Surgical Management for Primary Intracerebral Hemorrhage
A study from American researchers reviewed previous literature and conducted a systematic review of surgical treatments for primary intracerebral hemorrhage. The research was published in the 2024 issue of Neurology.

PMID:39074339 DOI: 10.1212/WNL.0000000000209714
Abstract
The incidence of primary intracerebral hemorrhage is increasing annually, especially among younger patients, partly due to the increased use of anticoagulants. From 2016 to 2018, the incidence of intracerebral hemorrhage (ICH) in the United States was nearly 79/100,000 person-years, with an incidence rate of 367/100,000 person-years in people aged 75 and older. Globally, ICH accounts for 28% of all newly diagnosed strokes, and due to the higher incidence and mortality rates of ICH, the disease burden exceeds that of ischemic strokes. Although the mortality rate of ICH appears to be declining, functional prognosis has not improved significantly. Following negative conclusions from clinical trials on craniotomy for hematoma evacuation, recent clinical trials of comprehensive medical management strategies, including enhanced blood pressure control and anticoagulants aimed at reducing hematoma expansion, have failed to achieve definitive efficacy. Meanwhile, ongoing interest in minimally invasive hematoma evacuation techniques stems from the recognition of secondary iatrogenic damage caused by craniotomy to the subcortical white matter tracts. Recent studies have shown positive conclusions for minimally invasive surgical treatment of lobar hemorrhage, thus necessitating a reconsideration of surgical approaches for ICH. In this narrative review, the authors summarize landmark studies, review recent literature, and discuss unresolved issues surrounding surgical management of ICH.
Research Background
Intracerebral hemorrhage leads to cranial nerve injury through the physiological mechanisms of hyperacute, acute, and subacute phase cases. Direct tissue damage caused by white matter tract destruction represents primary, persistent mechanical injury. The mass effect of the hematoma causes compression of the white matter tracts, but function may remain intact, potentially restored by removing the mass effect of the hematoma. The mass effect can also lead to increased intracranial pressure and secondary abnormal brain perfusion, which can be restored by hematoma removal. Patient prognosis depends on the degree of mass effect, namely the volume of the hematoma and its correlation with critical functional areas. Hematoma expansion exacerbates primary mechanical injury, typically completing this bleeding event within hours of onset. Pharmacological trials aimed at reducing hematoma expansion have either failed to meet their targets or have been unable to improve patient prognosis due to limited reductions in hematoma expansion. Secondary injury is driven by neurotoxic blood degradation products (including reactive oxygen species and iron), yet to date, medical therapies targeting these treatment goals have proven futile. Similarly, only recently have trials of surgical treatment for ICH begun to show benefits. Newly published trials on minimally invasive surgical treatment of lobar hemorrhage and decompressive craniectomy for severe deep intracerebral hemorrhage have brought new prospects to this field.
This narrative review summarizes landmark surgical research on intracerebral hemorrhage, reviews recent literature, and outlines unresolved issues in the field. The article describes current evidence and areas needing further research, including optimal techniques and timing for surgical management, the effects of surgery on non-lobar hemorrhages, potentially benefiting patient populations, administrative issues regarding equitable access to advanced surgical methods, and the impact of surgery on prognosis. To ensure a comprehensive review of the latest literature advancements, the authors enlisted a medical librarian with expertise in review writing to search the literature from the past 4 years (Table 1).
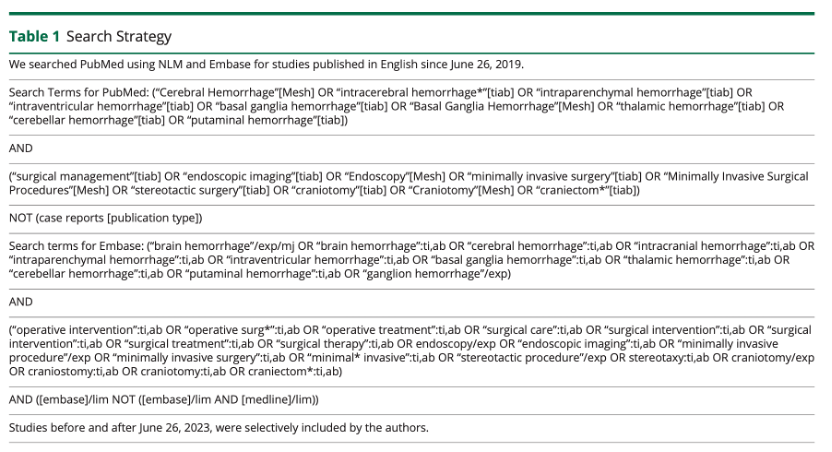
Table 1 Literature Search Strategy
Landmark Clinical Trials
In 2005, the International Surgical Trial for Intracerebral Haemorrhage (STICH) randomized 1033 patients to early surgery (median time from onset to surgery was 30 hours) or initial conservative treatment (Table 2). The trial found no benefit in clinical outcomes for the surgical group, with benefits only observed in subgroup analysis for patients with hematomas located 1 cm from the cortical surface. Although subsequent studies on this subgroup in STICH II similarly failed to show benefits from open surgical hematoma evacuation, the conclusion was that the damage caused by surgery offset the benefits of hematoma removal, which drove the development of minimally invasive surgical (MIS) techniques. These techniques include passive drainage methods, such as stereotactic thrombolysis and active hematoma drainage techniques using endoscopy.
