This article is published in the “Modern Urology” journal, August 2025 issue, in the short articles and case reports section. Click the “Read Original” button at the end of the article to access the journal’s official website and download the PDF of this article.
Cite this article: Luo Hengyu, Liu Shengzhuo, Zheng Haizhou, Gao Cunxiang, Shen Sikuai, Zhu Yuchun, Zheng Zhong. Case Report: Contradictory Results of CXCR4 Imaging and Adrenal Vein Sampling. [J]. Modern Urology, 2025, 30(8): 723-725.
Case Report: Contradictory Results of CXCR4 Imaging and Adrenal Vein Sampling
|
Luo Hengyu1, Liu Shengzhuo2, Zheng Haizhou3, Gao Cunxiang4, Shen Sikuai2, Zhu Yuchun2, Zheng Zhong5 |
1. Department of Urology, Mianyang Traditional Chinese Medicine Hospital; 2. Department of Urology, West China Hospital, Sichuan University; 3. Department of Urology, Wuhan Pu Ren Hospital; 4. Department of Urology, Chengdu Pi Du District Traditional Chinese Medicine Hospital; 5. Department of Urology, Xichang People’s Hospital
Percutaneous adrenal vein sampling (AVS) is the gold standard for the subtype and localization diagnosis of primary aldosteronism (PA)[1], but due to its invasive nature and high technical requirements, it is not widely performed. Clinically, subtype and localization are often determined by position stimulation tests, computed tomography (CT), or magnetic resonance imaging (MRI)[2], but the consistency rate between CT/MRI and AVS diagnosis is less than 63%[3]. The 68Ga-Pentixafor positron emission tomography (PET)/CT or PET/MRI imaging targeting C-X-C motif chemokine receptor 4 (CXCR4) has gained widespread attention in recent years as a new method for subtype and localization diagnosis due to its non-invasive nature and results that are not affected by interventional technical skills, testing levels, or anatomical variations of adrenal vein blood vessels. Previous studies have shown good consistency between CXCR4 imaging and AVS diagnosis results, with no contradictions in unilateral functional localization found[4], but the authors encountered two cases at West China Hospital of Sichuan University where the CXCR4 imaging results contradicted the AVS diagnosis, which are reported as follows.
1 Case Report
Patient 1, a 65-year-old female, presented with elevated blood pressure for 14 years, hypokalemia for over 9 years, and a left adrenal mass discovered 4 years ago, seeking further treatment at West China Hospital of Sichuan University. The specific diagnosis and treatment process is shown in Figure 1, and the imaging data is shown in Figure 2A–C.
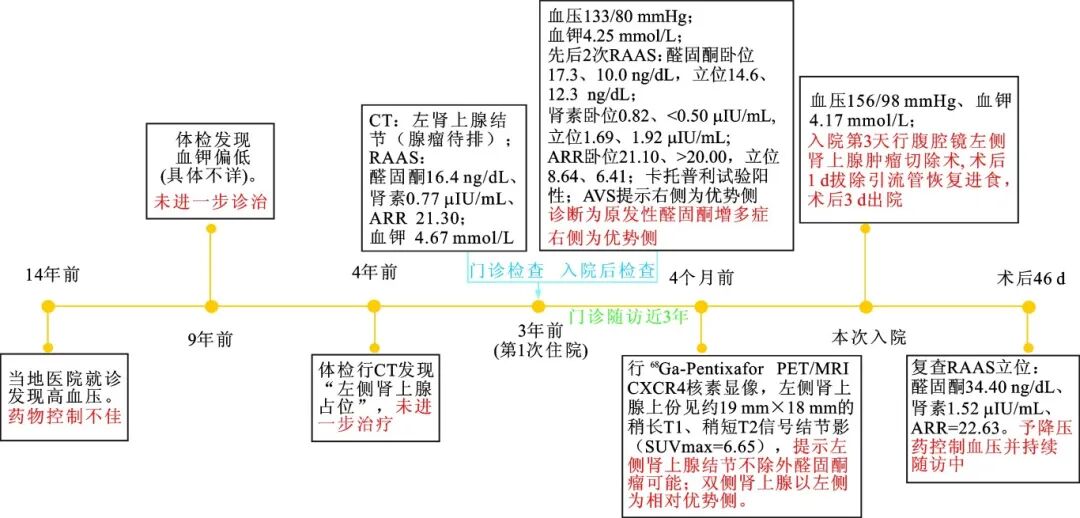
CT: computed tomography; RAAS: renin-angiotensin-aldosterone system; ARR: aldosterone to renin ratio; AVS: adrenal vein sampling; SUV: standard uptake value; 1 mmHg=0.133 kPa; PET: positron emission tomography; MRI: magnetic resonance imaging; CXCR4: C-X-C motif chemokine receptor 4.
