*For medical professionals only


The left atrial appendage closure (LAAC) is an effective alternative treatment to long-term oral anticoagulants (OAC) for preventing thromboembolic events related to non-valvular atrial fibrillation (AF). However, antithrombotic therapy is required after LAAC to prevent device-related thrombus (DRT). The optimal antithrombotic strategy post-LAAC remains unclear. LAAC has been in use for over 10 years, accumulating a substantial body of research evidence regarding antithrombotic therapy, although most of it is based on observational studies.
Recently, the journal Circulation: Cardiovascular Interventions published a review analyzing the clinical evidence for antithrombotic therapy following LAAC and developed a strategy for selecting antithrombotic options for clinical practice. Let’s take a look.
Basic Principles of Antithrombotic Therapy After LAAC
The left atrial appendage closure (LAAC) is an effective alternative to long-term oral anticoagulants (OAC) for preventing embolic events associated with non-valvular atrial fibrillation (AF), primarily used in patients at high risk for both ischemia and bleeding. However, the occurrence of device-related thrombus (DRT) limits the clinical application of LAAC, and bleeding events post-LAAC should not be underestimated, especially during the intensified antithrombotic treatment phase aimed at preventing DRT. Therefore, selecting an appropriate antithrombotic therapy is crucial for preventing both DRT and bleeding events.
Currently, DRT is believed to result from incomplete endothelialization of the device, but our understanding of this process is still limited. We can roughly divide the healing process after device implantation into three stages: The first stage is the acute thrombus-prone state, triggered by direct exposure of the device to the bloodstream; the second stage is the endothelialization process; and the third stage is the stabilization phase where new endothelium covers the device.
Regarding the acute thrombus-prone state, several studies have indicated that it is associated with enhanced coagulation activation. A study involving 43 patients showed that thrombin formation was activated within 7 days post-surgery and only partially returned to baseline levels by 30 days post-surgery, while platelet activation levels did not significantly increase. The ADRIFT study results indicated that using rivaroxaban early (within 10 days) after LAAC significantly reduced coagulation activation levels. Another study involving 78 patients (48 receiving antiplatelet therapy, 30 receiving anticoagulation therapy) also showed similar results. These findings suggest that enhanced coagulation activation post-LAAC may be a significant contributor to early DRT formation.
Concerning the endothelialization process, animal experiments have shown that fibrin can be detected on the surface of the device by the third day post-LAAC, which may represent the first step of device endothelialization. In animal models, endothelialization can be completed within 28-45 days post-LAAC: smooth muscle cells from the endocardium grow inward in a proteoglycan-collagen matrix, replacing fibrin deposits and effectively sealing the device. A similar process has been observed in humans, but the duration extends to 130 days post-surgery. Although the formation mechanisms are quite similar, the speed of endothelialization in humans is slower due to factors such as age, comorbidities, and atrial fibrillation, potentially leading to endothelial dysfunction.
The final stage of the vascular healing process after device implantation is generally considered to be less active, primarily involving the evolution of thrombus closure within the left atrial appendage and the growth of new tissue. However, research on late DRT indicates that even 5 years post-surgery, the thrombus-prone state may be reactivated due to incomplete coverage of the device by the endocardium or damage to the new tissue. The study by Simard et al. showed that 36.3% and 20.3% of DRT occurred at 6 months and 1 year post-surgery, respectively. Furthermore, despite most patients receiving intensified antithrombotic therapy within 45 days post-surgery, a quarter of DRT occurred during this period, and there was no statistical correlation between the antithrombotic treatment regimen and the occurrence of DRT. This indicates that early DRT may not solely be related to coagulation or platelet activation, thus not entirely preventable by pharmacological treatments, which also challenges the long-term effectiveness of antithrombotic therapy post-LAAC. Currently, several factors have been identified as risk factors for DRT, particularly left ventricular systolic dysfunction, previous ischemic events, larger left atrial appendage size, and deeper device implantation (more than 10 mm from the pulmonary ridge). These risk factors should be carefully considered when developing antithrombotic strategies post-LAAC.
