Lambert-Eaton Myasthenic Syndrome (LEMS) is a disease affecting the neuromuscular junction, caused by the production of antibodies against voltage-gated calcium channels (VGCC) in the patient’s blood, leading to reduced acetylcholine release from the presynaptic membrane, resulting in specific clinical and electrophysiological manifestations. Approximately 50%-60% of LEMS patients have an associated tumor, classified as paraneoplastic syndrome (PNS), known as tumor-associated LEMS (T-LEMS), with small cell lung cancer (SCLC) being the most common tumor. Other, less common tumors include prostate cancer, leukemia, and lymphoma. Conversely, some LEMS patients have been followed for a long time without any tumor detection, classified as non-tumor LEMS (NT-LEMS), with an unclear pathogenesis. Although both types present similar clinical symptoms, their prognoses are markedly different, and the focus of treatment post-diagnosis varies. More than half of NT-LEMS patients can achieve complete remission through immunotherapy, and the disease does not affect survival, hence the focus is more on treatment post-diagnosis. In contrast, T-LEMS patients require a detailed tumor screening plan after diagnosis, with antitumor therapy being the preferred treatment method once a tumor is detected. Only about 5% of T-LEMS patients are diagnosed with both LEMS and a tumor simultaneously, while approximately 86% of T-LEMS patients exhibit LEMS symptoms before the tumor appears. Therefore, a diagnosis of NT-LEMS cannot be simply assigned when a tumor is not found at the time of LEMS diagnosis, and administering immunosuppressive treatment for T-LEMS prior to tumor detection may accelerate the growth of potential tumors, making differential diagnosis between the two critically important. Due to the relative rarity of LEMS, most studies in China are retrospective, focusing on the clinical manifestations, electrophysiological performance, and treatment of LEMS, with no specific research on the differential diagnosis between N-LEMS and NT-LEMS. However, several studies abroad have explored the differences between the two, including pathogenesis, clinical manifestations, and serological indicators. This article provides a review of these aspects.
Clinical Features and Diagnostic Criteria of LEMS
The clinical manifestations of LEMS primarily include fluctuating proximal weakness in the limbs, reduced or absent tendon reflexes, and autonomic nervous dysfunction triad. Limb weakness often begins in the lower extremities, with more severe symptoms in the morning that can improve with activity. The most common symptom of autonomic nervous dysfunction is dry mouth, followed by constipation, erectile dysfunction (in male patients), and abnormal sweating. Unlike myasthenia gravis (MG), isolated extraocular muscle involvement is rare. Electrophysiologically, while some LEMS patients may show myopathic changes on electromyography, the most characteristic electrophysiological finding is a general decrease in amplitude at rest, increased amplitude after brief tetanic stimulation (greater than 100%), and a decrease in amplitude with low-frequency stimulation (≤5Hz, decrease greater than 10%), while high-frequency stimulation shows an increase in amplitude (≥10Hz, increase greater than 100%). The clinical triad combined with the electrophysiological triad can diagnose LEMS even in the absence of VGCC antibodies.