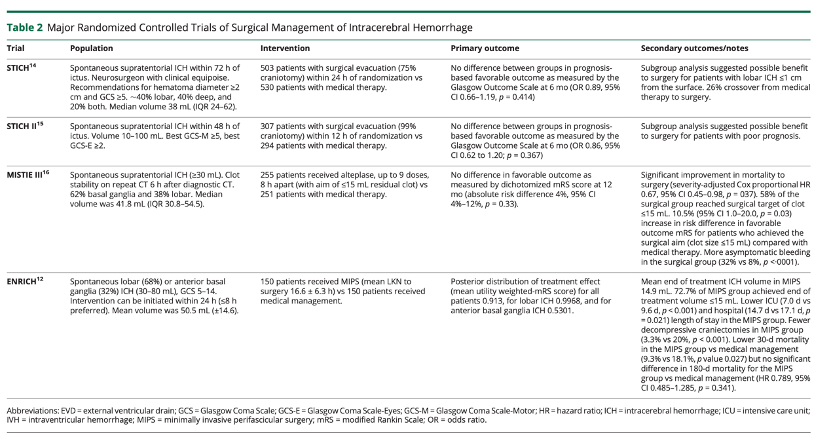
Table 2 Major Randomized Controlled Clinical Trials for Surgical Treatment of Intracerebral Hemorrhage
The MISTIE III trial published in 2015 is the first large randomized controlled trial of minimally invasive treatment for intracerebral hemorrhage. The MISTIE surgical process includes establishing a hematoma access channel under imaging guidance, followed by hematoma aspiration with a syringe, and finally passive drainage through the placement of a drainage tube in the hematoma cavity, during which continuous infusion of alteplase may be used to promote hematoma lysis and subsequent drainage (Figure 1). Compared with standard treatment, the trial found no improvement in patient prognosis; however, the surgery did improve the one-year survival rate. Secondary analyses indicated that for patients achieving surgical goals, namely residual hematoma volume ≤15 mL, the procedure was associated with significant improvement in functional prognosis, and the degree of hematoma clearance was correlated with the chance of achieving a good prognosis, with residual hematoma volume being a better predictor of good prognosis than the percentage reduction in hematoma. Therefore, MISTIE III established a target of ≤15 mL for residual hematoma volume. Larger initial hematoma volumes, a history of hypertension, irregular hematoma shapes, and issues related to catheter placement were associated with failure to achieve surgical targets, while more experienced surgeons and increased onsite surgical experience were correlated with higher success rates. In patients with lobar hemorrhage only in MISTIE III, a residual hematoma ≤28.8mL was associated with an increased likelihood of good functional prognosis. Insufficient or slow hematoma drainage may affect overall prognosis. In MISTIE III, the average time from onset to surgery was 58.3 hours, and the mean time to complete treatment was 123 hours. A meta-analysis on surgical treatment for ICH found that early hematoma clearance could improve outcomes, and the delayed achievement of surgical targets or slow drainage in MISTIE III may be one reason for the lack of positive conclusions.
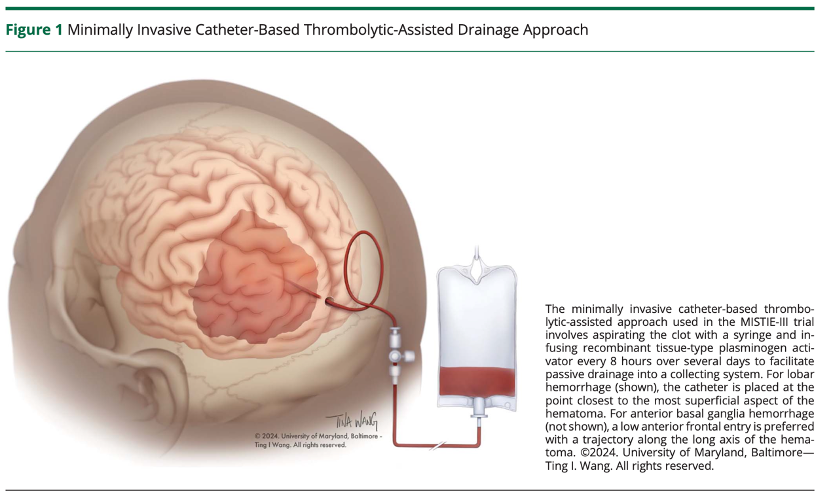
Figure 1 Minimally Invasive Techniques for Drainage Tube Placement and Thrombolysis-Assisted Drainage
The MISTIE-III trial utilized hematoma cavity drainage tube placement and minimally invasive thrombolysis-assisted methods, including suctioning the blood clot with a syringe and administering rt-PA every 8 hours within the first few days of treatment to promote passive drainage of the hematoma. For lobar hemorrhage (as shown), the external drainage tube was placed at the shallowest point near the hematoma. For basal ganglia hemorrhage, a low frontal approach was preferred, with the drainage tube placed along the long axis of the hematoma.
