Liver cancer is currently the 4th most common malignant tumor in China and the 2nd leading cause of cancer-related death.
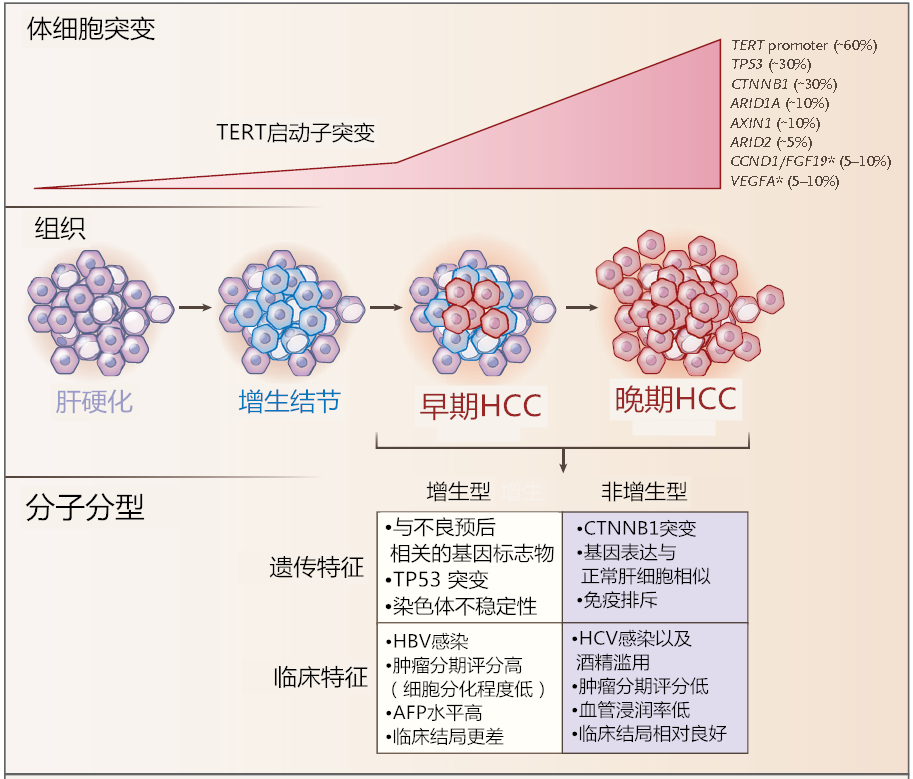
Liver cancer mainly includes three different pathological types: hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and combined hepatocellular carcinoma-cholangiocarcinoma (cHCC-CCA). These types differ significantly in terms of pathogenesis, biological behavior, histopathology, treatment methods, and prognosis, with HCC accounting for 75%-85% and ICC for 10%-15%. Today, we will discuss hepatocellular carcinoma (HCC).
In China, high-risk groups for liver cancer mainly include:
Individuals infected with hepatitis B virus (HBV) and/or hepatitis C virus (HCV), excessive alcohol consumption, non-alcoholic fatty liver disease, cirrhosis caused by other factors, and those with a family history of liver cancer, especially males over 40 years old.
Ultrasound imaging is the most commonly used method for liver imaging in clinical practice due to its convenience, real-time capability, non-invasiveness, and absence of radiation.
Serum AFP is currently an important indicator for diagnosing liver cancer and monitoring treatment efficacy. Serum AFP ≥ 400 μg/L, after excluding pregnancy, chronic or active liver disease, germ cell tumors, and gastrointestinal tumors, highly suggests liver cancer; for those with mildly elevated serum AFP, imaging examinations or dynamic observation should be combined, and compared with changes in liver function to aid in diagnosis.
Pathological Diagnosis of Liver Cancer
Primary liver cancer refers to malignant tumors originating from hepatocytes and intrahepatic cholangiocytes, mainly including HCC, ICC, and cHCC-CCA.
(1) HCC: Refers to malignant tumors occurring in hepatocytes. The pathological diagnostic terms “hepatocellular liver cancer” or “hepatocellular carcinoma” are not recommended.
(2) ICC: Refers to malignant tumors arising from the epithelial cells covering the branches of the intrahepatic bile ducts, with adenocarcinoma being the most common. Histologically, it can be divided into:
① Large duct type: Originates from larger bile ducts above the portal area between the hepatic lobule septa, with large and irregular duct diameters;
② Small duct type: Originates from small bile ducts or fine bile ducts below the hepatic lobule septa, with smaller and more regular duct diameters, or may appear as solid small strands with closed lumens.
Studies have shown that the biological behavior and genetic phenotype characteristics of these two subtypes of ICC differ, with patients having small duct type showing better clinical prognosis than those with large duct type.
(3) cHCC-CCA: Refers to the simultaneous presence of HCC and ICC components within the same tumor nodule, excluding collision tumors.
