As modern medicine gradually increases its understanding of sleep disorders, polysomnography has become increasingly widely used across various clinical departments including neurology, respiratory medicine, otolaryngology, dentistry, and psychiatry.As an important tool for clinical practice and research in sleep medicine, the value of polysomnography is increasingly recognized. In order to further clarify the clinical indications for polysomnography in China, standardize operating procedures, and unify diagnostic terminology and reporting formats, the Sleep Disorders Professional Committee of the Neurology Branch of the Chinese Medical Association, in collaboration with the Sleep Disorders Professional Committee of the Chinese Sleep Research Society and the Sleep Disorders Group of the Neurology Branch of the Chinese Medical Association, invited relevant experts from mainland China and Hong Kong to form the “Expert Committee on Polysomnography Operation Specifications and Clinical Applications in Adults” to conduct in-depth discussions. They appropriately referenced foreign guidelines and, based on extensive consultations, jointly drafted the “Expert Consensus on Polysomnography Operation Specifications and Clinical Applications in Adults”.
1. Overview
Polysomnography (PSG) is a diagnostic technique that continuously synchronizes the collection, recording, and analysis of multiple physiological parameters and pathological events during sleep using a polysomnograph in a sleep monitoring room.The parameters collected and recorded by polysomnography include electroencephalogram (EEG), electrooculogram (EOG), electromyogram (EMG), electrocardiogram (ECG), airflow, snoring, respiratory movement, oxygen saturation, body position, etc. Additional parameters such as audiovisual monitoring, esophageal pressure, esophageal pH, transcutaneous or end-expiratory carbon dioxide pressure, and erectile function can also be added.These parameters are displayed in the form of curves, numbers, images, and audiovisual data, forming interpretable and analyzable information, known as a polysomnogram (PSG).Polysomnography is a commonly used objective examination for analyzing sleep structure and assessing sleep disorders, serving as a fundamental tool for clinical practice and research in sleep medicine.
(1) Indications for Polysomnography
1. Sleep-Related Breathing Disorders:(1) Diagnosis of patients with sleep-disordered breathing (SDB), identifying the types of sleep apnea and hypoventilation events (obstructive/central/mixed) and classifying the sleep-related breathing disorders (obstructive/central), assessing severity, and differentiating from other sleep disorders; clarifying sleep-related hypoventilation and hypoxemia disorders; (2) Evaluating the effectiveness of various treatment methods for sleep-disordered breathing; (3) Re-examination of patients highly suspected of sleep-disordered breathing but with negative results from home sleep apnea monitoring or initial polysomnography; (4) Reassessing treatment for patients receiving non-invasive positive pressure ventilation who experience weight changes, poor clinical outcomes, or recurrent symptoms; (5) Performing manual pressure titration before non-invasive positive pressure ventilation; (6) Other clinical symptoms and signs suggesting possible sleep-related breathing disorders, such as excessive daytime sleepiness unexplained by primary diseases, daytime hypoxemia, polycythemia, refractory hypertension, unexplained arrhythmias, nocturnal angina, dry mouth upon awakening, or persistent chronic cough.
2. Excessive Daytime Sleepiness Disorders:(1) Diagnosis, differential diagnosis, and treatment effectiveness evaluation of narcolepsy; (2) Diagnosis and differential diagnosis of idiopathic hypersomnia; (3) Polysomnography should be conducted the night before multiple sleep latency testing (MSLT).
3. Parasomnias, Sleep-Related Epilepsy, and Other Nocturnal Events: Clarifying the types of nocturnal events such as parasomnias, sleep-related epilepsy, and movement disorders. Especially for patients with atypical clinical symptoms, unclear treatment effects, or those causing harm to themselves or others, polysomnography is required.
4. Sleep-Related Movement Disorders: Diagnosis and assessment of periodic limb movement disorder and differentiation from restless legs syndrome and REM sleep behavior disorder.
5. Insomnia: Mainly used for clinical assessment of insomnia patients with atypical symptoms or poor treatment outcomes. To clarify whether there is subjective insomnia and to differentiate whether other sleep disorders affecting sleep, such as sleep-related breathing disorders, periodic limb movement disorder, or parasomnias, are present.