Recent Literature
In 2022, the American Heart Association (AHA) guidelines recommended surgical treatment for patients with intracerebral hemorrhage to save lives from deteriorating conditions, but did not recommend surgery to improve functional prognosis. The guidelines proposed a weak recommendation to consider minimally invasive treatment rather than traditional craniotomy to improve functional prognosis. Experts have varying opinions on surgical treatment. A survey conducted in 2021 among 140 neurosurgeons and 378 neurologists in Dutch hospitals showed significant differences in recommendations for surgery for patients. The survey also found that neurosurgeons had a strong preference for traditional craniotomy that greatly exceeded that for minimally invasive surgery. Many recent analyses have evaluated the various advantages and disadvantages of traditional craniotomy techniques, minimally invasive surgical techniques, and conservative treatment.
Traditional Craniotomy vs. Conservative Treatment
Recent propensity-matched analyses of patients with moderate to large ICH undergoing routine craniotomy for hematoma evacuation found poorer outcomes in patients receiving surgical treatment compared to those receiving medical treatment. In contrast, a 2020 network meta-analysis (a statistical technique using direct and indirect comparisons) analyzing 12 randomized controlled trials of open and minimally invasive treatment techniques found that traditional craniotomy may indeed improve mortality and functional prognosis compared to medical treatment. However, these conclusions could not be replicated in the authors’ traditional meta-analysis of the same studies, nor in the separate meta-analysis of 6 randomized controlled trials. Thus, these studies suggest that traditional craniotomy does not benefit patients with intracerebral hemorrhage.
Decompressive Craniectomy vs. Conservative Treatment
For patients with larger hematoma volumes, a less invasive option is decompressive craniectomy without hematoma evacuation. A propensity-matched analysis of decompressive craniectomy without hematoma evacuation for supratentorial intracerebral hemorrhage found lower mortality rates and better functional prognosis at 3 months compared to the conservative treatment control group. The SWITCH study is a randomized controlled trial involving patients aged 18-75 with severe deep (basal ganglia or thalamic) hemorrhage (30-100 mL), exploring the efficacy of decompressive craniectomy within 72 hours of onset compared to conservative treatment. The planned enrollment was 300 cases, but the trial was halted after 201 cases due to lack of sponsorship. The primary outcome was mortality or dependency level at 6 months (modified Rankin scale [mRS] score of 5 and 6). Point estimates support decompressive craniectomy (relative risk 0.77,95%CI 0.59-1.01, p=0.057), but the results were not statistically significant. Predefined secondary outcomes, including changes in mRS classification at 6 months and length of hospital stay, showed better outcomes for patients undergoing decompressive craniectomy. Based on these research conclusions, considering decompressive craniectomy without hematoma evacuation for patients with severe deep intracerebral hemorrhage seems reasonable.
Hematoma Evacuation with or without Decompressive Craniectomy
Recent comparisons of hematoma evacuation with or without decompressive craniectomy have yielded different conclusions, possibly due to differences in surgical methods. Retrospective studies have found that patients with large basal ganglia hemorrhages (hematoma volume > 40ml) who underwent combined decompressive craniectomy and ultrasound-guided minimally invasive puncture aspiration followed by hematoma cavity drainage had lower intracranial pressure, less edema around the hematoma, faster edema resolution, shorter hospital stays, lower one-year mortality rates, and better functional prognosis at 6 months compared to those who underwent decompressive craniectomy alone. This combined surgical approach may require further studies in moribund patients.
Minimally Invasive Surgical Methods vs. Conservative Treatment
Various minimally invasive surgical techniques have been compared to conservative treatment, including hematoma cavity drainage tube placement, endoscopic hematoma evacuation, and microsurgical techniques using endoscopy. As previously mentioned, the large randomized controlled trial MISTIE III found that stereotactic, thrombolysis-assisted hematoma cavity drainage could improve mortality but did not find benefits in functional prognosis. A single-center randomized controlled trial comparing similar MISTIE surgical methods to conservative treatment for smaller basal ganglia hemorrhages (15-30 mL) found that patients undergoing minimally invasive surgery had improved NIHSS scores at 3, 7, and 30 days post-operation. A retrospective study on stereotactic hematoma puncture showed that in patients with supratentorial midline shift intracerebral hemorrhage, using a syringe to administer thrombolytics and aspirate the hematoma after establishing a hematoma cavity could improve mortality at 30 days, but did not improve functional prognosis.