Antithrombotic Therapy Regimens After LAAC
Warfarin (VKA) Combined with Aspirin
The PROTECT-AF and PREVAIL studies were designed before the era of direct oral anticoagulants (DOACs) and primarily aimed to assess the preventive effect of LAAC on ischemic events in patients without contraindications to anticoagulation. Patients implanted with the WATCHMAN device underwent combined treatment with aspirin and warfarin for 45 days, followed by dual antiplatelet therapy (DAPT) with aspirin and clopidogrel for 6 months, eventually maintaining long-term aspirin therapy. Based on these study results, this antithrombotic regimen was approved by the FDA for patients after WATCHMAN device implantation. Subsequent analyses showed that among 1,739 patients implanted with the WATCHMAN device, 65 patients (3.74%) experienced 74 instances of DRT, with 14 occurring within 45 days post-surgery, 15 between 45 days to 6 months, 32 between 6-12 months, and 13 after 12 months. The occurrence of DRT was associated with an increased risk of stroke or systemic embolism (RR 3.55 [95% CI, 2.18-5.79], P<0.001), yet 86.6% of ischemic events occurred in patients not diagnosed with DRT. Regarding safety, the pooled analysis results of PROTECT-AF and PREVAIL indicated that compared to the use of VKA alone, the LAAC group did not reduce the incidence of serious bleeding, which may be related to surgical complications and early intensified antithrombotic treatment. After excluding surgical complications, the LAAC group still had a higher incidence of bleeding events during the period of warfarin and aspirin combination therapy, which gradually decreased when patients switched to single-agent aspirin antithrombotic therapy. Considering the high bleeding risk associated with early VKA treatment post-LAAC and the unreliable pharmacokinetics and routine laboratory testing, the current clinical practice tends to favor the use of DOACs or other antithrombotic regimens. The FDA has now approved the new WATCHMAN FLX device along with the antithrombotic regimen used in the PINNACLE FLX study (replacing VKA with DOAC).
Direct Oral Anticoagulants (DOAC)
For patients undergoing LAAC, DOAC may be an effective alternative for short-term anticoagulation therapy. Data on the efficacy and safety of DOAC for antithrombotic therapy post-LAAC are limited and primarily derived from non-randomized controlled trials. The EWOLUTION study indicated that 10.9% of patients received DOAC treatment after LAAC, and although there was no difference in the rate of embolic events among different antithrombotic treatment groups, the DAPT group had the highest DRT incidence (3.1%), while the DOAC group had only 1 case (1.3%). In terms of safety, the bleeding event rate in the DOAC group was the lowest (1.9%, DAPT: 3.8%; VKA: 4.6%). The recently published PINNACLE FLX study (using the second-generation WATCHMAN FLX device) mandated the use of DOAC combined with low-dose aspirin for antithrombotic therapy within the first 45 days post-LAAC, and no DRT occurrences were observed during the 1-year follow-up. The study by Faroux et al. (285 patients, multicenter retrospective study) compared the efficacy and safety of DAPT versus DOAC treatment post-LAAC, showing no significant differences in clinical outcomes between the two groups during the 3-month follow-up. However, compared to DOAC, the DAPT group had a higher early mortality rate (3.7% vs. 1.1%), a higher incidence of major bleeding events (7.4% vs. 3.2%), and a higher rate of serious adverse events (11.1% vs. 5.3%). Additionally, 4 patients (2.6%) in the DAPT group experienced DRT, while none occurred in the DOAC group (P = 0.162). Other single-center retrospective studies also suggest that using DOAC as an antithrombotic regimen post-LAAC can yield good results.
However, the optimal dosing of DOAC remains to be determined. An observational study involving 555 patients compared the clinical outcomes of long-term half-dose DOAC with 45 days of full-dose DOAC combined with aspirin (followed by 6 months of DAPT and lifelong aspirin), reporting a total of 12 DRT cases during 18 months of follow-up, with no DRT occurring in the long-term half-dose DOAC group, which was associated with a lower incidence of major bleeding. Long-term half-dose DOAC may become a potential antithrombotic regimen for preventing ischemic and bleeding events post-LAAC, but existing evidence is primarily based on small-sample, non-randomized controlled clinical studies, which have potential selection biases and confounding factors, thus requiring randomized controlled trials to evaluate the most appropriate antithrombotic strategy post-LAAC. The ANDES and ADALA studies are currently ongoing clinical trials comparing the effects of DOAC versus DAPT on antithrombotic treatment post-LAAC, which may provide more valuable information in the future.
