MorphologyMorphologyPeripheral blood specimenPeripheral blood specimen
A well-prepared and well-stained peripheral blood smear should be examined and correlated with the patient’s blood counts. Cytology of leukocytes, red blood cells, and platelets should be evaluated. A manual 200-cell leukocyte differential count (or counting of all available cells in markedly leukopenic cases) should be performed as part of the evaluation of all myeloid neoplasms. The following cells should be enumerated as a proportion of peripheral blood leukocytes (excluding nucleated red blood cells [nRBCs]): segmented neutrophils, bands, myelocytes, metamyelocytes, promyelocytes, blasts, monocytes, promonocytes, basophils, eosinophils, and lymphocytes. The nRBC count should be expressed as the number of nRBCs counted per 100 leukocytes. If circulating neoplastic cells from a concomitant nonmyeloid neoplasm (such as a lymphoma or plasma cell leukemia) are present, they should be excluded from the white blood count and leukocyte differential count when applying thresholds for the diagnosis of myeloid neoplasms.
A well-prepared and well-stained peripheral blood smear should be examined and correlated with the patient’s blood counts. Cytology of leukocytes, red blood cells, and platelets should be evaluated. A manual 200-cell leukocyte differential count (or counting of all available cells in markedly leukopenic cases) should be performed as part of the evaluation of all myeloid neoplasms. The following cells should be enumerated as a proportion of peripheral blood leukocytes (excluding nucleated red blood cells [nRBCs]): segmented neutrophils, bands, myelocytes, metamyelocytes, promyelocytes, blasts, monocytes, promonocytes, basophils, eosinophils, and lymphocytes. The nRBC count should be expressed as the number of nRBCs counted per 100 leukocytes. If circulating neoplastic cells from a concomitant nonmyeloid neoplasm (such as a lymphoma or plasma cell leukemia) are present, they should be excluded from the white blood count and leukocyte differential count when applying thresholds for the diagnosis of myeloid neoplasms.
Bone marrow aspirate specimen
Bone marrow aspirate specimen
Well-prepared direct smears or buffy coat smears from aspirated bone marrow should be prepared and examined. If spiculated aspirate material cannot be obtained due to “dry tap,” touch preparations of the biopsy should be prepared (taking care to avoid damage to the core biopsy). Aspirate and touch preparations should be stained with Wright-Giemsa or May-Grünwald-Giemsa, and extra unstained smears should be prepared for possible iron or cytochemical stains.
Well-prepared direct smears or buffy coat smears from aspirated bone marrow should be prepared and examined. If spiculated aspirate material cannot be obtained due to “dry tap,” touch preparations of the biopsy should be prepared (taking care to avoid damage to the core biopsy). Aspirate and touch preparations should be stained with Wright-Giemsa or May-Grünwald-Giemsa, and extra unstained smears should be prepared for possible iron or cytochemical stains.
At least 500 nucleated bone marrow cells should be counted from areas close to spicules to avoid hemodilution or from more cellular areas of buffy coat smears, ideally obtaining counts from several different areas of the smear(s). The following cells should be individually enumerated as a proportion of all nucleated cells: segmented neutrophils, bands, myelocytes, metamyelocytes, promyelocytes, blasts, monocytes, promonocytes, basophils, eosinophils, lymphocytes, plasma cells, and erythroid precursors; it is acceptable to count segmented neutrophils, bands, myelocytes, and metamyelocytes together in one group of granulocytes and myeloid precursors, since the relative proportion of these cells does not impact classification of any myeloid neoplasm. Mast cells should only be included in the differential if mastocytosis is under diagnostic consideration. In cases where pure erythroid leukemia is a diagnostic consideration (see Chapters 32 and 35), pronormoblasts should be enumerated separately from maturing erythroid precursors. Although megakaryocytes are not included in the formal cell count, their presence and estimated frequency should be mentioned in the report. If a concomitant nonmyeloid neoplasm is present, these neoplastic cells should be excluded when applying thresholds for the purpose of classifying a myeloid neoplasm.