Regarding endoscopic treatment techniques, a single-center retrospective comparison study showed that the mortality rate after endoscopic hematoma evacuation was significantly lower than the predicted mortality rate based on ICH scores, although the conclusions had significant benefits, the ICH scores are known to overestimate mortality, raising questions about the true value of positive conclusions. In another article by the same authors, the presence of intraventricular hemorrhage was associated with poorer prognosis, while lobar hemorrhage (compared to basal ganglia) was associated with better prognosis. A propensity-matched analysis from different medical institutions involving 224 patients with only basal ganglia hemorrhage showed that endoscopic hematoma evacuation reduced in-hospital mortality compared to conservative treatment but did not improve 3 month functional outcomes. Whether endoscopic hematoma evacuation can improve prognosis in basal ganglia hemorrhage remains unproven. Several clinical trials on endoscopic hematoma evacuation for basal ganglia hemorrhage are underway (DIST NCT05460793, EMINENT-ICH NCT05681988, NESICH NCT05539859).
Minimally invasive surgery via the parenchymal approach (MIPS) accesses the brain through a small bone window and enters the hematoma via the parenchymal approach, providing a route for hematoma evacuation between the white matter tracts and most subcortical lesions (Figure 2). In several small non-randomized controlled studies, MIPS has shown superior efficacy compared to conservative treatment, including one study primarily involving deep hematomas. A secondary analysis of this study found that using diffusion tensor imaging (DTI) for route design yielded better prognosis than route design inferred from CT scans for patients with predominantly deep hematomas.
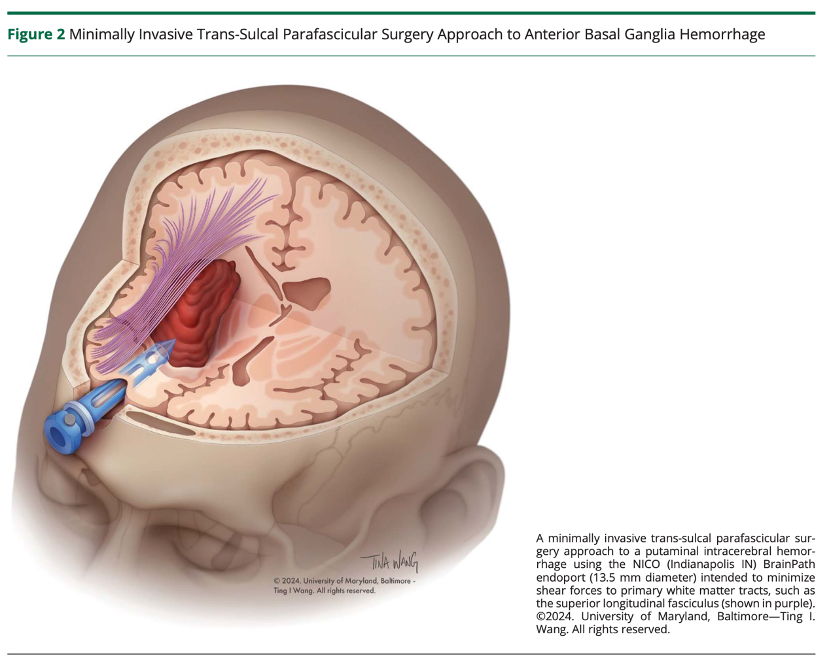
Figure 2Minimally Invasive Surgery for Basal Ganglia Hemorrhage
Using NICO (Indianapolis, Indiana) BrainPath endoport (diameter 13.5 mm) minimally invasive surgery via the parenchymal approach for treating intracerebral hemorrhage aims to minimize shear injury to primary white matter tracts, such as the superior longitudinal fasciculus (shown in purple).