6. Circadian Rhythm Sleep-Wake Disorders: Clarifying the patient’s sleep structure and excluding other sleep disorders. It is recommended to use portable sleep monitoring technologies such as actigraphy to observe circadian rhythm changes.
7. Sleep Disorders Related to Mental Illness:(1) Evaluation of treatment effectiveness for sleep disorders related to mental illness; (2) Excluding sleep-related breathing disorders, restless legs syndrome, and other sleep disorders, as well as drug-related sleep disorders.
(2) Basic Principles and Recommendations for Polysomnography
1. When performing polysomnography, it is important to consider that different individuals may have significant differences in sleep habits, selecting appropriate start and end times for recording based on the patient’s daily routine. The clinical value of interpreting polysomnography reports should also be combined with the patient’s age and underlying diseases for individualized diagnostic analysis. Additionally, necessary specialized examinations should be conducted for patients based on the corresponding clinical examination needs of different departments.
2. The latest version of the “AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications” is recommended for interpreting sleep stages and related events.
2. Examination Methods and Procedures
(1) Content of Polysomnography Records and Electrode Placement
Polysomnography typically records bioelectric signals such as EEG, EOG, EMG, and ECG; physiological signals such as airflow, chest and abdominal movements, pulse oximetry, and snoring; and external signals such as transcutaneous carbon dioxide and pressure titration-related parameters.
1. EEG electrodes should be placed according to the international “10-20” system naming standards.It is recommended to use the combinations C4-M1, F4-M1, O2-M1 for recording; backup leads should use C3-M2, F3-M2, O1-M2; acceptable leads include FZ-CZ, CZ-OZ, C4-M1.It is recommended to place the ground electrode at the Fpz position and its vicinity, and the reference electrode at the Cz position. If any electrodes malfunction during monitoring, backup electrodes should be placed at Fpz, C3, O1, and M2; it is acceptable to use Fpz instead of Fz, C3 instead of Cz or C4, O1 instead of Oz, and M2 instead of M1.
2. The EOG electrodes E1 and E2 should be placed 1 cm outward and downward from the outer canthus of the left eye and 1 cm outward and upward from the outer canthus of the right eye, respectively.EOG leads are recommended to use E1-M2/E2-M2 for recording.
3. The electrodes for detecting the chin EMG should be placed 2 cm below the anterior border of the mandible, 2 cm to the left of the midline for the Chin1 electrode, and 2 cm to the right of the midline for the Chin2 electrode. The reference electrode ChinZ should be placed 1 cm above the midline of the anterior border of the mandible.Recommended leads are Chin1-ChinZ or Chin2-ChinZ.
4. Monitoring of airflow: It is recommended to use both oral-nasal temperature sensors and nasal pressure sensors to monitor airflow. Oral-nasal temperature sensors are typically placed above the nostrils and the upper lip.
5. Monitoring of respiratory effort: It is recommended to use respiratory inductance plethysmography belts to monitor respiratory effort. The chest belt should be placed at the level of the nipples, and the abdominal belt should be placed at the level of the navel. Intercostal/diaphragmatic EMG and esophageal pressure measurements can also be used for recording.
6. Monitoring of pulse oximetry: Typically, fingertip or earlobe sensors are used to continuously record pulse oxygen saturation to assess the degree and frequency of oxygen desaturation. The adult pulse oximeter probe should be placed on the tip of the ring finger and securely fixed.
7. Cardiac monitoring: Typically, single-lead ECG monitoring is used.The modified lead II electrode placement method is recommended: the negative electrode is placed at the intersection of the right subclavian line and the extended line of the right lower limb, and the positive electrode is placed at the intersection of the 6th and 7th intercostal spaces with the extended line of the left lower limb. This is mainly used to assess heart rate and arrhythmias.
8. Monitoring of limb movements: Electrodes are typically placed on the midsection of the anterior tibialis muscle of both lower limbs, with a distance of 2-3 cm between the two electrodes. Depending on clinical examination needs, upper limb movements can also be monitored simultaneously, in which case the electrodes should be placed on the midsection of the extensor or flexor muscles of both arms, with a distance of 2-3 cm between the two electrodes.
