
Angina is the most common symptom of ischemic heart disease, with about 112 million people worldwide suffering from coronary heart disease. Among patients undergoing invasive coronary angiography (CAG), about 70% do not have obstructive coronary artery disease (CAD), with a significant portion being ischemia with non-obstructive coronary artery disease (INOCA). In 2020, the European Association of Percutaneous Cardiovascular Interventions (EAPCI) and the European Society of Cardiology (ESC) Coronary Pathophysiology and Microcirculation Working Group jointly published an expert consensus document outlining the latest perspectives on INOCA.
On October 27, 2021, at the 32nd Great Wall Cardiology Conference (GW-ICC 2021), Professor Jin Yuanzhe from the Fourth Hospital of China Medical University provided an insightful interpretation of the 2020 EAPC/ESC expert consensus on ischemia with non-obstructive coronary artery disease, offering guidance for the diagnosis and management of INOCA.
Definition of INOCA
Up to 70% of angina patients show no obstructive coronary artery stenosis (stenosis >50%) upon CAG examination, and their symptoms can easily be misattributed to non-cardiac causes, leading to inadequate treatment. Clinically, this condition characterized by suspected ischemic-related symptoms but without obstructive coronary artery stenosis found on CAG is defined as ischemia with non-obstructive coronary artery disease (Ischemia and No Obstructive Coronary Artery Disease, INOCA).
Types of Disease
Based on pathophysiological characteristics, INOCA can be classified into microvascular angina (MVA) and vasospastic angina (VSA). Microvascular angina (MVA) is angina caused by myocardial ischemia due to microvascular dysfunction, with diagnostic criteria as shown in Table 1. Microvascular dysfunction may be caused by microvascular remodeling or abnormal vasodilation of coronary small arteries, or both. Table 1: Diagnostic Criteria for Microvascular Angina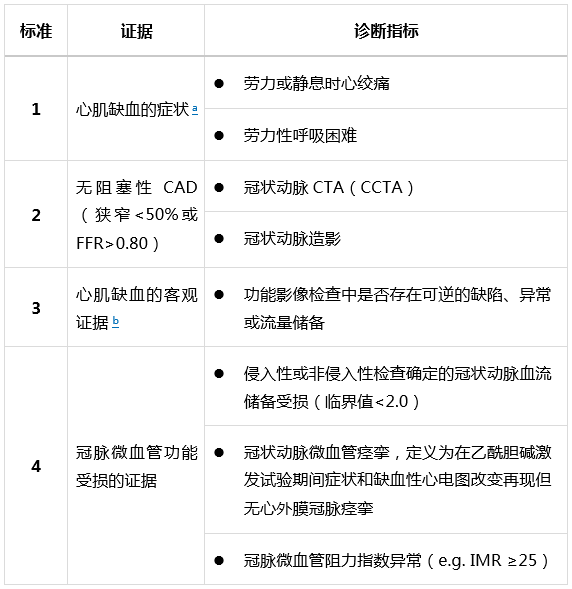 Note: MVA can only be diagnosed if the above four criteria are met. a. Many patients with preserved ejection fraction heart failure meet the following criteria: dyspnea, no obstructive CAD, and impaired CFR. Therefore, it is important to consider measuring left ventricular end-diastolic pressure (normal ≤10mmHg) and NT-proBNP (normal <125 pg/mL). b. Local ischemic signs may be present but are not mandatory; evidence of impaired coronary microvascular function should be available. Vasospastic angina (VSA) refers to myocardial ischemia caused by transient obstruction of epicardial coronary arteries due to abnormal vasomotion, with variant angina being one type. Triggers for vasospasm include smoking, drugs, sudden hypertension, cold, emotional stress, hyperventilation, and allergic reactions, among others. Adjacent segments of coronary arteries where drug-eluting stents are placed are also prone to spasm. MVA and VSA can coexist and are associated with poor prognosis.