The early minimally invasive hematoma evacuation trial (ENRICH) is the first multicenter randomized controlled trial of MIPS and the first multicenter randomized controlled trial with positive conclusions for surgical treatment of intracerebral hemorrhage. Patients enrolled had hematoma volumes of 30-80mL. In the ENRICH trial, compared to conservative treatment, MIPS improved the 180 day weighted modified Rankin score, with a Bayesian posterior probability of advantage of 0.981; however, its benefits were limited to patients with lobar hemorrhage. The trial adopted an adaptive design, leading to early termination of enrollment for basal ganglia hemorrhage patients, with a relatively high proportion of lobar hemorrhage patients (MIPS group accounted for 69%). The trial excluded patients with significant intraventricular hemorrhage and thalamic and subtentorial hemorrhage. The average hematoma volume was about 51mL, and the average residual hematoma volume at treatment completion for MIPS was 14.9 mL, with approximately 73% of patients achieving the target residual hematoma volume of ≤15mL. In addition to improving functional prognosis, patients undergoing MIPS had a lower proportion of those undergoing decompressive craniectomy, shorter ICU stay, reduced length of hospitalization, and lower mortality rates at 30 days. At 6 months, 50% of MIPS patients and 41% of conservative treatment patients had mRS scores of 0-3. The number needed to treat to prevent a 3-6 point increase in mRS score was 8.
The treatment effect of MIPS on patients with basal ganglia hemorrhage is evolving towards harm, raising the question of whether basal ganglia hemorrhages of 30-80mL have too great a mass effect to benefit from any type of surgery. The authors of ENRICH did not report the hematoma volume or residual hematoma volume after evacuation for basal ganglia hemorrhage separately. A meta-analysis prior to the publication of the ENRICH trial supported the superiority of minimally invasive surgery over conservative treatment in terms of good functional prognosis and mortality, but could not provide subgroup analyses regarding the site of hemorrhage. Several ongoing clinical trials include patients with basal ganglia hemorrhage, but differ from the ENRICH trial by allowing smaller hematoma volumes (HEALME NCT 05138341, MIND NCT03342664), using endoscopic techniques (NET-OCEAN NCT04957849), early hematoma clearance (EVACUATE NCT04434807), or a combination of several of the aforementioned features (DIST, EMINENT-ICH, NESICH).
Comparison of Various MIS Techniques
There are few direct comparisons of MIS techniques. A propensity-matched analysis of 343 patients undergoing catheter drainage compared to 212 patients undergoing endoscopic hematoma evacuation found significantly better functional prognosis and lower mortality rates in the endoscopic hematoma evacuation group. A network meta-analysis comparing endoscopic surgery with MIPS found no differences in mortality or functional prognosis, although advanced analyses using P scores suggested that endoscopic surgery may be superior. Future studies should evaluate the optimal minimally invasive surgical techniques based on specific hemorrhage presentations.
Several other issues remain regarding the surgical management of intracerebral hemorrhage, including techniques, timing, patient selection, adjunctive therapies, and issues of equitable access.
Unanswered Questions
Surgical Planning/Navigation
Technological advances hold promise for improving hematoma clearance rates and reducing iatrogenic injury. Accurate hematoma localization and navigation are critical for the success of minimally invasive surgical techniques compared to traditional craniotomy, whose main advantage is minimizing damage to normal tissue. In the MISTIE III study, improper catheter placement led to failure to achieve established surgical goals. Errors in patient positioning are often the culprit. Advances in neurosurgical navigation systems, including laser localization and augmented reality-based visualization systems, can more precisely locate smaller hematomas while reducing tissue damage.
The principal investigator of MIPS initially advocated for preoperative white matter tract imaging to guide surgical access. The effectiveness of using DTI sequences for white matter tract imaging with magnetic resonance imaging remains uncertain. In a retrospective study comparing 69 cases of DTI-guided endoscopic hematoma evacuation with 191 standard endoscopic hematoma evacuations, the study found that DTI guidance was an independent predictor of good prognosis in logistic regression analysis. The authors of ENRICH did not report the rate of DTI guidance. The importance of white matter fiber tract imaging deserves further investigation, particularly for patients with deep intracerebral hemorrhage.
Robotic-assisted surgical techniques have been explored to reduce iatrogenic tissue damage. Preliminary literature suggests that robotic surgeries result in shorter operative times and reduced postoperative inflammation compared to non-robotic-assisted hematoma puncture or endoscopy, but the best navigation system for maximizing hematoma clearance while minimizing tissue damage remains uncertain.
Promoting Hematoma Drainage
Administering thrombolytics in minimally invasive drainage aids in hematoma clearance. Irregular hematoma shapes hinder effective hematoma drainage. The rtPA used in the MISTIE III trial is limited by its short half-life, requiring multiple doses, which is often futile. Additionally, experimental evidence suggests that rtPA has harmful effects in terms of NMDA receptor-mediated neurotoxicity. A variant of rtPA called “modified tPA” has been carefully designed to prevent its interaction with NMDA receptors and extend its action time, thereby improving thrombolytic effects, and researchers are considering using modified tPA in place of rtPA for minimally invasive hematoma drainage to improve prognosis for patients in MISTIE III.
Several measures have been undertaken to improve hematoma drainage post-endoscopy. Hematoma suction devices assisted by neuroendoscopic working channels include sharp concave blades that can safely fragment blood clots without causing bleeding. Tissue liquefaction techniques relying on focused ultrasound to liquefy hematomas are also under further investigation. Numerous questions remain unanswered regarding the optimal methods for promoting hematoma clearance.