9. Video-audio recording: Video and audio recordings should be synchronized with EEG, EOG, EMG, and other signals to confirm the patient’s position, abnormal behaviors, and vocalizations during sleep. Audio can also assist in diagnosing bruxism, sleep talking, snoring, moaning, etc. The snoring sensor should be placed at an appropriate position on the neck to capture the maximum signal.
10. Position recording: A three-dimensional accelerometer to record position changes is usually placed near the midline of the chest, close to the xiphoid process, and can display various positions such as supine, prone, left lateral, right lateral, and upright.
11. Other auxiliary monitoring content:: Depending on different clinical examination needs, corresponding monitoring modules may be added. For patients with sleep-related breathing disorders, additional monitoring of end-expiratory carbon dioxide pressure and transcutaneous carbon dioxide pressure may be included. For patients with parasomnias or epilepsy, it is recommended to conduct continuous video EEG monitoring and increase the number of EEG recording electrodes, with a 10-second window used for analysis. For patients with gastroesophageal reflux disease, esophageal pH measurement may be performed simultaneously for diagnosis and treatment evaluation. For patients with erectile dysfunction, measuring the tension in the cingulate can reflect whether penile erection occurs, its intensity, and the sleep phase.
(2) Technical and Data Specifications for Polysomnography
1. Detect and record electrode impedance: Electrode impedance should be detected and recorded before the start and end of PSG recording. The electrode impedance for EEG, EOG, and chin EMG should be ≤5kΩ, and the lower limb EMG electrode impedance should ideally be ≤5kΩ, ≤10kΩ is acceptable. If artifacts occur, the electrode impedance should be rechecked.
2. Minimum digital resolution should be 12 bits.
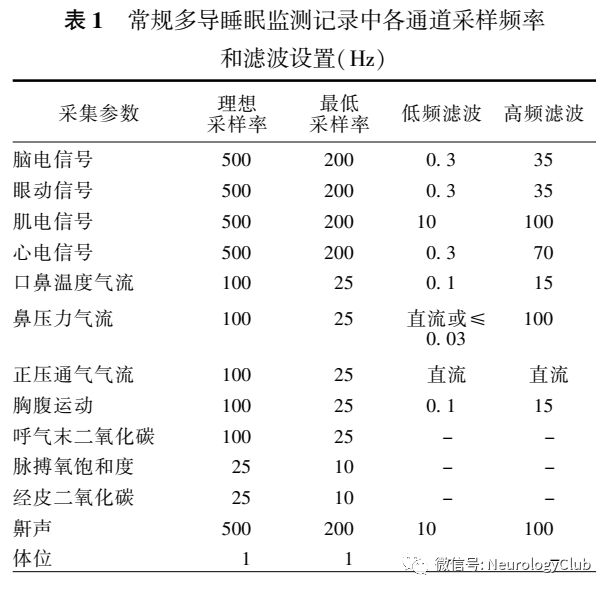
3. Sampling frequency and filtering: Sampling frequency and filtering settings for each channel should follow the recommendations in the “AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications” (Table 1).
(3) Procedures for Polysomnography
1. Mechanical calibration: Before monitoring, the sensitivity, polarity, and filtering settings of each amplifier should be calibrated; appropriate signal sampling frequencies should be selected for different leads; and the display should be set to an appropriate resolution. Currently, digital PSG does not require mechanical calibration for each monitoring session, only periodic calibration is necessary.
2. Electrode placement: After accurately measuring and locating according to the aforementioned electrode placement requirements, the electrodes should be sequentially adhered and placed.