Pathogenesis of LEMS
VGCC is composed of five subunits: α1, α2, β, γ, and δ, with the α1 subunit being the key component forming the calcium ion influx channel. VGCC is divided into six subtypes: P, Q, N, L, T, and R. Due to the similar electrophysiological characteristics of Q-type to P-type and its susceptibility to inactivation, it is often represented as P/Q. P/Q-type, N-type, and R-type VGCC are widely present in the nervous system, participating in neurotransmitter transmission and release, with acetylcholine release at the neuromuscular junction primarily relying on P/Q-type VGCC. Approximately 85%-90% of LEMS patients can detect anti-P/Q-type VGCC antibodies, with no significant difference between T-LEMS and NT-LEMS. Anti-P/Q-type VGCC antibodies have been proven to be pathogenic; transferring these antibodies into rats can induce clinical and electrophysiological manifestations similar to LEMS. Mice with mutations in P/Q-type VGCC also exhibit similar clinical and electrophysiological manifestations. Recent studies using culture media containing IgG from LEMS patients found that the voltage-dependent synaptic vesicle release efficiency of neurons was significantly reduced, while the same culture method applied to P/Q-type VGCC knockout neurons showed no effect, further confirming that the antibody causes disease through P/Q-type VGCC. At the neuromuscular junction, the presence of anti-P/Q-type VGCC antibodies limits VGCC function, reducing presynaptic calcium ion influx and subsequently decreasing the quantal release of acetylcholine, lowering the safety factor of the neuromuscular junction, thus causing a series of clinical and electrophysiological manifestations. Similarly, in the autonomic nervous system, the inhibition of P/Q-type VGCC function leads to reduced acetylcholine release from preganglionic fibers (sympathetic and parasympathetic) and postganglionic fibers (parasympathetic), resulting in corresponding symptoms of autonomic nervous dysfunction.
The cause of antibody production remains unclear. In T-LEMS patients, tumor cells (especially SCLC) also express P/Q-type VGCC antigens, suggesting that the production of T-LEMS antibodies is related to immune cross-reactivity. Symptoms of LEMS in these patients significantly improve after tumor treatment, and SCLC patients with LEMS have a longer survival than those without LEMS, indicating that the development of T-LEMS may be related to enhanced immune surveillance in tumor patients, while the mechanism of antibody production in NT-LEMS patients remains unclear.
P/Q-type VGCC is not only present at the neuromuscular junction but also on the surface of cerebellar Purkinje cells and granule cells. There are many reports of co-morbidity between T-LEMS and paraneoplastic cerebellar degeneration (PCD). Autopsy confirmed that P/Q-type VGCC is reduced by 70%-80% in the cerebellar molecular layer of T-LEMS patients with PCD, with an increased ratio of remaining cerebellar P/Q-type VGCC binding to endogenous IgG; however, this reduction was not observed in patients with isolated T-LEMS. Anti-P/Q-type VGCC antibodies can be detected in the serum of 24%-41% of PCD patients (with or without LEMS), with some showing elevated P/Q-type VGCC antibodies in cerebrospinal fluid (CSF), and some evidence of intrathecal synthesis of these antibodies. Given the presence of the same antibodies, why is only a small portion of T-LEMS patients associated with PCD? Why are cerebellar symptoms rare in NT-LEMS patients? The following hypotheses can be proposed: both T-LEMS and PCD are related to SCLC, thus increasing the likelihood of co-morbidity, while the antigen triggering antibody production in NT-LEMS remains unknown. Additionally, although the same antibodies are detected, different tissue antigens may trigger different clinical effects. Some studies injected IgG containing VGCC antibodies from PCD patients with LEMS and isolated LEMS patients into mouse CSF, finding that mice receiving the former’s IgG developed marked ataxia, while those receiving the latter’s did not, further confirming that the anti-P/Q-type VGCC antibodies in PCD patients with LEMS may have specific antigenic epitopes. Clinically, T-LEMS patients with PCD show symptom improvement after tumor treatment, while PCD symptoms do not alleviate, and PCD patients exhibit characteristics such as Purkinje cell loss and cerebellar cortical gliosis, leading to the hypothesis that the pathogenesis of PCD is primarily mediated by T cell cytotoxic immune responses, while the presence of anti-P/Q-type VGCC antibodies in PCD patients may also be secondary to cellular immune responses.