Dual Antiplatelet Therapy (DAPT)
DAPT is a widely used antithrombotic regimen after LAAC. Europe recommends 3 months of DAPT as the primary antithrombotic strategy post-LAAC, and the FDA has also approved 45 days of DAPT as an alternative treatment to OAC combined with aspirin after WATCHMAN FLX device implantation. However, to date, there are no randomized controlled trials assessing the clinical efficacy of DAPT post-LAAC. Compared to OAC, DAPT is primarily used to reduce the bleeding risk after LAAC, mostly applied to patients with a high HAS-BLED score or a history of serious bleeding events. However, it remains unclear whether DAPT can indeed reduce the potential bleeding risk. In non-LAAC patients, some studies have shown that the bleeding risk of DAPT is higher than that of VKA. The Amulet study results indicated that the incidence of serious bleeding events in the DAPT group was twice that of the OAC group (8.4% vs. 4.1%). Moreover, some research results suggest that the incidence of DRT is higher in the DAPT group. A propensity-matched study involving randomized controlled trials and large registry studies found that the incidence of DRT in the antiplatelet treatment group was higher than in the OAC group (1.4% vs. 3.1%; P = 0.014). Other studies have shown no significant differences between DAPT and OAC treatment regarding the incidence of DRT, ischemic events, and bleeding events, but these results are based on observational studies, which may have certain biases. Currently, the ongoing FADE-DRT study includes patients with contraindications to OAC who undergo LAAC, comparing the efficacy and safety of three antithrombotic treatment regimens: DAPT, genotype-guided antithrombotic therapy, and low-dose DOACs.
Other Regimens: Single Antiplatelet Therapy (SAPT) / No Antithrombotic Therapy
Serious bleeding events are an independent risk factor for mortality in patients after cardiac interventional procedures, and serious bleeding occurrences within the first year post-LAAC are not uncommon (5% – 10%). Patients at high bleeding risk may be able to prevent stroke through LAAC but may not tolerate DAPT or short-term OAC antithrombotic regimens after LAAC. In such extreme cases, SAPT or no antithrombotic therapy may be more appropriate. In existing clinical studies, such patients account for approximately 5% to 10%.
Currently, the evidence regarding SAPT or no antithrombotic therapy post-LAAC primarily comes from single-center, observational studies, and the results are inconsistent. Therefore, due to the lack of sufficient evidence, the use of SAPT or no antithrombotic therapy post-LAAC should only be applied to patients selected by expert panels, weighing the individual risks of DRT against serious bleeding.
Long-term Antithrombotic Therapy
Currently, there are still relatively few studies on long-term antithrombotic therapy strategies post-LAAC. Based on clinical experiences with other cardiac implanted devices, most studies currently consider single-agent aspirin as a choice for long-term antithrombotic therapy. However, it should be noted that one-third of DRT occurs within 6 months post-LAAC, and long-term SAPT treatment significantly increases the risk of bleeding. Long-term SAPT treatment provides little benefit in preventing ischemic events in patients with non-valvular atrial fibrillation while increasing bleeding risk, which may be similar to post-LAAC, especially considering there is no evidence that SAPT is effective in preventing DRT. Therefore, patients at high bleeding risk without other indications for SAPT may be able to discontinue antithrombotic therapy early after LAAC. In a global multicenter registry study, 15% of patients stopped all antithrombotic medications within 6 months post-LAAC, and the study results indicated that discontinuing antithrombotic therapy was not associated with an increased risk of DRT or ischemic events but significantly reduced the occurrence of serious bleeding events. The ongoing ASPIRIN-LAAO study will assess the safety of stopping aspirin 6 months post-LAAC.