At least 500 nucleated bone marrow cells should be counted from areas close to spicules to avoid hemodilution or from more cellular areas of buffy coat smears, ideally obtaining counts from several different areas of the smear(s). The following cells should be individually enumerated as a proportion of all nucleated cells: segmented neutrophils, bands, myelocytes, metamyelocytes, promyelocytes, blasts, monocytes, promonocytes, basophils, eosinophils, lymphocytes, plasma cells, and erythroid precursors; it is acceptable to count segmented neutrophils, bands, myelocytes, and metamyelocytes together in one group of granulocytes and myeloid precursors, since the relative proportion of these cells does not impact classification of any myeloid neoplasm. Mast cells should only be included in the differential if mastocytosis is under diagnostic consideration. In cases where pure erythroid leukemia is a diagnostic consideration (see Chapters 32 and 35), pronormoblasts should be enumerated separately from maturing erythroid precursors. Although megakaryocytes are not included in the formal cell count, their presence and estimated frequency should be mentioned in the report. If a concomitant nonmyeloid neoplasm is present, these neoplastic cells should be excluded when applying thresholds for the purpose of classifying a myeloid neoplasm.
Cytology of megakaryocytes, nucleated erythroids, and myeloid elements should be evaluated, as well as the cytology of blasts if increased and any other cell types that appear morphologically abnormal. The differential counts obtained from marrow aspirates should be compared with an estimate of the cells observed in corresponding biopsy sections in order to determine possible sampling artifacts, including hemodilution of the aspirate specimen.
Cytology of megakaryocytes, nucleated erythroids, and myeloid elements should be evaluated, as well as the cytology of blasts if increased and any other cell types that appear morphologically abnormal. The differential counts obtained from marrow aspirates should be compared with an estimate of the cells observed in corresponding biopsy sections in order to determine possible sampling artifacts, including hemodilution of the aspirate specimen.
Bone marrow trephine biopsy specimen
Bone marrow trephine biopsy specimen
The bone marrow biopsy provides information that is critical to the classification of myeloid neoplasms: hematopoietic cellularity, hematopoietic architecture, the relative proportions, maturation, and cytology of hematopoietic cells, and abnormalities of bone marrow stroma, particularly increased marrow fibrosis. The biopsy also provides material for immunohistochemical studies that may aid in diagnosis and classification. The biopsy specimen should optimally be taken at a right angle to the cortical bone, and be at least 1.5 cm in length, to enable evaluation of multiple intertrabecular areas of hematopoietic marrow. The bone marrow specimen should be well fixed, decalcified by a method that preserves cytomorphology and antigen immunogenicity, and thinly sectioned (at 2-4 μm). The biopsy should be stained with hematoxylin and eosin; Giemsa stain (which facilitates visualization of mast cells) and/or periodic acid-Schiff stain (which facilitates the visualization of megakaryocytes) also may be performed. A cell block prepared from clotted aspirate material may be fixed and evaluated similarly to the bone marrow biopsy specimen.
The bone marrow biopsy provides information that is critical to the classification of myeloid neoplasms: hematopoietic cellularity, hematopoietic architecture, the relative proportions, maturation, and cytology of hematopoietic cells, and abnormalities of bone marrow stroma, particularly increased marrow fibrosis. The biopsy also provides material for immunohistochemical studies that may aid in diagnosis and classification. The biopsy specimen should optimally be taken at a right angle to the cortical bone, and be at least 1.5 cm in length, to enable evaluation of multiple intertrabecular areas of hematopoietic marrow. The bone marrow specimen should be well fixed, decalcified by a method that preserves cytomorphology and antigen immunogenicity, and thinly sectioned (at 2-4 μm). The biopsy should be stained with hematoxylin and eosin; Giemsa stain (which facilitates visualization of mast cells) and/or periodic acid-Schiff stain (which facilitates the visualization of megakaryocytes) also may be performed. A cell block prepared from clotted aspirate material may be fixed and evaluated similarly to the bone marrow biopsy specimen.