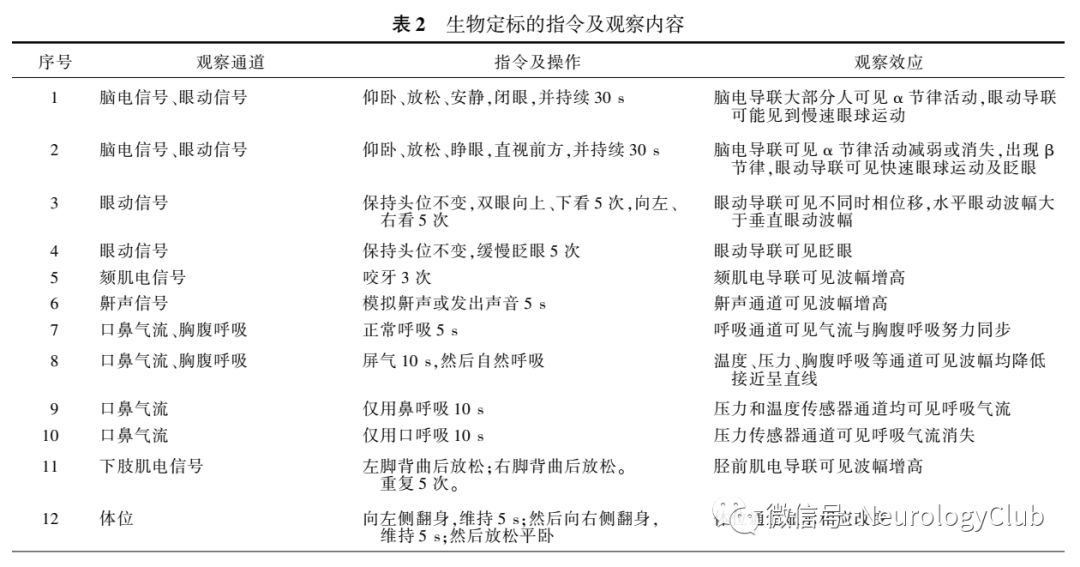
3. Biological calibration: Standardized biological calibration is a necessary part of every sleep monitoring session.Signals collected by observing the monitored individual making corresponding movements according to instructions can record basic physiological parameters such as alpha rhythm in EEG recordings and amplitude of tibialis anterior muscle activity, and confirm whether the electrode placement is accurate, and whether the monitoring equipment, sensors, and electrodes are functioning normally. These instructed movements include closing eyes, opening eyes, moving eyes up, down, left, and right, inhaling, exhaling, holding breath, and moving toes (Table 2). Biological calibration should occur before and after monitoring.
4. After obtaining a stable signal, monitoring should commence.During monitoring, attention should be paid to observing the patient’s abnormal behaviors, movements, and events, promptly identifying and correcting any potential signal artifacts, and regularly checking impedance.
5. When the patient requests to get up or end the recording, monitoring should be paused or terminated.
6. Analyze the examination results, issue a signed report, and have the doctor responsible for the sleep examination review and sign.
3. Basis and Basic Rules for Sleep Staging
(1) Basis for Sleep Staging
Polysomnography primarily relies on information recorded from EEG, EOG, and chin EMG to comprehensively assess wakefulness and various sleep stages.
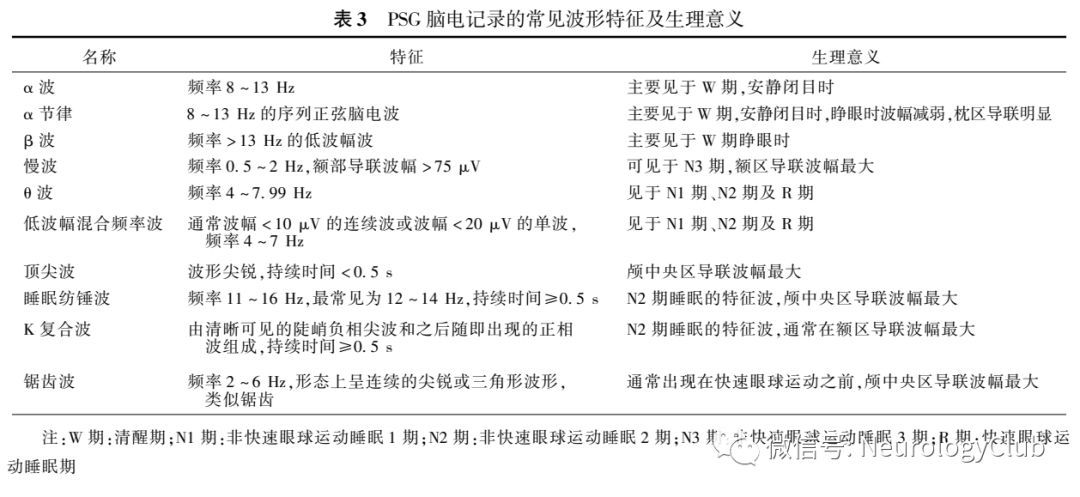
1. Common waveforms recorded in EEG: Identifying EEG waveforms is a crucial basis for sleep staging.In addition to common waveforms like alpha waves, beta waves, and delta waves seen in routine EEG monitoring, there are also unique EEG waveforms that serve as primary references for identifying the corresponding sleep stages, including alpha rhythms, low-amplitude mixed frequency waves, vertex waves, sleep spindles, K-complexes, slow waves, and sawtooth waves(Table 3).