Previous Studies on the Distinction Between T-LEMS and NT-LEMS
Currently, there is a lack of effective biological markers for classifying LEMS. How have previous studies defined T-LEMS and NT-LEMS? Diagnosing LEMS based on the presence of associated tumors is evidently unreliable; thus, the diagnosis of NT-LEMS primarily relies on follow-up. There is no definitive conclusion on the duration of follow-up required, nor whether finding a tumor categorizes it as T-LEMS. Since T-LEMS is a type of PNS, it should conform to the relevant characteristics of PNS. In 2004, Graus et al. established a series of diagnostic recommendations for PNS (including T-LEMS), suggesting that confirmed PNS should meet the following criteria: typical neurological symptoms should occur within five years of tumor detection; neurological symptoms and signs can alleviate through tumor treatment; and the presence of tumor-associated neuronal antibodies. It can be seen that a diagnosis of NT-LEMS is more likely if no tumor is found five years after LEMS diagnosis. Currently, the average follow-up period for NT-LEMS patients is 3-5 years, with negative tumor-associated neuronal antibodies. Some studies have found tumors during the follow-up period for LEMS, but not SCLC, and LEMS did not improve after tumor resection, thus they were also classified as NT-LEMS.
Differentiation Between T-LEMS and NT-LEMS
4.1 Clinical Manifestations A summary analysis of 227 LEMS patients indicated that the median age of onset in the NT-LEMS group was younger than that in the T-LEMS group (49 years vs. 58 years). In terms of gender composition, T-LEMS patients are predominantly male (70%), while there is no significant gender difference in the NT-LEMS group. The median time from onset to LEMS diagnosis is significantly longer in NT-LEMS patients (13.5 months) compared to T-LEMS patients (5 months). The proportion of weight loss is higher in the T-LEMS patient group than in the NT-LEMS group. NT-LEMS patients are more likely to be associated with other autoimmune diseases. Additionally, smoking rates are significantly higher among T-LEMS patients. Studies show that the most common