The bone marrow biopsy cellularity should be provided as part of the pathology report for all myeloid neoplasms. The cellularity should be expressed as a percentage, calculated as the proportion of the intertrabecular marrow area (excluding vascular spaces) occupied by hematopoietic cells (both neoplastic and nonneoplastic). Cellularity estimation should optimally be performed in areas devoid of artifacts such as intertrabecular hemorrhage and crushed tissue and should exclude subcortical areas of nonhematopoietic fatty marrow. When variable, the overall cellularity across the entire evaluable marrow should be reported. Marrow may be normocellular, hypocellular, or hypercellular based on the percentage cellularity relative to the patient’s age (age-adjusted cellularity); the recommended ranges are shown in Table 2. Although there is good interobserver reproducibility in estimating bone marrow cellularity, in the future artificial intelligence technologies may provide more accurate assessments. Machine learning–based analysis of bone marrow biopsy images may also inform the future diagnosis and classification of MDS and other myeloid neoplasms, by revealing novel morphologic features and mitigating subjectivity in interpreting well-established cytologic abnormalities.
The bone marrow biopsy cellularity should be provided as part of the pathology report for all myeloid neoplasms. The cellularity should be expressed as a percentage, calculated as the proportion of the intertrabecular marrow area (excluding vascular spaces) occupied by hematopoietic cells (both neoplastic and nonneoplastic). Cellularity estimation should optimally be performed in areas devoid of artifacts such as intertrabecular hemorrhage and crushed tissue and should exclude subcortical areas of nonhematopoietic fatty marrow. When variable, the overall cellularity across the entire evaluable marrow should be reported. Marrow may be normocellular, hypocellular, or hypercellular based on the percentage cellularity relative to the patient’s age (age-adjusted cellularity); the recommended ranges are shown in Table 2. Although there is good interobserver reproducibility in estimating bone marrow cellularity, in the future artificial intelligence technologies may provide more accurate assessments. Machine learning–based analysis of bone marrow biopsy images may also inform the future diagnosis and classification of MDS and other myeloid neoplasms, by revealing novel morphologic features and mitigating subjectivity in interpreting well-established cytologic abnormalities.
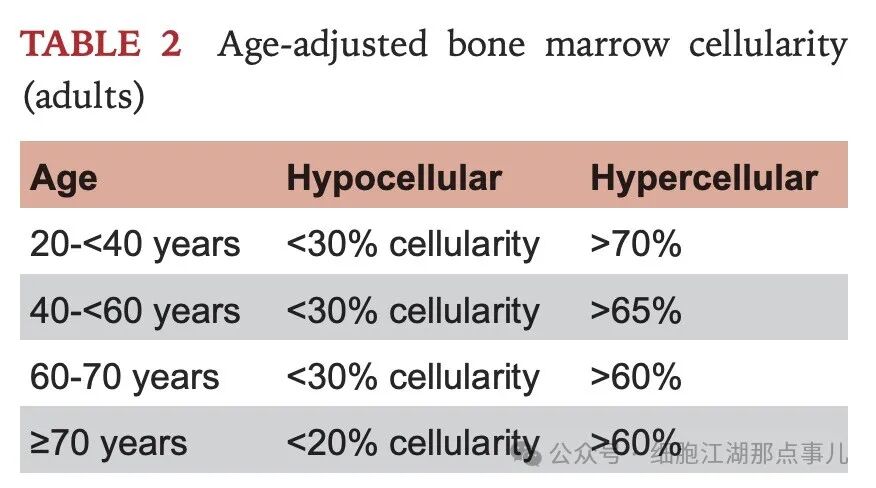
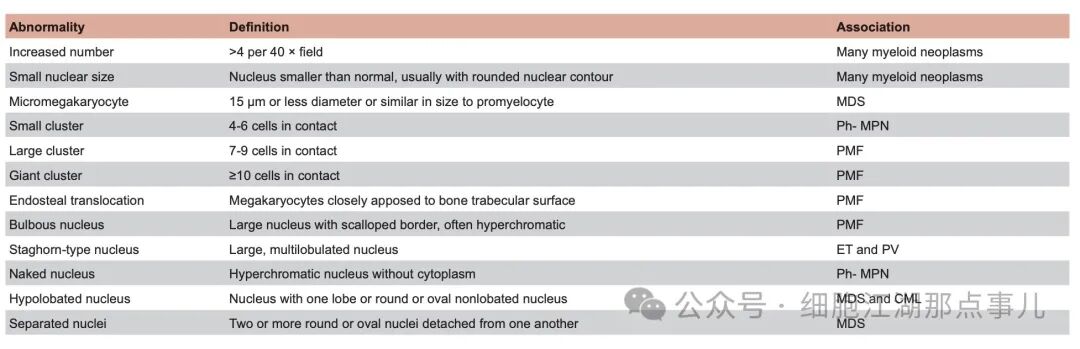
Megakaryocytes typically occur as single cells distributed evenly in the marrow space; approximately 3 to 4 megakaryocytes are seen per 40× field on average. Megakaryocytes can be regarded as increased or decreased if they are appreciably higher or lower in number. Megakaryocyte topography and cytology should be carefully evaluated and are key features in the classification of myeloid neoplasms, particularly MPN. Definitions of abnormalities in megakaryocyte number, topography, and cytology are shown in Table 3. The relative proportion (myeloid:erythroid ratio) and maturation of erythroid and myeloid elements in the biopsy should also be evaluated.