2. Common waveforms recorded in EOG: (1) Blinks:Conjugate vertical eye movements with a frequency of 0.5-2.0Hz that occur when blinking with eyes open. (2) Reading eye movements:Conjugate eye movements composed of slow eye movements followed by rapid eye movements that occur when reading text. (3) Rapid eye movements (REM):Conjugate, irregular, steep waveforms with a peak time of less than 500ms. Rapid eye movements are characteristic of REM sleep and can also be seen during wakefulness when scanning the environment with eyes open. (4) Slow eye movements (SEM):Conjugate, relatively regular sine waveforms, with a peak time typically greater than 500ms.
3. Common waveforms recorded in chin EMG:: The amplitude of chin EMG is typically higher during wakefulness than during sleep. Upon entering sleep, the amplitude of chin EMG gradually decreases from N1 to N3, and it may already be at a low level in N1, with the lowest level during REM sleep.
(2) Basic Rules for Sleep Staging
1. Basic units of sleep staging:: A continuous 30-second PSG recording is referred to as one epoch. An epoch is the smallest unit of sleep staging, and each epoch should be marked as a specific sleep stage. When two or more sleep stage characteristics appear within one epoch, the dominant (most prevalent) sleep stage should be used as the label for that epoch.
2. Marking of sleep stages:: The normal sleep structure is divided into three parts: non-rapid eye movement sleep (NREM), rapid eye movement sleep (REM), and wakefulness, with NREM further divided into N1, N2, and N3 stages. (1) W stage:The EEG during wakefulness can show low-amplitude mixed waveforms (beta and alpha waves), and when eyes are closed, alpha rhythms can be recorded in the occipital region, occupying more than 50% of the epoch.The EOG during wakefulness may show reading eye movements, rapid eye movements, and blinks, while slow eye movements can be recorded with eyes closed. The amplitude of chin EMG varies but is generally higher than during sleep. (2) N1 stage:The EEG features low-amplitude mixed frequency waves, occupying more than 50% of the epoch, and may show vertex waves.The EOG may show slow eye movements.The amplitude of chin EMG varies, usually lower than during wakefulness. (3) N2 stage:The EEG features sleep spindles and K-complexes.The EOG typically shows no significant eye movements, and slow eye movements may occasionally be observed.The amplitude of chin EMG varies, usually lower than during wakefulness. (4) N3 stage:The slow waves in the EEG should occupy at least 20% of the epoch.The EOG typically shows no eye movements.The amplitude of chin EMG varies, usually lower than in N2, and may approach the level during REM sleep. (5) REM stage:The EEG may show low-amplitude mixed frequency waves, and sawtooth waves may also occur.The EOG shows rapid eye movements.The amplitude of chin EMG is significantly reduced, usually at the lowest level throughout the recording.
3. Other conditions for sleep staging:: (1) Major body movements (MBM):Due to body movements and EMG artifacts interfering with the EEG for more than 50% of an epoch, accurate sleep staging cannot be determined. (2) Arousal:A sudden change in EEG frequency during sleep leads to a transient interruption of sleep continuity, but does not necessarily manifest as wakefulness. In interpreting arousal during NREM sleep, it is necessary to observe a sudden change in EEG frequency, with the appearance of alpha waves, theta waves, or waves with a frequency greater than 16Hz, lasting at least 3 seconds, preceded by at least 10 seconds of stable sleep. In interpreting arousal during REM sleep, it is required that while meeting the criteria for EEG frequency change, there should also be observed increased EMG activity in the chin EMG recording lasting over 1 second.