Intraoperative Assessment
Given the importance of achieving a postoperative residual hematoma of ≤15m for patients, various methods have been explored to assess the extent of hematoma clearance. In one technical approach, after sufficient blood clot suctioning and observing the hematoma cavity wall, maximum flushing is performed to improve visibility while checking for active bleeding on the cavity wall, and cauterization is performed as needed to stop bleeding. Intraoperative CT and ultrasound are then used to evaluate the extent of hematoma clearance before closure. For unacceptably high residual hematomas, intraoperative assessments appear to be more reliable than postoperative imaging, though this hypothesis remains untested.
In addition to measuring residual hematoma volume, intraoperative assessments have other objectives. An innovative ultrasound technique capable of detecting low-flow vascular structures not detected by CT angiography, known as super-microvascular imaging, may help reduce bleeding caused during surgery, and super-microvascular imaging can be used through endoscope-sized keyhole craniotomies. Intraoperative use of fluorescent dyes for angiography has also been suggested as a method for visualizing and localizing bleeding points during endoscopy and stopping the bleeding.
Timing of Surgery
The optimal timing for surgical clearance of intracerebral hemorrhage remains controversial. Past views suggested that to establish stable hematomas, reduce postoperative bleeding, and promote hematoma clearance during thrombus liquefaction, surgical treatment is often delayed. However, ideal surgery should avoid hematoma expansion, optimize hematoma clearance rates, minimize postoperative rebleeding, reduce damage to surrounding tissues (especially critical white matter tracts), and minimize inflammatory responses following red blood cell lysis.
As previously mentioned, the MISTIE III study has been criticized for its prolonged timing of treatment, aimed at ensuring hematoma stability before administering thrombolytics. On the other hand, early surgery within 4 hours of symptom onset for routine craniotomy has been halted due to increased mortality associated with rebleeding. A 2020 meta-analysis (including routine craniotomy and minimally invasive treatment) found that only early surgical treatment after symptom onset improved outcomes for supratentorial hemorrhage compared to medical treatment. In a combined post hoc analysis of STICH I and II and MISTIE III studies, good functional prognosis adjusted probabilities increased with shorter timeframes within the first 62 hours post-symptom onset for patients in STICH I and II. The timing of surgery was not related to outcomes in the MISTIE III cohort, indicating that the surgical approach determined the impact of timing on outcomes. The prohibition of ultra-early surgery in the MISTIE III study protocol prevented researchers from benefiting from the potential advantages of earlier surgery. In the ENRICH trial, the median time from known functional integrity to surgical treatment was 16.75 hours; only 5 patients (3.3%) experienced rebleeding associated with neurological deterioration post-surgery. Early MIPS appears safe, but the study did not achieve sufficient power to assess the impact of surgical timing on outcomes.
Retrospective studies of early endoscopic surgery (within 6-8 hours of symptom onset) have demonstrated safety and suggested improved outcomes. Unlike passive drainage techniques, endoscopic or small bone window microsurgical techniques allow surgeons to actively search for active bleeding points and apply hemostatic techniques to reduce hematoma expansion. In this way, the spotting sign observed on CT angiography, believed to represent the active extravasation of contrast agent into the hematoma, provides both motivation for early surgery and surgical targets, rather than contraindications for surgical intervention.
The Dutch intracerebral hemorrhage surgical study is a prospective non-randomized trial that performed supratentorial hematoma surgery within 8 hours of symptom onset for patients with hematoma volumes ≥10 mL and NIHSS≥2, finding that the surgery was safe and feasible. The median hematoma volume decreased from 47.7mL before surgery to 10.5mL after surgery, and the spotting sign (present in 12/40 patients) was not associated with postoperative rebleeding. In comparison, a retrospective study from a single center found that patients who underwent endoscopic hematoma evacuation with spotting signs within 6-8 hours of onset had a significantly higher likelihood of postoperative rebleeding and poorer outcomes than those without spotting signs. Completed but unpublished single-arm INVEST study (NCT02654015) and randomized controlled MIND study excluded patients with spotting signs from minimally invasive surgery studies, while the randomized controlled EVACUATE study did not. The EVACUATE study will assess ultra-early MIPS techniques (within 8 hours of onset), while the DIST and HEALME studies will assess ultra-early endoscopic hematoma evacuation surgical methods, all compared to conservative treatment.