Immunohistochemical Examination of Liver Cancer
The main purposes of immunohistochemical examination of liver cancer are: ① to differentiate between benign and malignant tumors of hepatocytes; ② to differentiate between HCC and ICC as well as other special types of liver tumors; ③ to distinguish primary liver cancer from metastatic liver cancer. Due to the high heterogeneity of liver cancer histological types, existing liver cancer cell protein markers have certain limitations in diagnostic specificity and sensitivity, often requiring reasonable combinations and objective assessments, and sometimes needing to be used in conjunction with markers from other systemic tumors.
(1) HCC:
The following markers are positive for hepatocyte labeling, which helps indicate tumors of hepatocyte origin but cannot be used as the basis for distinguishing between benign and malignant hepatocyte tumors.
① Arginase-1: Cytoplasmic/nuclear staining in hepatocytes.
② Hepatocyte antigen: Cytoplasmic staining in hepatocytes.
③ Antibodies specific for canalicular membrane proteins: Such as CD10, polyclonal carcinoembryonic antigen, and bile salt export pump proteins, which can show specific staining at the canalicular membrane of hepatocytes, aiding in confirming hepatocyte tumors.
The following markers help differentiate between benign and malignant hepatocyte tumors.
① Phosphatidylinositol protein-3: Cytoplasmic and membrane staining in hepatocellular carcinoma cells.
② CD34: Although CD34 immunohistochemical staining does not directly label parenchymal liver cells, it can display the microvascular density and distribution patterns of different types of liver tumors: for example, hepatocellular carcinoma shows a diffuse pattern, cholangiocarcinoma shows a sparse pattern, hepatocellular adenoma shows a patchy pattern, and focal nodular hyperplasia shows a cord-like pattern, which, when combined with tumor histological morphology, aids in differential diagnosis.
③ Heat shock protein 70: Cytoplasmic or nuclear staining in hepatocellular carcinoma cells.
④ Glutamine synthetase: Often shows diffuse strong positivity in hepatocellular carcinoma; some hepatocellular adenomas, especially those with β-catenin mutation activation, may also show diffuse positivity; in HGDN, moderate intensity focal staining is seen, with positive cells < 50%; in focal nodular hyperplasia, it shows characteristic irregular map-like staining; in normal liver tissue, only hepatocytes around the central veins are stained, and these characteristics aid in differential diagnosis.