comorbidity in NT-LEMS is hyperthyroidism, followed by insulin-dependent diabetes, with other autoimmune diseases including systemic lupus erythematosus, psoriasis, rheumatoid arthritis, and pernicious anemia. Some NT-LEMS patients may have a history of infection before onset, and cases of LEMS triggered by influenza vaccination have also been reported. Notably, LEMS with MG (with serological evidence) has been widely reported, and most do not have associated tumors. In contrast, T-LEMS patients are more likely to have other types of PNS, with reports of not only the most common PCD but also strabismus-myoclonus syndrome, paraneoplastic sensory neuropathy, and limbic encephalitis.
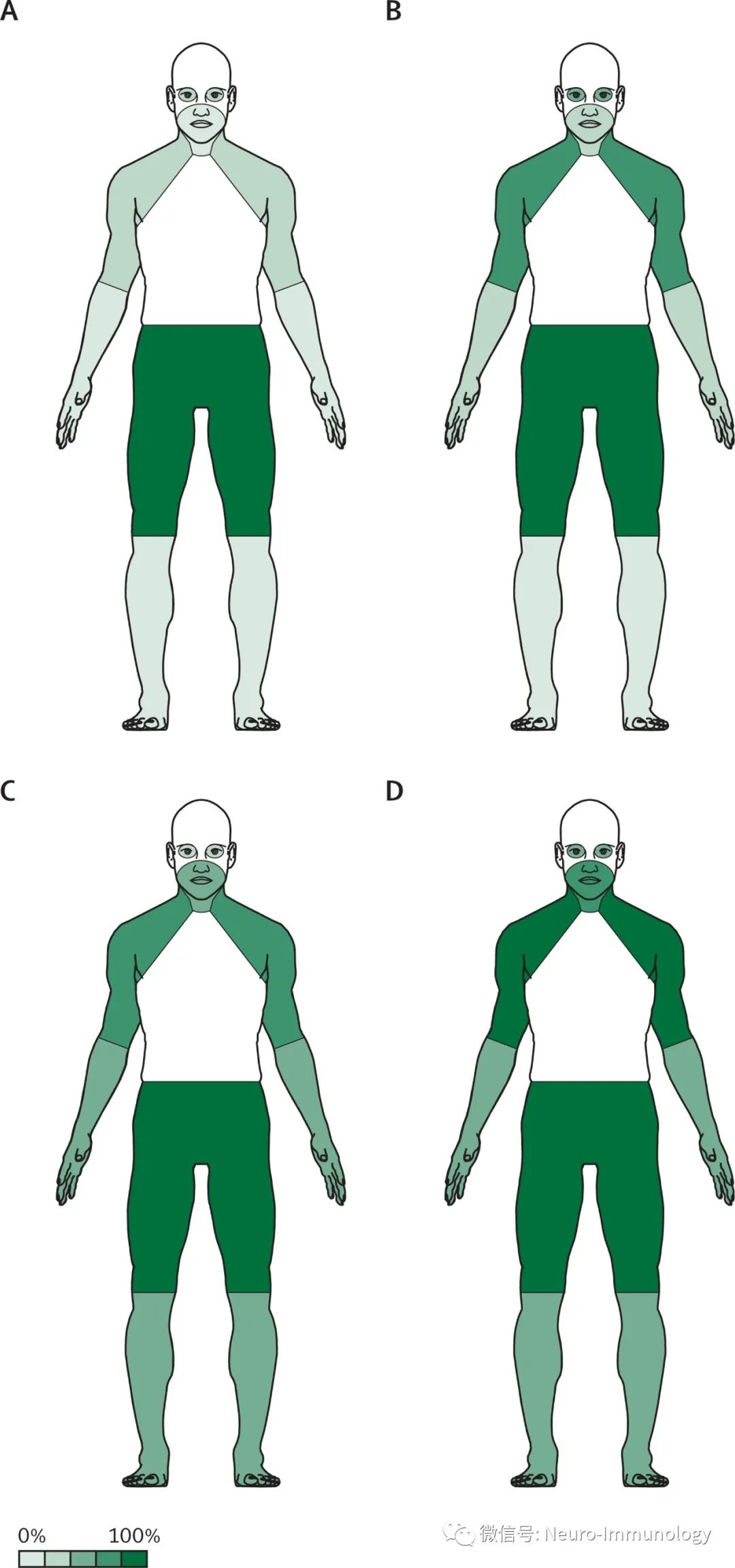
Figure 1: Symptom distribution of NT-LEMS patients at 3 months (A) and 12 months (B), as well as SCLC-LEMS patients at 3 months (C) and 12 months (D); percentages describe the approximate proportion of patients with involvement in that area within the given time frame; NT=non-tumor; LEMS=Lambert-Eaton Myasthenic Syndrome; SCLC=small cell lung cancer; Source: Titulaer MJ, Lang B, Verschuuren JJ. Lambert-Eaton myasthenic syndrome: from clinical characteristics to therapeutic strategies. Lancet Neurol. 2011 Dec;10(12):1098-107.
4.2 Tumor-Associated Prediction Scoring in LEMS Based on previous clinical research results, Titulaer et al. developed the Dutch-British LEMS tumor-associated prediction score (DELTA-P) and conducted sensitivity and specificity studies. The following clinical conditions increase the DELTA-P score by 1 point: bulbar symptoms (difficulty swallowing, choking while drinking, dysarthria, neck muscle weakness, etc.); erectile dysfunction (in male patients); weight loss ≥5%; smoking history; age of onset >50 years; Karnofsky performance status score of 0-60. When the score is 0-1, the probability of SCLC is 0-2.6%, essentially ruling out T-LEMS, whereas scores of 3-6 indicate probabilities of SCLC at 83.9%, 93.5%, 96.6%, and 100%, respectively. This scoring method is relatively simple and easy to operate, but the study population is based on Dutch and British patients, requiring further validation in China.