Note: MVA can only be diagnosed if the above four criteria are met. a. Many patients with preserved ejection fraction heart failure meet the following criteria: dyspnea, no obstructive CAD, and impaired CFR. Therefore, it is important to consider measuring left ventricular end-diastolic pressure (normal ≤10mmHg) and NT-proBNP (normal <125 pg/mL). b. Local ischemic signs may be present but are not mandatory; evidence of impaired coronary microvascular function should be available. Vasospastic angina (VSA) refers to myocardial ischemia caused by transient obstruction of epicardial coronary arteries due to abnormal vasomotion, with variant angina being one type. Triggers for vasospasm include smoking, drugs, sudden hypertension, cold, emotional stress, hyperventilation, and allergic reactions, among others. Adjacent segments of coronary arteries where drug-eluting stents are placed are also prone to spasm. MVA and VSA can coexist and are associated with poor prognosis.
Clinical Presentation and Prognosis
The clinical presentation of INOCA can resemble the angina symptoms of obstructive coronary heart disease and may also present as shortness of breath, interscapular pain, dyspepsia, nausea, fatigue, weakness, vomiting, and sleep disturbances. The clinical symptoms and signs vary widely among patients, often misattributed to non-cardiac causes, leading to inadequate treatment.
INOCA is associated with reduced quality of life, loss of daily work ability, and increased rates of mortality, morbidity, readmission, and repeat coronary angiography. Vasospastic angina is related to adverse events such as cardiac sudden death, acute myocardial infarction, and syncope.
Diagnosis and Assessment
In clinical practice, non-invasive tests are preferred for assessing angina. Various non-invasive techniques, including exercise tolerance tests, transthoracic Doppler echocardiography (TTDE), myocardial contrast echocardiography (MCE), myocardial perfusion imaging, positron emission tomography (PET), and cardiac magnetic resonance imaging (CMR), can detect local ischemia in INOCA.