Figure 1 Treatment process of Patient 1
Patient 2, a 51-year-old female, was admitted to West China Hospital of Sichuan University due to “elevated blood pressure for 1 year, adrenal nodule discovered 6 months ago, and fatigue for 2 months.” Patient 1 was diagnosed with hypertension at a local hospital a year ago and was treated with antihypertensive medication, controlling blood pressure at 110–130/70–90 mmHg (1 mmHg=0.133 kPa). Six months ago, a chest CT revealed a small nodule on the left adrenal gland, but no further treatment was pursued. Two months before admission, the patient experienced fatigue, and outpatient tests showed potassium levels at 3.25 mmol/L, treated with potassium chloride sustained-release tablets 3 times/d at 1 g each. Upon admission, blood pressure was 128/85 mmHg, potassium was 3.73 mmol/L, and CT indicated a lateral branch nodule on the left adrenal gland, considering the possibility of a tumor with slight calcification. Renin-angiotensin-aldosterone system (RAAS) hormone levels in supine and standing positions showed aldosterone levels of 11.40, 13.80 ng/dL, renin levels of 0.80, 1.20 μIU/mL, and aldosterone to renin ratio (ARR) of 14.25, 11.50. Pre- and post-saline load test aldosterone levels were 22.00, 16.90 ng/dL; captopril test pre- and post-medication aldosterone levels were 20.90, 24.40 ng/dL, diagnosing PA[5]. On the 9th day after admission, the patient underwent bilateral AVS via the femoral vein, indicating the right side as the dominant side.
Due to the inconsistency between the blood sampling results and the CT diagnosis, the patient underwent 68Ga-Pentixafor PET/MRI CXCR4 imaging on the 16th day of admission, indicating: an approximately 11 mm × 8 mm isointense T1, slightly hyperintense T2 signal on the lateral branch of the left adrenal gland, with increased uptake of 68Ga-Pentixafor, maximum standard uptake value (SUV) of 7.91; the maximum SUVs for normal adrenal tissue on both sides were 2.45 (right) and 2.26 (left), considering the left adrenal lateral branch nodule to be highly likely an aldosterone-producing tumor (Figure 2D–F).
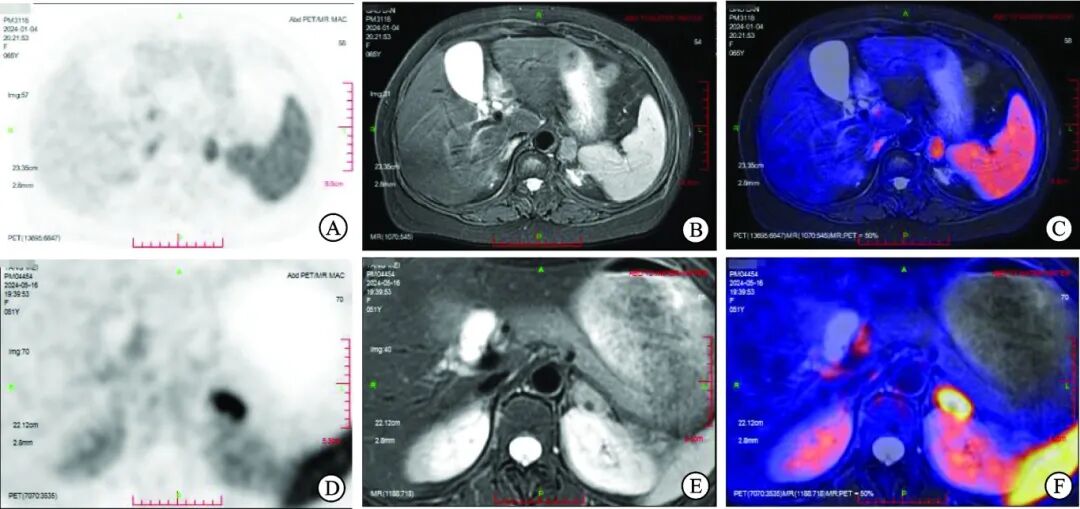
A, D: Patients 1 and 2 bilateral adrenal glands 68Ga-Pentixafor positron emission tomography (PET imaging); B, E: Patients 1 and 2 bilateral adrenal magnetic resonance imaging (MRI) T2WI imaging; C, F: Patients 1 and 2 PET and MRI fusion images.