Megakaryocytes typically occur as single cells distributed evenly in the marrow space; approximately 3 to 4 megakaryocytes are seen per 40× field on average. Megakaryocytes can be regarded as increased or decreased if they are appreciably higher or lower in number. Megakaryocyte topography and cytology should be carefully evaluated and are key features in the classification of myeloid neoplasms, particularly MPN. Definitions of abnormalities in megakaryocyte number, topography, and cytology are shown in Table 3. The relative proportion (myeloid:erythroid ratio) and maturation of erythroid and myeloid elements in the biopsy should also be evaluated.

Identification and morphologic evaluation of blasts in the biopsy and aspirate smear
Identification and morphologic evaluation of blasts in the biopsy and aspirate smear
Morphologic identification and enumeration of blasts in the bone marrow and peripheral blood is critical for the classification of all myeloid neoplasms. Marrow blast enumeration should be performed on the aspirate smear or touch preparation if an aspirate is unobtainable or markedly hemodilute. Immunohistochemical staining for CD34 on the biopsy specimen highlights CD34+ blasts that can be enumerated, although in some myeloid neoplasms the blasts do not express CD34. It may be appropriate to use the CD34+ blast estimate on the biopsy specimen in lieu of the aspirate blast count in the following instances: (1) The aspirate smear is unobtainable due to dry tap and a touch preparation is not available or not evaluable; (2) the aspirate smear/touch prep are compromised due to hemodilution or other artifacts; (3) sampling artifact is suggested by a larger number of blasts seen in the biopsy compared with the aspirate smear, including cases with focal aggregates or sheets of blasts in the biopsy. In cases where blasts are known to be CD34 negative and are CD117+, CD117 immunostaining can be used to estimate blasts; however, CD117 also stains early erythroid elements, promyelocytes, and mast cells and thus blasts may be overestimated based on CD117 immunostaining. Flow cytometry determination of blast percentage should not be used as a substitute for visual counting of blasts: flow cytometry samples of bone marrow aspirate can be hemodilute and can also be affected by a number of preanalytic variables, such as loss or exclusion of nucleated erythroid cells.
Morphologic identification and enumeration of blasts in the bone marrow and peripheral blood is critical for the classification of all myeloid neoplasms. Marrow blast enumeration should be performed on the aspirate smear or touch preparation if an aspirate is unobtainable or markedly hemodilute. Immunohistochemical staining for CD34 on the biopsy specimen highlights CD34+ blasts that can be enumerated, although in some myeloid neoplasms the blasts do not express CD34. It may be appropriate to use the CD34+ blast estimate on the biopsy specimen in lieu of the aspirate blast count in the following instances: (1) The aspirate smear is unobtainable due to dry tap and a touch preparation is not available or not evaluable; (2) the aspirate smear/touch prep are compromised due to hemodilution or other artifacts; (3) sampling artifact is suggested by a larger number of blasts seen in the biopsy compared with the aspirate smear, including cases with focal aggregates or sheets of blasts in the biopsy. In cases where blasts are known to be CD34 negative and are CD117+, CD117 immunostaining can be used to estimate blasts; however, CD117 also stains early erythroid elements, promyelocytes, and mast cells and thus blasts may be overestimated based on CD117 immunostaining. Flow cytometry determination of blast percentage should not be used as a substitute for visual counting of blasts: flow cytometry samples of bone marrow aspirate can be hemodilute and can also be affected by a number of preanalytic variables, such as loss or exclusion of nucleated erythroid cells.