Invasive techniques, including coronary angiography, diagnostic wires, pressure and flow measurements, and pharmacological tests, can be used to differentiate between vasospastic angina, microvascular angina, and non-cardiac pain.
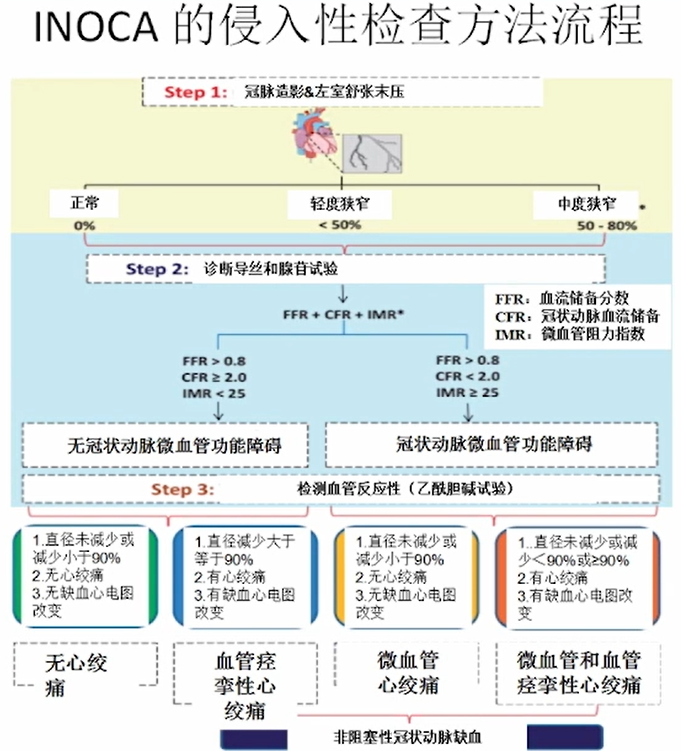 Table 2: Clinical Classification and Diagnostic Criteria for INOCA
Table 2: Clinical Classification and Diagnostic Criteria for INOCA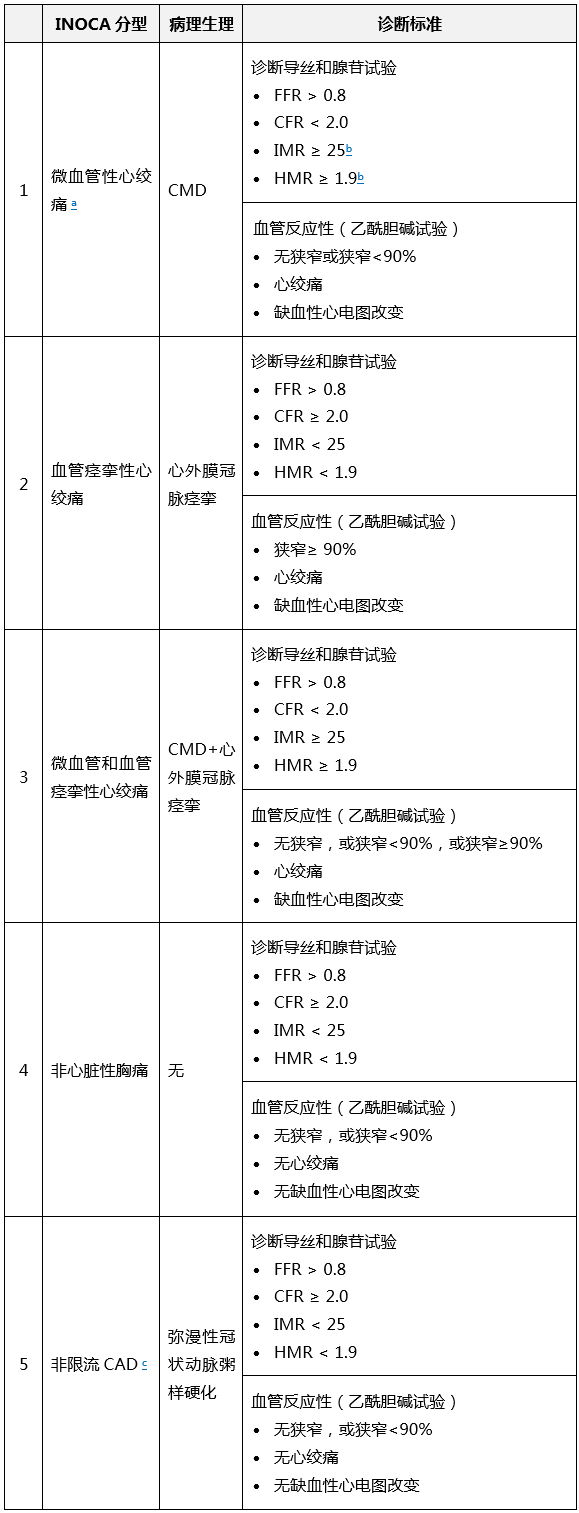 Note: CAD, coronary artery disease; CFR, coronary flow reserve; FFR, fractional flow reserve; HMR, microvascular resistance; IMR, index of microvascular resistance.
Note: CAD, coronary artery disease; CFR, coronary flow reserve; FFR, fractional flow reserve; HMR, microvascular resistance; IMR, index of microvascular resistance.
Management of INOCA
INOCA requires individualized, routine, multidisciplinary intervention and treatment, primarily including lifestyle modifications, risk factor management, and anti-anginal medication therapy. Lifestyle interventions include diet, exercise, weight control, smoking cessation, and stress management. Risk factor management includes controlling blood pressure, blood lipids, and blood glucose. Strict blood pressure control aims to prevent the progression of microvascular changes and reduce the frequency and severity of angina. Anti-anginal medications include ACEI/ARB, CCB, β-blockers, and nitrates, with the selection of drugs for INOCA primarily as shown in Table 3.Table 3: Pharmacological Treatment for INOCA
Conclusion
INOCA is a significant issue currently facing the cardiovascular field, with challenges including inadequate diagnosis, insufficient treatment, and poor prognosis. Clinicians need to have a thorough understanding of INOCA and conduct appropriate non-invasive or invasive examinations for patients suspected of having INOCA. After obtaining a clear diagnosis, specific multidisciplinary treatment plans should be determined based on the individual characteristics of the patient. In the future, more clinical research is needed to address the unresolved issues in the field of INOCA.References: Kunadian V, Chieffo A, Camici PG, et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J. 2020 Oct 1; 41(37): 3504-3520.