Other Sites of Intracerebral Hemorrhage
ICH surgical management studies mainly focus on lobar and basal ganglia hemorrhages. There is a general consensus that cerebellar hemorrhage requires surgical intervention when hematoma volume exceeds 15mL or when there is neurological deterioration, brainstem compression, or hydrocephalus. The efficacy of minimally invasive surgery for cerebellar hemorrhage remains uncertain. Retrospective reviews suggest that endoscopic techniques have excellent hematoma clearance rates and outperform traditional surgery in terms of intraoperative bleeding and length of hospital stay, although some patients undergoing endoscopic surgery may still require decompressive craniectomy to relieve the mass effect of surrounding edema. Direct comparative studies of hematoma cavity puncture and endoscopic cerebellar hematoma drainage have shown that after adjusting for other variables, endoscopic surgery has mortality benefits. The optimal surgical technique for cerebellar hemorrhage remains uncertain.
Thalamic hemorrhage has been excluded from large randomized controlled trials of minimally invasive surgery, such as the MISTIE research (thalamic hemorrhage was excluded from the MISTIE III study) or the ENRICH study. A retrospective study of 21 patients with thalamic hemorrhage (average volume about 40 mL) treated with endoscopic SCUBA technique showed a very high hematoma clearance rate (91.4%). Two patients died at 1 month, and all other patients were unable to live independently, but at 6 months, 4 patients improved to being able to walk independently. Robotic-assisted stereotactic surgery has been evaluated for hematoma evacuation surgery in small volume thalamic hemorrhages. A retrospective study comparing 35 robotic surgeries of 5-15mL thalamic hemorrhages with 49 control patients found no improvement in neurological examination, functional prognosis, or mortality at 3 months for the surgical group. Due to the deeper location of the hemorrhage and proximity to the corticospinal tracts, increased guidance precision may be needed, which can be achieved through robotic surgical techniques.
Research on surgical treatment for primary brainstem hemorrhage is relatively scarce. In an unadjusted retrospective comparison, patients with primary brainstem hemorrhage (mainly pons hemorrhage) undergoing conventional surgical hematoma evacuation were compared to 240 patients receiving medical treatment, showing significantly lower mortality rates and improved functional prognosis for surgical patients, particularly for those who underwent surgery within 6 hours of onset. A retrospective corrected analysis involving 211 patients with primary brainstem hemorrhage found that hematoma cavity puncture drainage (113 patients) was associated with survival at 30 days, but not with recovery from coma at 90 days. Robotic hematoma cavity puncture has also been reported. In an unadjusted retrospective comparison, patients with brainstem hemorrhage undergoing robotic-assisted hematoma cavity puncture had no postoperative bleeding, reduced mortality, but did not improve functional outcomes compared to those receiving conservative treatment.
Ventricular hemorrhage is typically treated with bedside placement of external ventricular drains, and several studies have evaluated direct endoscopic hematoma evacuation for primary ventricular hemorrhage. Retrospective studies show that patients undergoing endoscopic hematoma evacuation for ventricular hemorrhage have faster hematoma clearance, improved neurological function on the GCS scale, and shorter hospital stays compared to those undergoing external ventricular drainage. One study found that endoscopic hematoma evacuation combined with irrigation reduced the incidence of ventriculitis compared to external ventricular drainage alone. This finding supports the hypothesis that accelerated hematoma clearance reduces the risk of infections associated with external ventricular drainage. A retrospective review suggests that some patients with severe ventricular hemorrhage may not require external ventricular drainage or permanent ventricular-peritoneal shunting after endoscopic hematoma evacuation. Other studies could not determine the impact of this surgery on long-term shunt rates.
Patient Selection
It remains uncertain whether age will alter surgical prognosis for patients with intracerebral hemorrhage, as it does for patients with ischemic stroke. A study on decompressive craniectomy for large volume hematomas using national health data from 2000 to 2011 found no impact of age on hospital mortality or discharge destination. A retrospective study on endoscopic hematoma evacuation in elderly patients found that nearly 30% of patients aged 65-80 achieved good outcomes, while this rate was about 15% for those aged 80 and older.
A retrospective analysis of endoscopic hematoma evacuation, craniotomy, and conservative medical treatment for shell-core hemorrhage assessed discharge outcomes for patients aged 65-74 and those aged 75 and older. Compared to conservative medical treatment, patients undergoing endoscopic hematoma evacuation or craniotomy showed lower mortality rates and lower mRS scores in both age groups. In patients with ICH scores of 3, benefits were limited to the 65-74 age group, particularly for those undergoing endoscopic hematoma evacuation, indicating an interaction between age, severity of condition, and technique. Further research is needed to evaluate the specific benefits of minimally invasive surgery in elderly patients and those with pre-existing disabilities.