4. Abnormal Events During Sleep Stages
(1) Respiratory-Related Events
1. Apnea: The amplitude of the airflow signal from the oral-nasal temperature sensor channel decreases by ≥90% compared to baseline, and the event lasts for ≥10 seconds. Based on the presence or absence of respiratory effort during the period of airflow cessation, it is further divided into: (1) Obstructive apnea:Respiratory effort persists or increases during the period of airflow cessation; (2) Central apnea:Respiratory effort ceases during the period of airflow cessation; (3) Mixed apnea:During the initial part of the event, respiratory effort ceases, followed by a restoration of respiratory effort.
2. Decreased pulse oxygen saturation: Typically defined as an event where the pulse oxygen saturation decreases by ≥3% compared to before the respiratory event.
3. Hypoventilation: The amplitude of the nasal pressure channel airflow signal decreases by ≥30% compared to baseline, the event lasts for ≥10 seconds, and is accompanied by a decrease in pulse oxygen saturation of ≥3% or arousal.
4. Respiratory effort-related arousal (RERA): A respiratory event lasting ≥10 seconds characterized by increased respiratory effort or flattened nasal pressure waveform, leading to arousal during sleep, but does not meet the criteria for apnea or hypoventilation.
(2) Cardiac-Related Events
1. Sinus Tachycardia: During sleep, sinus rhythm with a heart rate of ≥90 beats/min, lasting more than 30 seconds.
2. Sinus Bradycardia: During sleep, sinus rhythm with a heart rate of ≤40 beats/min, lasting more than 30 seconds.
3. Cardiac Arrest: Cardiac arrest lasting ≥3 seconds.
4. Wide Complex Tachycardia: At least three consecutive heartbeats with wide QRS complex waveforms, duration ≥120ms, heart rate >100 beats/min.
5. Narrow Complex Tachycardia: At least three consecutive heartbeats with QRS complex duration <120ms, heart rate >100 beats/min.
6. Atrial Fibrillation: Irregular heart rhythm, with normal P waves replaced by rapid fibrillation waves of varying size, shape, and duration.
(3) Abnormal Limb Movement Events
1. Significant Limb Movement: Lasting 0.5-10 seconds, with EMG amplitude increased by >8μV compared to resting state, where the duration starts from the point of EMG amplitude increase and ends when the amplitude rises no more than 2μV compared to resting state.
2. Periodic Limb Movement: Four or more consecutive limb movements, with an interval of 5-90 seconds between the starting points of two consecutive limb movements.
3. Periodic Limb Movement During Sleep (PLMS): Periodic limb movements that occur during sleep.
4. Muscle Activity During REM Sleep: In one epoch of REM sleep, the chin EMG activity exceeds the minimum amplitude of non-REM sleep for more than 50% of the time.
5. Paroxysmal Muscle Activity During REM Sleep: In one epoch of REM sleep, subdivided into 3-second mini epochs, with 5 mini epochs showing paroxysmal muscle activity lasting 0.1-5.0 seconds, with amplitude increased ≥4 times compared to baseline EMG amplitude.
5. Content and Format of the Report
(1) Routine Report Content for Polysomnography
1. General Information of the Patient:: Including name, gender, contact information, height, weight, blood pressure, body mass index (BMI), neck circumference, waist circumference, etc.
2. General Information of the Examination:: Including examination date, purpose, electrode placement method, recorded parameters, basis for sleep staging and related events interpretation, signatures of polysomnography analysis technician and physician, etc.