Figure 2 Imaging of Two Patients with Primary Aldosteronism
After discussing with the patient based on consensus recommendations, a laparoscopic left adrenal tumor resection was performed on the 22nd day of admission[6]. The surgery was successful, and the patient recovered well. A follow-up 34 days post-surgery showed standing RAAS hormone levels: aldosterone 22.80 ng/dL, renin 1.59 μIU/mL, ARR 14.34. The patient’s renin level remained suppressed, and the ARR was above the cutoff value, suggesting a possible error in dominant side selection. Currently, blood pressure is controlled with medication, and the patient is under continuous follow-up.
2 Discussion
PA mainly includes aldosterone-producing adenoma (APA) and idiopathic hyperaldosteronism (IHA), which account for over 90% of PA cases[7]. Since APA can be cured by surgery, while IHA requires long-term medication, accurately distinguishing PA subtypes is crucial for treatment strategy formulation. Previously, the diagnosis of APA mainly relied on AVS; when AVS indicates a dominant side for aldosterone secretion and imaging confirms the presence of an adrenal tumor on that side, the likelihood of APA is high. However, AVS is technically challenging and costly, especially with a low success rate for catheterization of the right adrenal vein, making the search for new diagnostic methods a research hotspot. Studies have shown that CXCR4 expression is significantly elevated in APA, and its expression level is positively correlated with aldosterone synthase (cytochrome P450 family 11 subfamily B member 2, CYP11B2)[8], thus CXCR4 imaging has become a potential tool for PA subtype diagnosis. Research indicates that the sensitivity of CXCR4 imaging in diagnosing APA can reach 88%–100%, with specificity of 78.6%–100%[8-10], and good consistency with AVS diagnosis results (83.3%–90%), with no reports of contradictory unilateral functional localization with AVS results[4,10].
In contrast, the CXCR4 imaging results of 11 patients who underwent surgery concurrently with this study were consistent with the dominant side determined by AVS and the lesion side shown by CT, with good recovery of hormone levels post-surgery. However, in the two patients reported here, the AVS results indicated the dominant side was opposite to the side shown by CT, and the CXCR4 imaging results were also contrary to the AVS dominant side. After discussing with the patients, considering the potential influence of human factors on AVS and the variability of aldosterone concentrations[11], both patients chose to follow the CXCR4 imaging results for tumor resection. Short-term follow-up results showed that the RAAS of both patients remained suppressed, and the ARR was still above the diagnostic threshold, indicating a possible error in side selection.
The possible reasons for the contradictory results between CXCR4 imaging and AVS are as follows: ① PET/CT may miss small lesions[4,10]. The maximum SUV of the lesion is positively correlated with the size of the lesion[12], thus the dominant side in these two patients may have small lesions or nodular hyperplasia that CXCR4 imaging failed to detect abnormal uptake on that side. ② CXCR4 imaging reflects the degree of tissue uptake of 68Ga-Pentixafor, representing only the expression level of CXCR4 and not fully representing the aldosterone secretion function of the tissue. Studies have shown that about 90% of functional nodules exhibit high CXCR4 expression[13], meaning that about 10% of functional lesions may show low CXCR4 expression on PET/CT, potentially leading to imaging results that do not correspond to the actual site of high aldosterone secretion. ③ The consistency of CXCR4 expression levels with CYP11B2 expression is about 86.67%[12], thus about 13.33% of lesions with high CXCR4 expression may not exhibit increased aldosterone secretion, meaning that the CXCR4-positive side is not necessarily the dominant side for aldosterone secretion.