Adjunctive Neuroprotective Therapies
Surgical clearance of blood clots can reduce secondary injury from neurotoxic products produced by red blood cell lysis. Greater hematoma clearance rates can indeed reduce edema, but edema around the hematoma still exists. Therefore, there is interest in combining minimally invasive surgery with neuroprotective agents to reduce edema and improve prognosis. Following previous studies on the iron chelator deferoxamine in patients not receiving surgical treatment, rabbit studies suggest that adding deferoxamine in minimally invasive surgery increases tight junction proteins around the hematoma, reduces blood-brain barrier permeability, and improves neurological function. Rosiglitazone, a PPARγ agonist, inhibits the nuclear factor kappa B pathway and regulates lipid and glucose metabolism, serving as an upstream regulator of inflammatory responses. In rabbit models of intracerebral hemorrhage, adding rosiglitazone to minimally invasive surgery improved neurological function while reducing the release of excitatory glutamate in surrounding tissues, decreasing blood-brain barrier permeability, and inhibiting oxidative stress responses by increasing superoxide dismutase content and downregulating inducible nitric oxide synthase. Pioglitazone, also a PPARγ agonist, is currently being studied in humans as part of the ENRICH-Plus study (NCT05582707), comparing the prognosis of patients with basal ganglia hemorrhage receiving MIPS treatment combined with pioglitazone versus those receiving only MIPS treatment.
In addition to the aforementioned pharmacological treatments, temperature control therapy is also under investigation. A single-center randomized controlled trial compared the efficacy of hematoma puncture with and without whole-body temperature control to 34–35°C, showing improved functional prognosis for hypothermic patients at 1 year. Recently, an international expert consensus recommended using a combined local hypothermia and whole-body temperature control approach for patients undergoing minimally invasive surgery for intracerebral hemorrhage, combining endoscopic infusion of cooling fluids with a systemic temperature control strategy for 48 hours.
Equitable Access
Surgical procedures require expensive equipment and the accessibility of specialized neurosurgeons. A retrospective study in Japan found that surgeons with >20 years of experience had a lower risk of postoperative bleeding after craniotomy than those with 10 years or less of experience. In the MISTIE III trial, institutions with more senior and experienced surgeons were associated with improved surgical outcomes. If MIS becomes the standard of care, neurosurgeons will need training to widely employ these techniques, especially as emerging evidence suggests that timely hematoma clearance is increasingly important. Cadaver models have been developed for training purposes. Medical centers may need to establish minimum annual standards for the number of minimally invasive surgeries required to maintain surgical proficiency among neurosurgeons.
When local hospitals lack surgical treatment qualifications, quickly transferring patients to qualified medical centers may provide similar patient outcomes compared to direct admission. Future medical management of intracerebral hemorrhage patients may need to follow the management strategies for acute ischemic stroke patients, utilizing existing stroke care systems. However, special attention should be paid to the pathological differences between the two, as the same medical model may lead to different outcomes for the two diseases.
In resource-poor settings where transfer is not feasible, low-cost technological solutions (including new navigation systems and homemade minimally invasive solutions to promote suction, hematoma retraction, and cauterization) may make minimally invasive surgical treatment for intracerebral hemorrhage more widespread. Non-navigated manual minimally invasive surgical approaches may also be safe for experienced operators, providing a cost-effective option. Bundled medical management strategies are also recommended for hospitals in resource-poor regions.
Prognosis
Clinical variables and grading scales are unreliable for accurate prognostic assessment after intracerebral hemorrhage. In patients undergoing surgical treatment, several retrospective reviews have found that ICH scores overestimate mortality from traditional and minimally invasive surgeries for supratentorial and subtentorial hemorrhage patients. A retrospective propensity-matched analysis indicated that the benefits of life-saving traditional surgery are transient, improving 30 day mortality but not 90 day mortality. With advances in minimally invasive surgical techniques, re-evaluation of early prognostic tools will need to consider surgical indications and adjusted recovery trajectories and prognoses.
Conclusion
Based on the ENRICH trial, MIPS surgery performed within 24 hours of onset is recommended for patients with 30-80mL lobar hemorrhage, aiming to reduce the hematoma volume to <15mL in patients aged 18-80 with no significant pre-existing disabilities. More than a quarter of patients did not achieve surgical targets, leaving room for technological advancements to drive better prognoses. The SWITCH study suggests that decompressive craniectomy without hematoma evacuation may benefit patients aged 18-75 with 30-100mL basal ganglia or thalamic hemorrhages. Unresolved concerns remain regarding the timing and efficacy of minimally invasive surgery for smaller or larger hemorrhages, non-lobar sites of hemorrhage, and elderly patients or those with existing disabilities. The prognosis for intracerebral hemorrhage varies not only between supratentorial and subtentorial but also based on specific volume thresholds at particular sites. Therefore, the volume of intracerebral hemorrhage requiring surgical clearance and the determinants of surgical success may ultimately also relate to the site of hemorrhage. The optimal minimally invasive surgical techniques may similarly be determined by precise neuroanatomic locations. Health systems should begin implementing comprehensive workflows to ensure that patients most likely to benefit can access surgical opportunities equitably and timely.
Translator’s Note