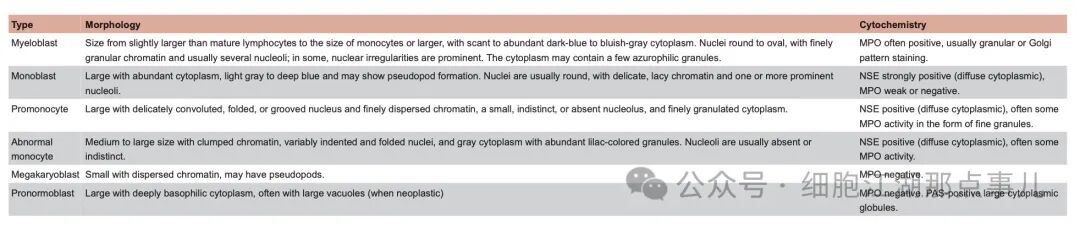
For the purposes of myeloid neoplasm classification, the following cells are counted as blasts: myeloblasts, monoblasts, and megakaryoblasts. Additionally, promonocytes are considered as blast equivalents and included in the overall blast count for all myeloid neoplasms, although caution must be exercised to correctly identify promonocytes and distinguish them from immature or reactive monocytes; monocytes, whether cytologically normal or abnormal, are never considered as blast equivalents. Promyelocytes are only regarded as blast equivalents in the setting of PML::RARA rearrangement (acute promyelocytic leukemia). Pronormoblasts are only regarded as blast equivalents in the setting of pure erythroid leukemia (see Chapters 32 and 35). Descriptions and immunophenotypes of the various blast and blast equivalent cell types are shown in Table 4.
For the purposes of myeloid neoplasm classification, the following cells are counted as blasts: myeloblasts, monoblasts, and megakaryoblasts. Additionally, promonocytes are considered as blast equivalents and included in the overall blast count for all myeloid neoplasms, although caution must be exercised to correctly identify promonocytes and distinguish them from immature or reactive monocytes; monocytes, whether cytologically normal or abnormal, are never considered as blast equivalents. Promyelocytes are only regarded as blast equivalents in the setting of PML::RARA rearrangement (acute promyelocytic leukemia). Pronormoblasts are only regarded as blast equivalents in the setting of pure erythroid leukemia (see Chapters 32 and 35). Descriptions and immunophenotypes of the various blast and blast equivalent cell types are shown in Table 4.
|
Cell Type |
Morphological Features |
Chemical Staining |
|
Myeloblasts |
Cell size ranges from slightly larger than mature lymphocytes to the size of monocytes or larger, with cytoplasm ranging from scant to abundant, appearing deep blue to blue-gray. The nucleus is round to oval, with finely granular chromatin, usually with multiple nucleoli; in some cells, nuclear irregularity is significant. The cytoplasm may contain a few azurophilic granules. |
MPOUsually positive, typically showing granular or Golgi pattern staining |
|
Monoblasts |
Cell body large, cytoplasm abundant, ranging from light gray to deep blue, may show pseudopodia formation. The nucleus is usually round, with fine, reticular chromatin, and one or more prominent nucleoli. |
NSEStrongly positive (diffuse distribution in cytoplasm),MPOweakly positive or negative |
|
Promonocytes |
Cell body large, chromatin finely dispersed, nucleus may appear distorted, folded, or indented, chromatin is finely scattered, nucleoli small, inconspicuous or absent, cytoplasm finely granular |
NSEPositive (diffuse distribution in cytoplasm), usually showing fine granular MPO activity |
|
Abnormal Monocytes |
Cell body medium to large size, chromatin clumped, nuclear shape irregular and folded, cytoplasm gray with abundant pale purple granules. Nucleoli are usually absent or inconspicuous. |
NSEPositive (diffuse distribution in cytoplasm), usually with MPO activity |
|
Megakaryoblasts |
Small and dispersed chromatin, may have pseudopodia. |
MPONegative |
|
Pronormoblasts |
Cell body larger, cytoplasm deeply basophilic, often with large vacuoles (when neoplastic) |
MPONegative. |
Cytochemical stains
Cytochemical studies performed on bone marrow or blood smears can be useful in determining the lineage of blasts and maturing hematopoietic elements; however, in most laboratories they have been supplanted by immunological studies using flow cytometry and are not required for the diagnosis of any ICC entities. The morphologic and cytochemical features of blasts and blast equivalents are summarized in Table 4. In cases of MDS/MPN, nonspecific esterase (NSE) and myeloperoxidase (MPO) staining may be helpful in distinguishing monocytes from dysplastic granulocytic precursors. The presence of MPO or NSE staining by cytochemistry, in addition to immunophenotypic features, can also be used to establish a myeloid lineage component in the diagnosis of a mixed-phenotype acute leukemia (see Chapter 39).