Future Perspectives: Antithrombotic Treatment Strategy Selection After LAAC
Currently, there is no optimal antithrombotic regimen for preventing DRT and ischemic events post-LAAC. Individualized assessment of bleeding risk should be an important consideration when selecting antithrombotic regimens post-LAAC. Based on previous research results, we propose a strategy for selecting antithrombotic therapy post-LAAC (Figure 1). Based on the patient’s bleeding risk and tolerance to antithrombotic therapy, patients can be categorized into three groups: the first group includes patients without contraindications to OAC (i.e., patients who were on OAC before LAAC), who can receive short-term OAC antithrombotic therapy post-surgery; the second group includes patients who cannot tolerate short-term OAC treatment, primarily due to recent bleeding or high bleeding risk (i.e., patients who were not on OAC before LAAC despite having a risk of stroke related to atrial fibrillation), who can receive short-term DAPT or low-dose DOAC therapy post-surgery; and the third group includes patients with extremely high bleeding risk or active bleeding who cannot tolerate short-term DAPT or low-dose DOAC treatment, who may receive SAPT or no antithrombotic therapy after careful evaluation of expected risks and benefits.
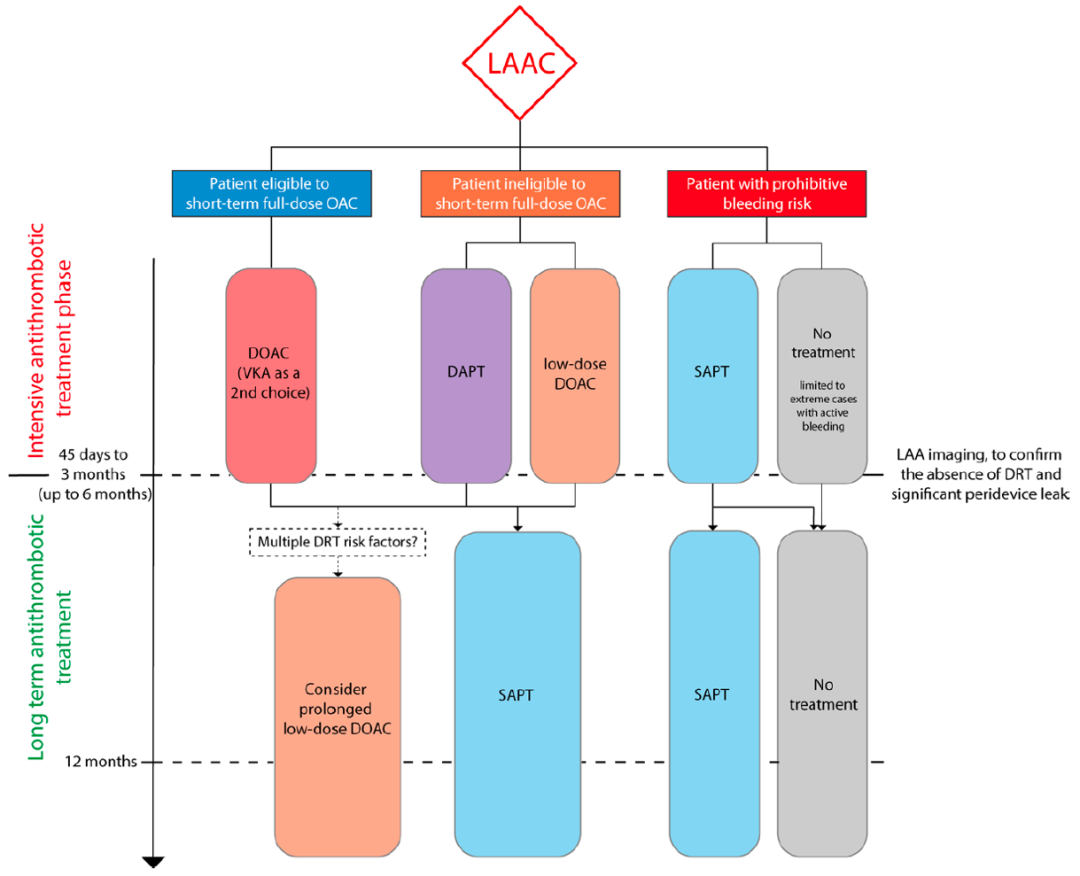
Figure 1 Antithrombotic Treatment Strategy After Left Atrial Appendage Closure (LAAC)
Patients who cannot tolerate short-term oral anticoagulant (OAC) therapy: those with recent bleeding or uncontrollable high bleeding risk (i.e., patients who did not receive OAC therapy before the procedure).
