
HCV infection is one of the most common causes of chronic liver disease, potentially leading to liver failure, cirrhosis, and liver cancer, representing a significant global public health issue. According to estimates by the World Health Organization, in 2015, there were 71 million people globally with chronic HCV infection, and 399,000 died from cirrhosis or hepatocellular carcinoma caused by HCV infection. The previous standard treatment was pegylated interferon (PEG-IFN) combined with ribavirin (RBV) (PR regimen), but with the advent of direct antiviral agents (DAA), the traditional PR regimen has gradually been replaced by DAA. Currently, DAA is the recommended medication for treating HCV infection, achieving over 90% sustained virologic response (SVR) in patients with known major genotypes and subtypes of HCV infection. However, a small number of HCV-infected patients experience DAA treatment failure, including virologic breakthrough and relapse. This study selected patients who failed DAA treatment, defined as patients who had undetectable HCV RNA at the end of treatment but tested positive for HCV RNA post-treatment. We aimed to analyze the factors affecting DAA treatment failure in hepatitis C by comparing baseline clinical data and genetic sequencing with successful HCV-infected patients.
1 Materials and Methods
1.1 Study Subjects
We selected 13 patients with chronic hepatitis C (CHC) who failed initial DAA treatment from multiple centers between November 2019 and October 2021 for the treatment failure group. All patients had completed a full 12-week course of DAA treatment and were HCV RNA negative at the end of treatment, but tested HCV RNA positive after treatment. The treatment start dates for patients ranged from November 2017 to July 2021, and the serum HCV RNA relapse dates ranged from March 2018 to January 2022. We selected 51 CHC patients who successfully received DAA treatment from December 2017 to May 2020 at the Infectious Diseases Department of Peking University First Hospital as the control group, all of whom were treatment-naive patients. All patients’ CHC diagnoses met the criteria of the “Guidelines for the Prevention and Treatment of Hepatitis C (2019 Edition)” in China. Exclusion criteria: (1) Patients with significant missing clinical data; (2) Patients whose post-treatment HCV RNA positive serum samples were not collected or whose serum samples showed significant hemolysis or contamination; (3) Patients with other viral infections, such as HBV, HIV, etc.
1.2 Observational Indicators
We collected all clinical data from patients, including gender, age, pre-treatment genotype (using PCR sequencing method), medications and duration of treatment failure, blood sampling dates at treatment failure, serum HCV RNA quantification, and some common blood and biochemical indicators, and performed comparative and statistical analysis of baseline data between treatment failure and treatment success patients. We collected serum samples from treatment failure patients with HCV RNA relapse and baseline serum samples from treatment success patients for HCV RNA extraction, reverse transcription, and PCR amplification of three segments: NS3/NS5A/NS5B, followed by Sanger sequencing to obtain peak charts.
1.3 Experimental Design
According to the instructions of the QIAamp Viral RNA Mini Kit (Germany, Qiagen), we extracted viral RNA from patients’ serum. The RevertAid First Strand cDNA Synthesis Kit (USA, ThermoFisher) was used for reverse transcription PCR of RNA, with all operations performed using disposable consumables and on ice. Primers were designed based on previous literature and synthesized by Beijing Liuhe Huada Gene Technology Co., Ltd. The obtained cDNA was subjected to nested PCR amplification, and the amplification products were identified by electrophoresis on a 1% agarose gel. Positive amplification products were sent to Beijing Liuhe Huada Gene Technology Co., Ltd. for Sanger sequencing, using AJ238799.1 as the reference sequence, and the sequence information was analyzed using Vector NTI Suite 9.0 software, and submitted to the HCV resistance database (hcv.bioinf.mpi-inf.mpg.de/index.php) for analysis.
2 Results
2.1 General Information
A total of 13 patients were included in the DAA treatment failure group, of which only 1 patient had concomitant chronic kidney disease (CKD) stage 3, while the others had no concomitant diseases. Among the 13 patients, 12 had complete treatment course data, all relapsed within one year post-treatment, with 3 relapsing within one month, 2 within two months, 2 within three months, 2 within six months, and 3 within twelve months. Among the 5 male patients, 4 relapsed within three months, and 1 relapsed after three months; among the 7 female patients, 3 relapsed within three months, and 4 relapsed after three months. The HCV RNA positivity within three months was not related to the patient’s gender (P=0.198).