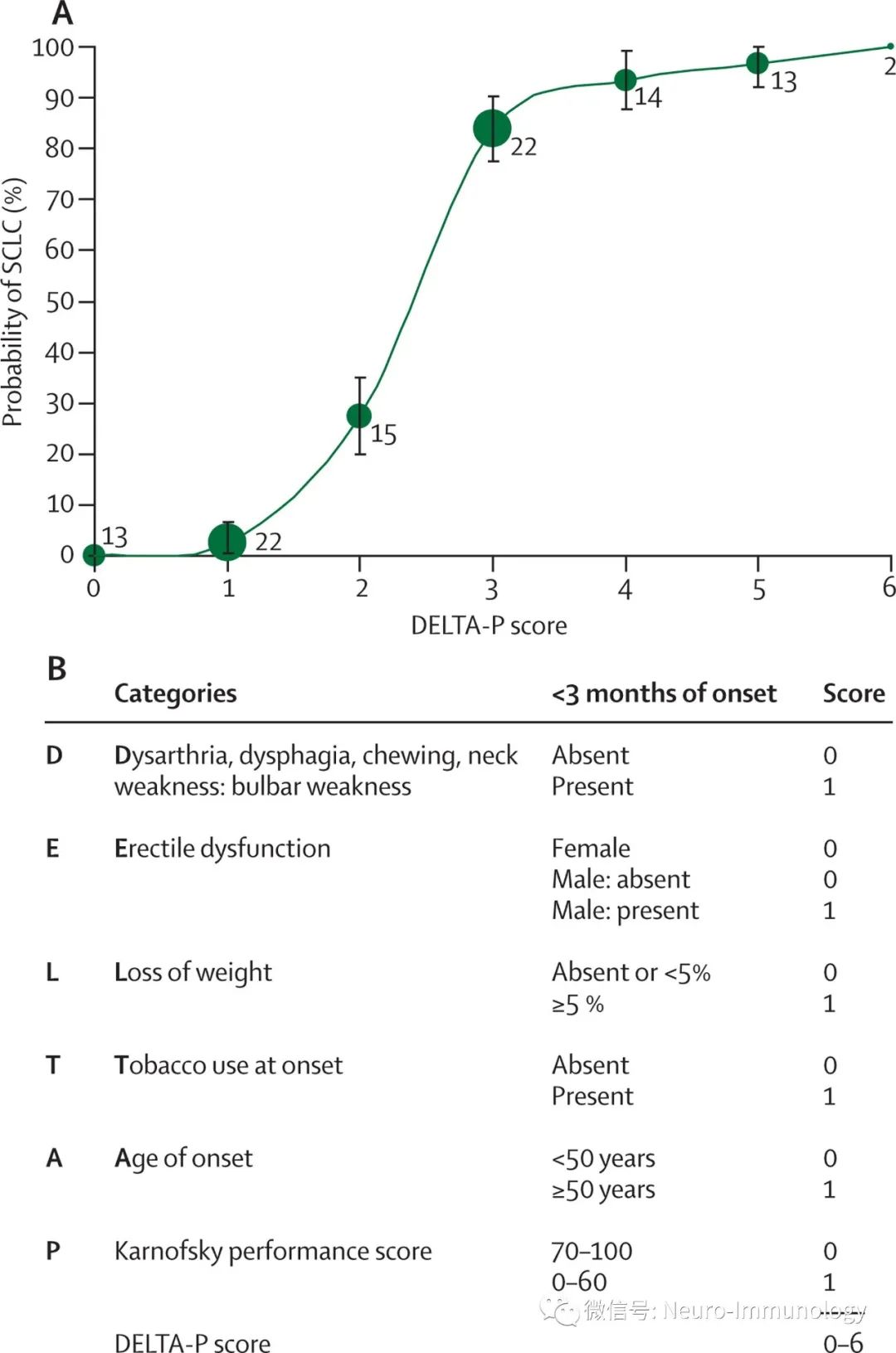
Figure 2: DELTA-P score; Source: Titulaer MJ, Lang B, Verschuuren JJ. Lambert-Eaton myasthenic syndrome: from clinical characteristics to therapeutic strategies. Lancet Neurol. 2011 Dec;10(12):1098-107.