3. Sleep Structure Parameters:: (1) Light Out Time (hh:mm): The starting time of sleep monitoring. The time when the lights are turned off and the patient is instructed to begin sleeping, which should generally align with the patient’s usual bedtime. (2) Light On Time (hh:mm): The termination time of sleep monitoring. The time when the patient is awake and indicates no longer sleeping. (3) Total Recording Time (TRT) (minutes): The total duration of sleep recording from light out to light on. (4) Sleep Latency (SL) (minutes): The time from light out to the first frame of sleep. (5) Total Sleep Time (TST) (minutes): The total actual sleep time from light out to light on, which is the sum of the durations of all sleep stages (N1, N2, N3, R). (6) Wake After Sleep Onset (WASO) (minutes): The total time of all awakenings from the first frame of sleep to the end of the recording. (7) REM Latency (minutes): The time from the first frame of sleep to the first frame of REM sleep. (8) Sleep Efficiency (SE) (%): Total sleep time/total recording time × 100%. (9) Wake Time (W) (minutes): The total time of all awakenings during the recording, including sleep latency and wake time after sleep onset. (10) Duration of Each Sleep Stage (minutes): The cumulative time for each sleep stage (N1, N2, N3, R). (11) Proportion of Each Sleep Stage (%): The percentage of cumulative time for each sleep stage (N1, N2, N3, R) relative to total sleep time. (12) Number of Awakenings (times): The total number of awakenings during sleep. (13) Arousal Index (ArI) (times/hour): The number of awakenings per unit sleep time, i.e., the number of awakenings/total sleep time.
4. EEG Recordings:: Describe baseline brain waves, whether abnormal brain activity exists, etc. If abnormal brain activity is detected during monitoring, it should describe the sleep stage, whether symptoms of abnormal episodes were observed, duration, and whether there were changes in autonomic functions such as heart rate and respiration.
5. Respiratory-Related Event Parameters:: (1) Number of Sleep-Related Breathing Events (times): The total number of apneas, hypoventilation, and RERA events during sleep. (2) Number of Apneas and Hypoventilation (times): The total number of apneas and hypoventilation events during sleep. (3) Number of Apneas (times): The total number of apneas during sleep, further divided into obstructive, central, and mixed apneas. (4) Number of Hypoventilation Events (times): The total number of hypoventilation events during sleep. (5) Sleep-Related Breathing Event Index (times/hour): The number of breathing events per unit sleep time, i.e., the number of apneas, hypoventilation, and RERA events/total sleep time. (6) Longest Duration of Apnea and Hypoventilation. (7) Oxygen Desaturation Index (ODI) (times/hour): The number of desaturation events per unit sleep time, i.e., the number of desaturation events/total sleep time. (8) Average and Minimum Oxygen Saturation. (9) Cumulative Time Below 88% or 90% Oxygen Saturation.
6. Cardiac-Related Event Parameters:: Changes in heart rate during wakefulness and sleep (maximum heart rate, minimum heart rate, average heart rate), whether arrhythmia events exist, etc. If tachycardia is present, the maximum heart rate during the event should be described; if bradycardia is present, the minimum heart rate during the event should be described; if cardiac arrest occurs, the longest duration of arrest should be described; if atrial fibrillation is present, the average heart rate should be described.
7. Abnormal Limb Movement Events:: (1) Number and Index of Periodic Limb Movements During Sleep: (2) Number and Index of Arousal-Related Periodic Limb Movements:
8. Trend Graphs:: Display the sleep stages, awakenings, breathing events, pulse oxygen saturation, and limb movement events during different monitoring periods in a structured format.
9. Description of the Examination Process by the On-Duty Technician and Analysis Technician:: Including the patient’s cooperation during the examination, any abnormal activities observed at night, related interventions, changes in the examination environment and equipment status, the quality of the polysomnography, and any special polysomnography presentations.
10. Diagnostic Summary:: Describe the overall sleep situation (sleep time, sleep structure), sleep-related breathing events and severity, and any abnormal behaviors or limb movement events during sleep.
(2) Safety and Precautions for Polysomnography:The physician in the sleep monitoring room should arrange for medical staff to monitor throughout the night based on the examination purpose and specific patient condition assessment, and obtain informed consent from special patients as necessary, requesting family accompaniment. Emergency plans should be developed for potential unexpected situations that may arise during monitoring, and sleep physicians and technicians should enhance personnel training to be capable of independently handling emergencies.The sleep monitoring room should have a relatively independent space, ensuring a quiet, dark, and comfortable sleep environment, with controllable room temperature, equipped with basic emergency equipment and protective devices.