We collected genotype data from 12 patients, of which 5 were type 1b, 3 were type 2a, and 4 were type 3b. All 3b type patients failed treatment with the combination of sofosbuvir and velpatasvir (SOF/VEL), while 1 of the 2a type patients failed treatment with sofosbuvir alone, and 2 failed treatment with sofosbuvir combined with ribavirin (RBV). Among the 1b type patients, there was 1 case of treatment failure with sofosbuvir, 1 with elbasvir and grazoprevir (EBR/GZR), and 2 with the combination of daclatasvir (DAC) and asunaprevir (ASV). Treatment failure in 3b or 2a type patients may be closely related to the use of sofosbuvir, whereas treatment failure in 1b type patients may be due to various treatment regimens. Furthermore, statistical analysis showed that baseline TBil, DBil, and Cr levels in male treatment failure patients were generally higher than those in females (P values <0.05).
2.2 Comparison of Clinical Data Between the Two Groups
We compared the baseline clinical data of hepatitis C patients in the treatment failure group and the control group, finding statistically significant differences in age and genotype between the two groups (P values <0.05). Including these factors in a logistic regression model showed that patients aged 55 years or younger and those with genotype 3b had an increased risk of DAA treatment failure (P values <0.05).
2.3 Genetic Sequencing Results and Comparison of Treatment Failure Patients
We obtained gene sequences for NS3, NS5A, and NS5B regions from 3, 5, and 5 patients, respectively, with their RAS distribution shown in Table 4. Among the 5 patients with amplified target gene segments, 4 were type 1b, possibly due to the reference sequence AJ238799.1 being the full-length genome sequence of genotype 1b HCV. The common RAS in the NS3 gene segment from 3 patients were A66G and F147S; the common RAS in the NS5A gene segment from 5 patients were Q24/K26/L34V; and the common RAS in the NS5B gene segment from 5 patients were Q47L/R98K/Q127L/A218S, none of which were common RAS on the three gene segments.
Distribution of RAS in the Treatment Failure Group
| No. | Genotype | Medication | NS3 RAS | NS5A RAS | NS5B RAS |
| 1 | 1b | DAC+ASV | S7A, T46S, V48I, Y56H, A66G, P86Q, K87A, P89S, S122G, F147S, D168A, V170I, S181T | Q24, K26, L31V, L34V, K78R, T83M, H85S, Y93H, V164A, K166R, V174T | A25P, Q47L, M57L, D62N, R65Q, Q90K, R98K, K114R, Q127L, A218S |
| 2 | 2a | SOF/VEL+RBV | Q24, K26, R30Q, L34V, L37F, T55A, S101T, T135N, V138L, V153L, V164P, E171D, V174T, V196T, A197V, L199V | A25P, Q47L, M57L, R65Q, K81R, V85I, Q90M, R98K, N117D, K124E, Q127L, T132S, M173R, N206K, A218S, I262V | |
| 3 | 1b | Generic | Q24, K26, R30Q, L31M, L34V, L37F, I74L, H85R, Y93H, C98S, V124I, 138L, A146T, V164A, V174T | Q47L, D62N, R65Q, V85L, Q90K, R98K, K124E, Q127L, T130S, E131V, T137V, A218S, S231N, R254K, I262V, N273 | |
| 4 | 1b | EBR/GZR | V48I, A66G, P86Q, K87S, F147S, A150V, V151A, V170I, M179T | Q24, K26, L31F, L34V, T56I, Y93H, R108K, A115P, V121I, V164A, A197T | A25P, Q47L, K81R, V85I, Q90K, R98K, K100Q, N110S, V116T, K124E, Q127L, E131Q, D135N, N206K, C213S, A218S, S231N, R254K, N273 |
| 5 | 1b | DAC+ASV | A66G, K87A, S122C, F147S | W22, Q24, K26, R30Q, L31M, L34V, T83M, H85C, Y93H, V164A, K166R, V174T | A25P, S46G, Q47L, M57L, Q90K, R98K, K114R, Q127L, A218S, S231N, V235I, Q251R, R254T |
2.4 Comparison of Resistance Between the Two Patient Groups
According to previous studies, the main RAS in the NS3 gene segment are Y56F, Q80K, S122G, V170I; the main RAS in the NS5A gene segment are R30Q, P32A, P58S, Y93H; and the main RAS in the NS5B gene segment are C316N, C451H, and I585C. A total of 39, 38, and 38 gene sequences of NS3, NS5A, and NS5B regions were obtained from the 51 successful treatment patients. The comparison of the main RAS occurrence rates between the 5 treatment failure patients and the 51 successful treatment patients is shown in Figure 1.
From the figure, it can be seen that the most common RAS in the NS3 region of successful treatment patients is S122G, with an occurrence rate of 71.79%, followed by V170I with an occurrence rate of 38.46%; the most common RAS in the NS5A region is Y93H, with an occurrence rate of 21.05%, followed by R30Q with an occurrence rate of 10.53%; the main RAS in the NS5B region is C316N, with an occurrence rate of 71.05%. Among the 3 treatment failure patients, 1 detected S122G and 2 detected V170I in the NS3 gene segment, while Q80K and Y56F were not detected. The common A66G and F147S in the 3 patients were not found in the 51 successful treatment patients; among the 5 treatment failure patients, 4 detected Y93H and 3 detected R30Q in the NS5A gene segment, while P32A and P58S were not detected. The common Q24/K26/L34V in the 5 patients was not found in the 51 successful treatment patients; none of the C316N, C451H, and I585C were detected in the NS5B gene segment of the 5 treatment failure patients, and the common Q47L/R98K/Q127L/A218S was not found in the 51 successful treatment patients.