4.3 Anti-Glial Nuclear Antibody (AGNA)/SOX1 Antibody Graus et al. found an antibody in the serum of 24 PNS patients that stained the Bergmann glial cell nuclei layer of rat cerebellar Purkinje cells, although its antigen was not identified at the time, thus named anti-glial nuclear antibody. Their research found that this antibody was present at a higher proportion in T-LEMS patients compared to other types of PNS, while NT-LEMS patients did not show this antibody. In a subsequent study, Graus et al. identified the antigen of this antibody as SOX1, which belongs to a large family of developmental transcription factors, divided into types A-H, with SOX1 belonging to type SOXB, which is actively expressed during neural development and downregulated in adults except for a few areas. SOX1 is expressed in Bergmann glial cells of the adult cerebellum. Studies have confirmed that SOX1 is present on the surface of SCLC cells, thus SOX1 antibodies can be detected in the serum of T-LEMS patients, with a positive rate of up to 64%, further confirming that NT-LEMS patients do not have this antibody. However, whether this antibody can be detected in T-LEMS before tumor occurrence, and whether it has predictive value for tumors, requires further prospective studies.
4.4 Tumor-Associated Neuronal Antibodies Due to the expression of certain antigens by tumors that have cross-immunity with components of the nervous system, tumor-associated neuronal antibodies are produced. Different types of tumor-associated neuronal antibodies are related to tumor types. Studies indicate that anti-Hu antibodies are expressed at higher levels in SCLC patients, appearing in about 30% of SCLC patients with LEMS. Simultaneously, using ELISA to detect both anti-SOX1 and anti-Hu antibodies can improve the diagnostic sensitivity for T-LEMS, and the method is relatively simple, potentially suitable for clinical screening.
4.5 HLA Polymorphism HLA polymorphism has been confirmed to be related to genetic susceptibility to various autoimmune diseases. In 2000, Parsons et al. confirmed that HLA II molecules DR3 and DQ2 are associated with NT-LEMS. A 2001 study on HLA polymorphism in 19 Caucasian NT-LEMS patients indicated that the haplotype HLA-B8-DR3-DQ2 was significantly higher in NT-LEMS patients compared to the control group, while the aforementioned three molecules also showed strong correlation in MG Caucasian patients, and no difference was found in T-LEMS patients compared to the control group. In a few HLA-B8 positive T-LEMS patients, their survival after LEMS diagnosis was notably longer than that of HLA-B8 negative T-LEMS patients, suggesting that HLA-B8 negative smokers are a strong predictive indicator for T-LEMS and indicate poor prognosis. There is currently a lack of data on HLA molecular polymorphism studies in LEMS patients in China.
4.6 Reactivity of Antibodies to Different Structural Domains of the P/Q-type VGCC α1 Subunit The α1 subunit is the main functional region of VGCC, which has four structural domains (I-IV). Studies have shown that 90% of antibodies reacting with domain IV are found in LEMS patients without tumors, which is significant for differentiating T-LEMS from NT-LEMS. However, due to a small sample size, further validation is needed, and the detection method is complex, making it unsuitable for clinical screening.
In summary, this article comprehensively reviews the research results of T-LEMS and NT-LEMS regarding pathogenesis, clinical manifestations, serology, etc., providing some reference for clinicians in classifying LEMS and assessing the risk of tumors in patients, thereby developing appropriate tumor screening plans and treatment strategies to maximize patient benefits. Although progress has been made in research, there is still a lack of a recognized and operable “gold standard” for differentiating pre-tumor T-LEMS from NT-LEMS, and most studies are based on foreign populations. The proportion, clinical characteristics, comorbidities, and genetic susceptibility of NT-LEMS patients in China may not necessarily have similar characteristics to foreign populations, and further research is needed to confirm whether the DELTA-P score is applicable to the Chinese population.
Clinical Neurology Journal October 2015, Volume 28, Issue 5
Authors: Zhang Dong, Li Wei, Yan Chuan Zhu, Cao Li Li(Department of Neurology, Shanxi Medical University First Hospital)
Typesetting: You Chun
Initial Review:Sun Xue Ting
Re-review:Wan Cheng Qun
Final Review:Cai Zhi You