(2) ICC:
① Epithelial cell surface glycoprotein (MOC31): Membrane staining in cholangiocarcinoma cells.
② Cytokeratin (CK) 7/CK19: Cytoplasmic staining in cholangiocarcinoma cells.
③ Mucin-1 (muc-1): Membrane staining in cholangiocarcinoma cells. Although these markers are positive, indicating tumors of cholangiocyte origin, they may also be positively expressed in non-tumorous cholangiocytes, requiring careful differentiation.
(3) cHCC-CCA:
HCC and ICC components express the respective markers of their tumors. Additionally, positive expressions of markers such as CD56, CD117, and epithelial cell adhesion molecule (EpCAM) may suggest tumor characteristics associated with stem cell differentiation, indicating greater invasiveness.
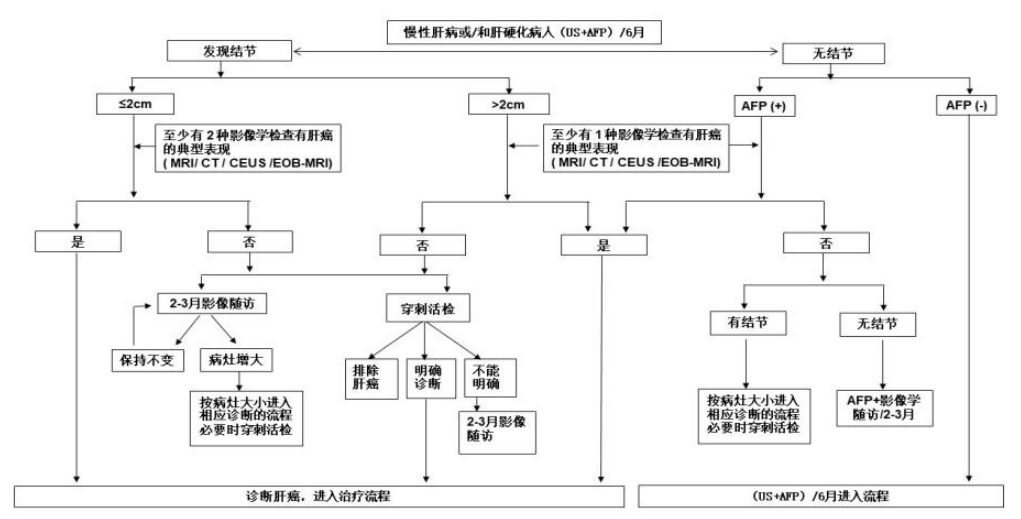
Diagnosis Flowchart for Liver Cancer
Staging of Liver Cancer
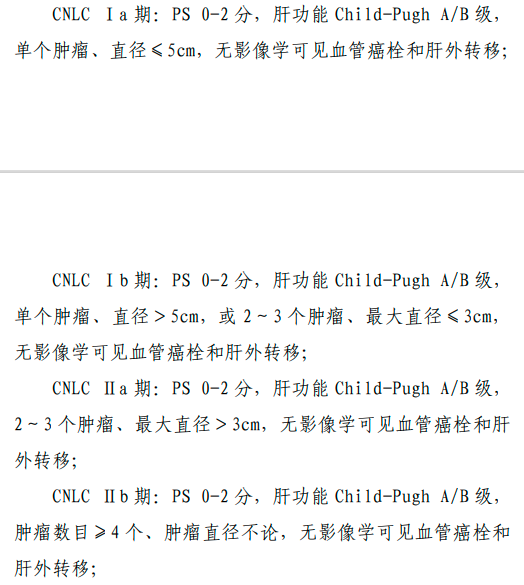
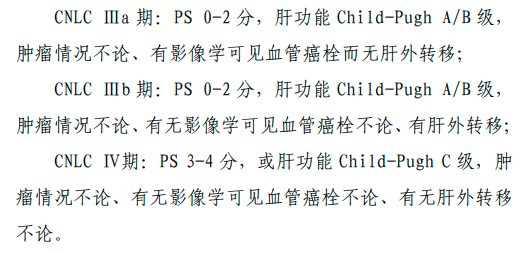
The staging of liver cancer is crucial for selecting treatment options and evaluating prognosis. Various staging systems exist internationally, such as BCLC, TNM, JSH, and APASL. Considering China’s specific national conditions and practical experience, a staging system for liver cancer in China (China liver cancer staging, CNLC) has been established based on patients’ performance status (PS), liver tumor, and liver function, including: CNLC stage I-a, I-b, II-a, II-b, III-a, III-b, and IV, with specific staging scheme descriptions in Figure 3.
Clinical Staging and Treatment Flowchart for Liver Cancer in China
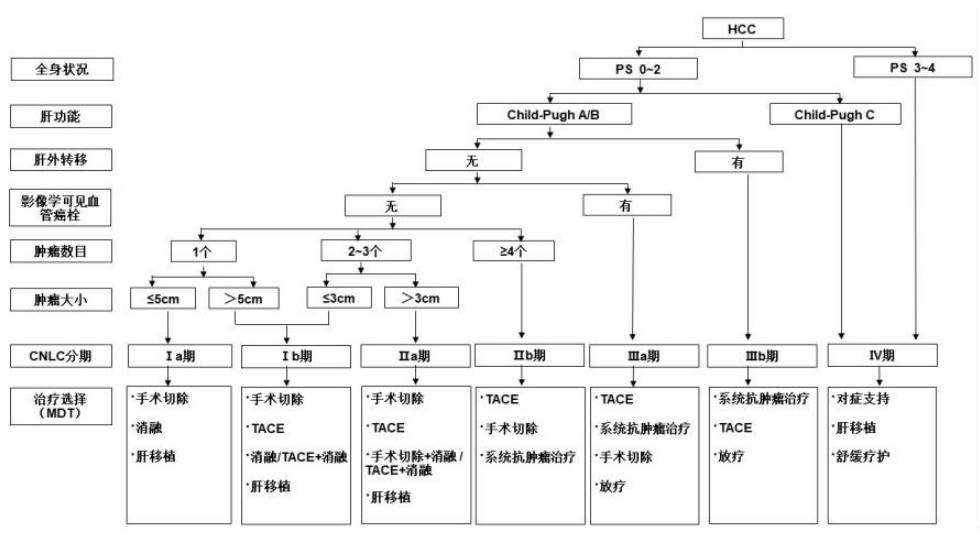
Note: Systemic anti-tumor treatments include:
First-line treatments:
Atezolizumab + Bevacizumab, Sintilimab + Bevacizumab similar agents;
Doravirine, Lenvatinib, Sorafenib;
FOLFOX4;
Second-line treatments:
Regorafenib, Apatinib, Carrelizumab, Tislelizumab
Copyright Statement
This public account is purely for public welfare, and we focus on sharing. The content and images of the articles may come from the internet, and the copyright belongs to the original authors. If there are any objections, please contact us for timely deletion!
Leave a message on the platform

Postscript: Many friends have not developed the habit of liking. If you think this is well written, please give a thumbs up at the bottom ♡ as encouragement! Persistence is a belief, and focus is an attitude!