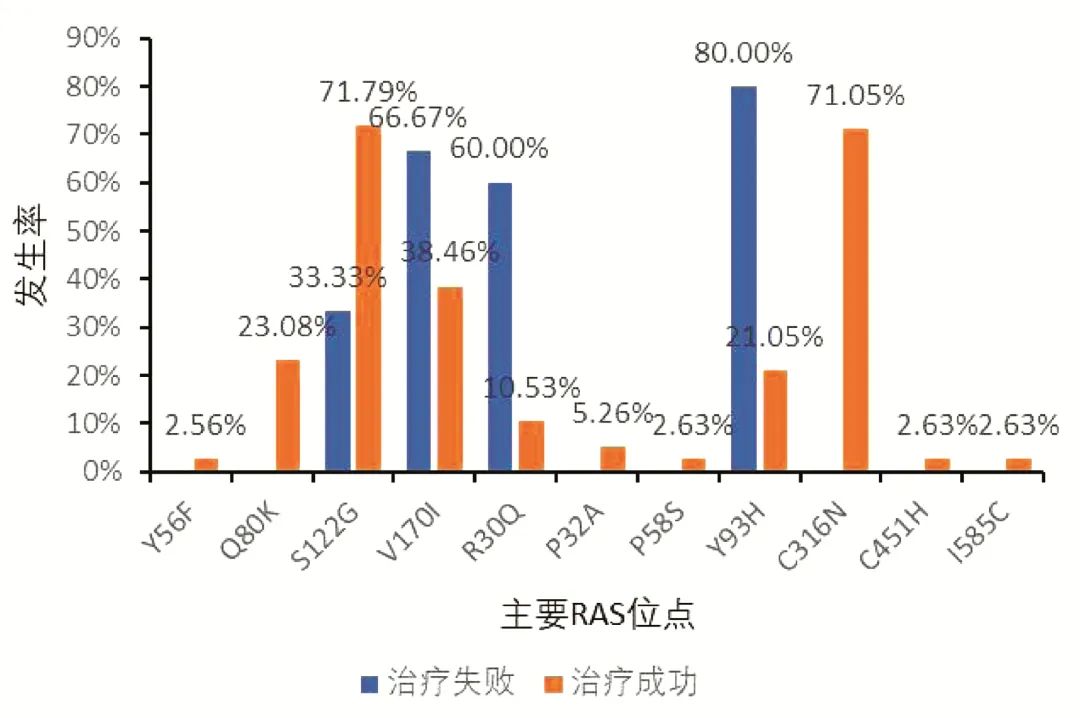
Figure 1 Comparison of RAS Occurrence Rates
3 Discussion
According to previous literature, factors associated with DAA treatment failure include the choice of medication regimen and duration, resistance status (mainly NS5A RAS), genotype, and disease progression (such as liver fibrosis). The results of this study show that HCV RNA relapse due to DAA treatment failure generally occurs within one year post-treatment; baseline TBil, DBil, and Cr levels in male patients are generally higher than those in females, possibly indicating the progression of liver disease, including liver fibrosis, cirrhosis, or liver tumors, which may accelerate the occurrence of DAA treatment failure. All 4 patients with type 3b were treatment failures with sofosbuvir. Sofosbuvir is the most commonly used pan-genotypic DAA in China. According to the 2019 version of the “Guidelines for the Prevention and Treatment of Hepatitis C”, clinical trial results mainly involving the Asian population show that the SVR12 rate of sofosbuvir treatment for 12 weeks is 100%, 100%, 100%, 95%, 76%, and 99% for genotypes 1a, 1b, 2, 3a, 3b, and 6, respectively, indicating a significant decrease in the SVR12 rate for type 3b patients. Type 1b patients have more available treatment regimens, and different regimens may lead to treatment failure and HCV RNA relapse.
Comparing treatment failure and treatment success populations further illustrates that age and genotype are closely related to the success rate of DAA treatment, with type 3b patients more likely to experience treatment failure due to improper treatment regimen choices and disease progression. The SVR12 rate of sofosbuvir for type 3b patients in clinical trials mainly involving the Asian population is 76%, while the SVR12 rate for patients with liver cirrhosis is only 50%, far below the overall SVR rate. This study also found that age may be a risk factor related to DAA treatment failure, with those aged 55 years or younger at higher risk of treatment failure; this conclusion needs to be further validated with a larger sample size.