In summary, in clinical practice, the results of CXCR4 imaging should be interpreted with caution. Especially in patients where CT suggests an adenoma on one side but AVS results indicate the dominant side is the opposite, even if CXCR4 imaging suggests a high SUV for the adenoma, the AVS diagnosis conclusion should not be overturned solely based on that result. AVS should still be regarded as the gold standard for side localization diagnosis, and optimal treatment decisions should be made based on a comprehensive assessment of various examination results.
 References
References
[1] Wei Qiang, Zhu Yuchun. Functional Subtyping Diagnosis of Primary Aldosteronism: Expert Consensus on Adrenal Vein Sampling. [J]. Modern Urology, 2020, 25(3): 205-208.
[2] Li Yuanmei, Ren Yan, Chen Tao, et al. Diagnosis and Research Progress of Primary Aldosteronism. [J]. Journal of Sichuan University (Medical Edition), 2020, 51(3): 267-277, 262.
[3] KEMPERS MJ, LENDERS JW, VAN OUTHEUSDEN L. Systematic review: diagnostic procedures to differentiate unilateral from bilateral adrenal abnormality in primary aldosteronism. [J]. Ann Int Med, 2009, 151(5): 329-337.
[4] Xu Chengwei, Zhou Fulin, Huang Yong, et al. The Application Value of PET/CT in Functional Localization Diagnosis of Primary Aldosteronism. [J]. Journal of Chongqing Medical University, 2024, 49(4): 500-506.
[5] Chinese Medical Association Endocrinology Branch. Expert Consensus on Diagnosis and Treatment of Primary Aldosteronism (2020 Edition). [J]. Chinese Journal of Endocrinology and Metabolism, 2020, 36(9): 727-736.
[6] Chinese Physician Association Urology Physician Branch Adrenal Hypertension Surgical Collaboration Group, Chinese Medical Association Endocrinology Branch Adrenal Group, Chinese Medical Association Nuclear Medicine Branch PET Group. Clinical Application Expert Consensus on CXCR4 Receptor Imaging in Diagnosis of Primary Aldosteronism (2022). [J]. Xiehe Medical Journal, 2022, 13(6): 986-991.
[7] FUNDER JW, CAREY RM, MANTERO F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. [J]. J Clin Endocrinol Metab, 2016, 101(5): 1889-1916.
[8] HEINZE B, FUSS CT, MULATERO P, et al. Targeting CXCR4 (CXC chemokine receptor type 4) for molecular imaging of aldosterone-producing adenoma. [J]. Hypertension, 2018, 71(2): 317-325.
[9] DING J, ZHANG YS, WEN J, et al. Imaging CXCR4 expression in patients with suspected primary hyperaldosteronism. [J]. Eur J Nucl Med Mol Imag, 2020, 47(11): 2656-2665.
[10] HU J, XU T, SHEN H, et al. Accuracy of gallium-68 pentixafor positron emission tomography-computed tomography for subtyping diagnosis of primary aldosteronism. [J]. JAMA Netw Open, 2023, 6(2): e2255609.
[11] YOZAMP N, HUNDEMER GL, MOUSSA M, et al. Intraindividual variability of aldosterone concentrations in primary aldosteronism implications for case detection. [J]. Hypertension, 2021, 77(3): 891-899.
[12] Zheng Yanqing. Study on the Subtyping Value of 68Ga-Pentixafor PET/CT for Primary Aldosteronism. [D]. Hunan: Central South University, 2023.
[13] GAO Y, DING J, CUI Y, et al. Functional nodules in primary aldosteronism: identification of CXCR4 expression with 68Ga-pentixafor PET/CT. [J]. Eur Radiol, 2023, 33(2): 996-1003.
The only submission channel for this journalis the official website of “Modern Urology”
Website:http://jmurology.xjtu.edu.cn/
Editorial office phone: 029-82657054
Please do not trust any other websites or individuals for submissions to avoid being deceived.
Click the button below to“Read Original”to download the PDF of this article.
Editor: Zhong Jiao Jiao, Guo Chu Jun
Review: Wang Wei
Modern Urology∣ YourPartner