Patients with extremely high bleeding risk: those who cannot tolerate dual antiplatelet therapy (DAPT) or low-dose OAC therapy due to active bleeding or uncontrollable bleeding recurrence risk.
For long-term antithrombotic therapy, SAPT remains the most common regimen, and long-term low-dose DOAC may serve as an alternative for patients at high DRT risk. For patients at high bleeding risk without other indications for antithrombotic therapy, consideration may be given to stopping all antithrombotic treatments.
Conclusion
The choice of medications and treatment duration for antithrombotic therapy post-LAAC remains unclear. The variability in patient types included in related clinical studies (ranging from low to high bleeding risk) has led to uncertainty in the selection of antithrombotic therapy.Although mechanistic studies suggest that OAC may be the optimal choice for early antithrombotic therapy post-LAAC, there remains controversy regarding the efficacy of different antithrombotic strategies in preventing DRT and ischemic events post-LAAC. Therefore, when considering the risk of DRT occurrence, how to avoid serious bleeding may be key in selecting the antithrombotic treatment strategy post-LAAC..
Source:Antithrombotic Management After Left Atrial Appendage Closure: Current Evidence and Future Perspectives. Circ Cardiovasc Interv. 2023;16(5):e012812. doi: 10.1161/CIRCINTERVENTIONS.122.012812.
Recommended Reading
“Kidney” Planning Ahead, Controlling Risks, Early Intervention in CKD is Key to Improving Prognosis in Cardiovascular Disease Patients!
Original Work from Professor Chen Minglong’s Team: In Elderly Patients with Paroxysmal Atrial Fibrillation, Should Ablation of Low-Voltage Areas be Performed After Isolation of the Pulmonary Veins?
Opinion | EHJ: Oral Anticoagulation Therapy for Patients with Rheumatic Heart Disease and Atrial Fibrillation
Case | Management of Spontaneous Coronary Dissection of the Left Main Postpartum
Progress | Circulation Subjournal: ECG Age May Predict the Occurrence of Cardiovascular Events
Progress | Does Loneliness Increase the Risk of CVD in Diabetic Patients?
Progress | BMJ: Can Vitamin D Supplementation Reduce the Incidence of Major Cardiovascular Events in Elderly Patients?
Progress | JACC: What is the Impact of TAVR (SAPIEN 3) on Prognosis in Intermediate-Risk Patients Compared to SAVR?
Progress | JAMA Subjournal: What is the Impact of Coronary Atherosclerotic Plaque Activity on Future Coronary Events?
Progress | EHJ: In Heart Failure with Atrial Fibrillation, a New Score Can Predict Improvement in LVEF after Ablation, Identifying Which Patients Benefit the Most
Progress | Can Rapidly Increasing GDMT Doses Improve Prognosis in Elderly Patients with Acute Heart Failure?
Progress | EHJ: Does a History of Stroke Affect Prognosis Differently in HFrEF and HFpEF Patients?
Progress | EHJ: What is the Impact of Different Plaque Morphologies on Inflammatory Risk and Clinical Prognosis in Acute Coronary Syndrome?
Progress | EHJ: Triglyceride-Rich Lipoprotein Residuals, LDL, and the Risk of Coronary Heart Disease
Progress | Circulation: Is There a Threshold and Inflection Point for LVEF in Heart Failure Patients, and is Current Heart Failure Classification Reasonable?
Progress | In Middle-Aged and Elderly Patients with Left Ventricular Hypertrophy, Is Lowering Systolic Blood Pressure Below 130 mmHg Harmful?

