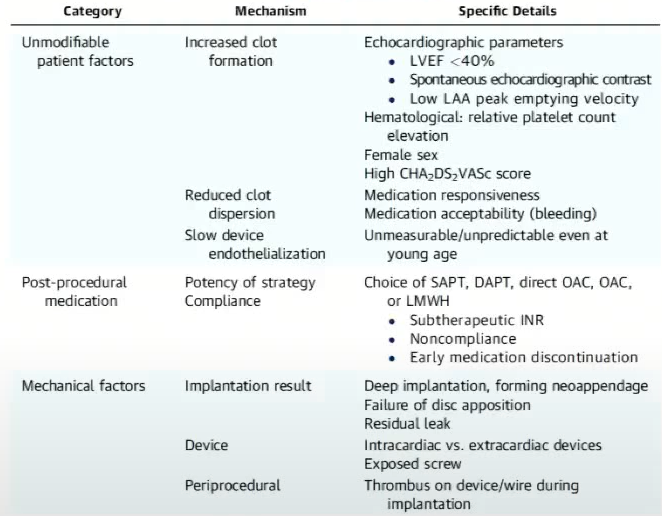
For the antithrombotic strategies after LAAC, medication is only one aspect; the patient’s mechanical characteristics and surgical quality are also important factors affecting the incidence of DRT, which requires clinicians to enhance their ability to screen and differentiate patients.
Table 2 Risk Factors for DRT
✧ Antithrombotic regimens after LAAC should consider comprehensive factors such as thrombus/bleeding risks and device types;
✧ Based on pathophysiological mechanisms, if patients can tolerate anticoagulation therapy, the application of OAC after surgery may be more reasonable;
✧ OAC alone may reduce bleeding risks compared to OAC + APT, and the clinical net benefit may be greater;
✧ The use of NOAC for anticoagulation after LAAC is safe, effective, and convenient;
✧ For disc occlusion devices, existing evidence suggests that DAPT is safe and effective;
✧ In addition to antithrombotic drugs, attention should be paid to other factors that promote DRT and thromboembolic events.