Cytochemical studies performed on bone marrow or blood smears can be useful in determining the lineage of blasts and maturing hematopoietic elements; however, in most laboratories they have been supplanted by immunological studies using flow cytometry and are not required for the diagnosis of any ICC entities. The morphologic and cytochemical features of blasts and blast equivalents are summarized in Table 4. In cases of MDS/MPN, nonspecific esterase (NSE) and myeloperoxidase (MPO) staining may be helpful in distinguishing monocytes from dysplastic granulocytic precursors. The presence of MPO or NSE staining by cytochemistry, in addition to immunophenotypic features, can also be used to establish a myeloid lineage component in the diagnosis of a mixed-phenotype acute leukemia (see Chapter 39).
Reticulin and trichrome stains
Reticulin and trichrome stains
A silver impregnation method to evaluate reticulin fibrosis should be performed on all myeloid neoplasms to quantify the presence and degree of any bone marrow fibrosis. Trichrome stain assists in fibrosis assessment and should be performed in any cases with significantly increased reticulin fibrosis (grade 2 or 3). Bone marrow fibrosis (reticulin and trichrome) should be graded according to the European consensus scoring system.
A silver impregnation method to evaluate reticulin fibrosis should be performed on all myeloid neoplasms to quantify the presence and degree of any bone marrow fibrosis. Trichrome stain assists in fibrosis assessment and should be performed in any cases with significantly increased reticulin fibrosis (grade 2 or 3). Bone marrow fibrosis (reticulin and trichrome) should be graded according to the European consensus scoring system.
Iron stain
Iron stain
Although iron stains can be performed on both aspirate and biopsy tissue specimens, evaluation for ring sideroblasts and storage iron should always be performed on the bone marrow aspirate (or touch prep), since iron is leached out in the decalcification and processing of the biopsy specimen. Iron staining should be performed in all possible MDS and MDS/MPN cases to evaluate for ring sideroblasts, defined as erythroid precursors with at least five granules of iron, encircling one-third or more of the nucleus. When present, ring sideroblasts should be enumerated as a percentage of all nucleated erythroid elements. Although ring sideroblasts are most sensitively detected in the aspirate smears, they may be identified in some cases in nondecalcified bone marrow clot sections. Iron staining also evaluates for the presence of storage iron, which may be helpful in separating polycythemia vera (which typically lacks stainable iron in the bone marrow) from other types of MPN.
Although iron stains can be performed on both aspirate and biopsy tissue specimens, evaluation for ring sideroblasts and storage iron should always be performed on the bone marrow aspirate (or touch prep), since iron is leached out in the decalcification and processing of the biopsy specimen. Iron staining should be performed in all possible MDS and MDS/MPN cases to evaluate for ring sideroblasts, defined as erythroid precursors with at least five granules of iron, encircling one-third or more of the nucleus. When present, ring sideroblasts should be enumerated as a percentage of all nucleated erythroid elements. Although ring sideroblasts are most sensitively detected in the aspirate smears, they may be identified in some cases in nondecalcified bone marrow clot sections. Iron staining also evaluates for the presence of storage iron, which may be helpful in separating polycythemia vera (which typically lacks stainable iron in the bone marrow) from other types of MPN.