Previous studies have shown that the occurrence and type of RAS depend on the viral genotype and the drug. RAS is more common in genotypes 1a and 3 compared to other genotypes. It may arise due to exposure to DAA treatment, or it may exist in patients who have not received DAA treatment. In this study, there was a significant difference in RAS between treatment failure and success, possibly due to the interaction between different DAAs and viral nucleic acids that alters the occurrence of RAS.
Elbasvir’s active components include elbasvir and grazoprevir. The most common RAS associated with elbasvir treatment failure is Y93H and L31F/M/V in GT1b, where L31M+Y93H can significantly reduce elbasvir’s efficacy for GT1b patients (reducing it by 5000 times). Common NS3 RAS associated with grazoprevir treatment failure include V36L/M, Y56F/H, Q80K/L, R155I/K/L/S, A156G/M/T/V, V158A, and D168A/C/E/G/K/N/V/Y, primarily found in GT1a, but can also occur in GT1b. Sofosbuvir’s active components are sofosbuvir and velpatasvir. RAS S282T is associated with sofosbuvir treatment failure, but is rarely found in patients who failed sofosbuvir-containing regimens (<4%), possibly due to its lower adaptability and detectable time frame. Studies have shown that L159F(+C316N/L320F) may affect sofosbuvir treatment failure in GT1 and GT3 patients, with L159F+C316N primarily detected in GT1b patients and L159F+V321A only detected in GT1a and GT3 patients. NS5A RAS related to velpatasvir treatment failure involves positions 24, 28, 30, 31, 32, 58, 92, and 93, with the most commonly detected RAS being Q30E/H/K/L/R, M28T/V, Y93C/H/N/S/T, and L31M/V in GT2, and A30K/V, E92K, Y93H/N/R, and L31M/P/V in GT3. Natural NS5A RAS can lead to decreased SVR12 rates in GT3 patients, with patients having Y93H at baseline showing lower SVR rates. RAS associated with daclatasvir treatment failure includes Y93C/H/I/R and L31F/M/V in GT1b, and L31I, Y93H, and A30K in GT3. Y93H is also a common RAS in daclatasvir treatment failure and can be detected in various genotypes.
In this study, treatment failure patients with elbasvir showed L31F+Y93H reducing elbasvir efficacy, but other RAS such as NS3’s V48I/151A/170I, A66G/150V, F147S were also detected. No common RAS affecting sofosbuvir were detected in patients who failed sofosbuvir combined with ribavirin treatment, while common RAS affecting velpatasvir included Q24 and R30Q, but other RAS such as L34V/37F/199V, V138L/153L/164P/174T/196T were also detected. In two patients with treatment failure of daclatasvir combined with asunaprevir, L31V+Y93H and L31M+Y93H affecting daclatasvir were respectively detected, but other RAS such as Q24, K26, L34V, T83M, H85C/S, V164A/174T, K166R were also detected. Among the known RAS targeting different DAAs, this study detected some, such as 31M/93H associated with velpatasvir and elbasvir, and 30Q/31M/93H associated with daclatasvir, while the effects of other detected RAS on DAAs require further exploration.
In summary, DAA treatment failure generally occurs within one year post-treatment, with male patients possibly accompanied by more severe liver disease progression. Patients aged 55 years or younger and those with genotype 3b have a higher risk of treatment failure. As drugs may alter mutation sites, mutation sites may also affect drug efficacy, with significant differences in common RAS before treatment in the successful population and after treatment failure, providing insights for subsequent treatment regimen formulation. This study has certain limitations, including a small total sample size, with relatively few treatment failure patients, and only 5 treatment failure patients having RAS determined, and no successful detection of RAS in serum from 3b type treatment failure patients, making it impossible to discuss the reasons for treatment failure at the genetic level. The correctness of the above statistical inferences and the interaction of RAS with DAA in aiding clinical decision-making await further exploration.

Scan the QR code or click the link below
View the original text or download the PDF for free
http://www.lcgdbzz.org/cn/article/doi/10.3969/j.issn.1001-5256.2022.05.016
 Cite this article
Cite this article
Yang Yuqing, Shang Jia, Lu Chengzhen, Yang Song, Chen Hongyu, Pan Jiali, Han Yifan, Xi Hongli, Kang Qian, Tan Ning, Xu Xiaoyuan. Analysis of Factors Affecting Treatment Failure of Direct Antiviral Drugs for Hepatitis C[J]. Clinical Hepatology and Biliary Diseases, 2022, 38(5): 1059-1063.
This article was edited by: Wang Yanan
Public account editor: Xing Xiangyu

2022 Issue 5
Download the complete PDF
 Further Reading
Further Reading