Click the blue text
Follow us
This
issue

Highlights
of
At the 2025 WCLC, Junshi Biosciences unveiled the groundbreaking phase I clinical data of its PD-L1 ADC (HLX43), attracting widespread attention in the industry. As the next frontier in the field of immune checkpoint inhibitors, PD-L1 ADC integrates the “dual strike” mechanism of immunotherapy and cytotoxic effects, being regarded as a new frontier in tumor treatment. At this WCLC conference, HLX43 stood out with impressive efficacy and good safety, particularly demonstrating excellent anti-tumor activity in patients with non-squamous non-small cell lung cancer (NSCLC).It is the second PD-L1 ADC (the first being Pfizer’s PD-L1 ADC (SGN-PDL1V, code PF-08046054)) to enter clinical stages globally.
This article will delve into the latest data disclosed about HLX43 at WCLC, compare it with other innovative therapies in development, and explore the rise of immune checkpoint ADCs.
Contents of this issue
|
01 |
WCLC 2025 Overview: Highlights of HLX43 Data |
|
02 |
Unique Design of HLX43 and Comparison with Competitors |
|
03 |
Overview of Competitors in EGFR Wild-Type NSCLC |
|
04 |
Summary and Outlook |
【01 WCLC 2025 Overview: Highlights of HLX43 Data】
HLX43 demonstrated a high response rate and broad-spectrum activity in patients with advanced NSCLC. As of June 28, 2025, a total of 56 advanced NSCLC patients (29 squamous and 27 non-squamous) were enrolled in the Ia/Ib phase. These patients had all failed standard therapies, with most having received platinum-based chemotherapy (96.4%) and immunotherapy (89.3%), and nearly half had undergone targeted therapy (46.4%), with a quarter having received docetaxel treatment.
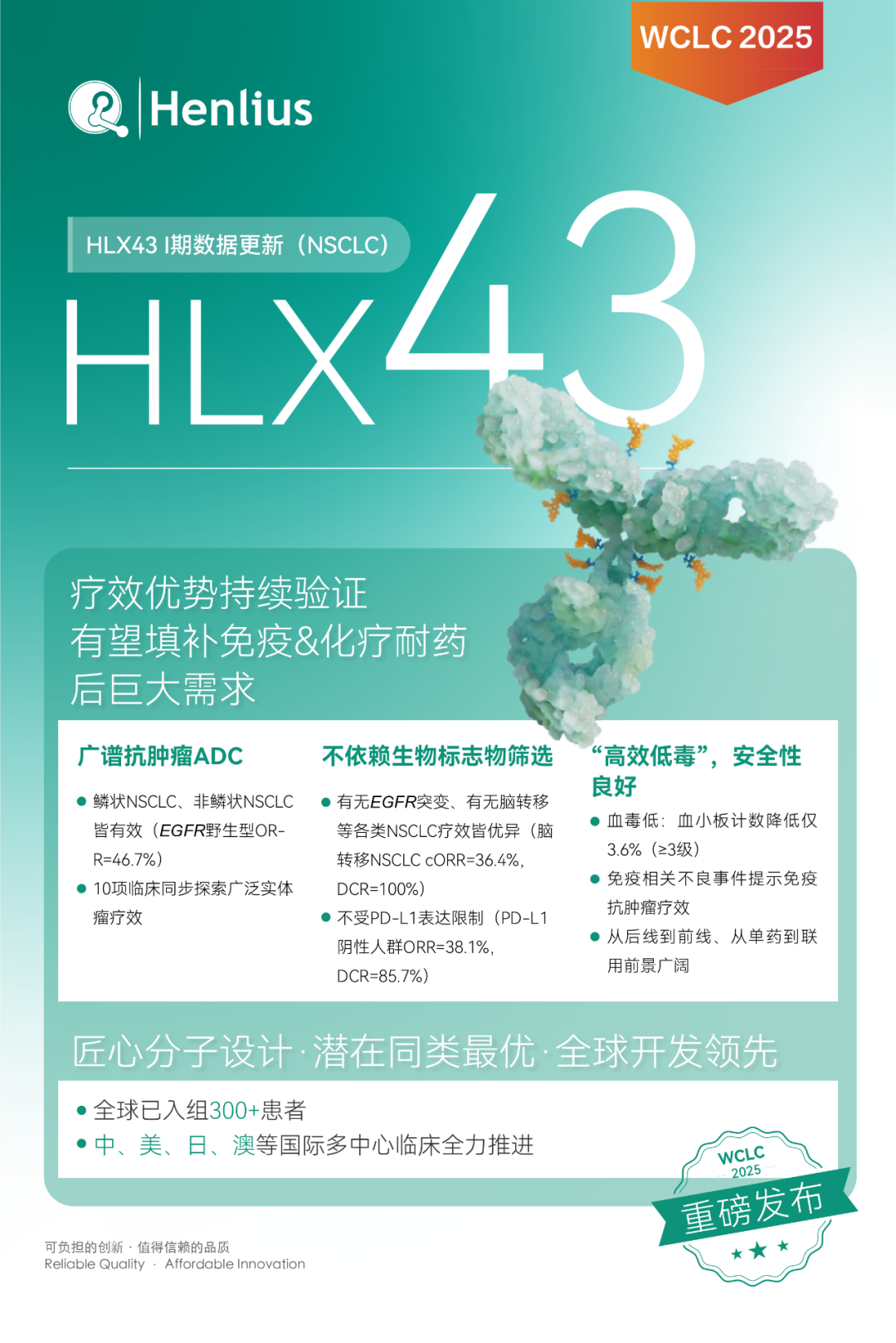
Among the 54 evaluable patients, the ORR of HLX43 monotherapy reached 37.0%, and the disease control rate (DCR) was 87.0%. This overall response level far exceeds historical data for chemotherapy in late-stage NSCLC after multiple lines of treatment (docetaxel ORR is typically less than 20%), initially demonstrating the significant advantages of ADCs over traditional therapies.
Squamous NSCLC (fourth line and above): In 28 heavily pre-treated squamous NSCLC patients, the ORR was 28.6%, and the DCR was 82.1%. Compared to the standard third-line chemotherapy docetaxel’s approximately 12.8% ORR, HLX43 more than doubled the response rate in squamous patients, showing significant clinical benefit. Notably, even in the subgroup of advanced NSCLC patients who had failed docetaxel (n=10), HLX43 treatment still achieved a 30.0% ORR and 80% DCR. This indicates that HLX43 remains effective in docetaxel-resistant patients, filling a treatment gap in this population.
Non-squamous NSCLC (third line and above): In 26 advanced non-squamous NSCLC patients (mainly lung adenocarcinoma, all EGFR wild-type or TKI-resistant cases), HLX43 achieved a 46.2% ORR, with a DCR as high as 96.2%. Almost all patients had disease control, demonstrating dominant efficacy. Particularly noteworthy is that among the 15 EGFR wild-type non-squamous NSCLC patients, the confirmed ORR reached 46.7%, and the DCR was 93.3%. This achievement sets a new record for post-line treatment of EGFR wild-type non-squamous NSCLC. It is worth mentioning that among the 5 non-squamous patients treated with HLX43 at a dose of 2.5 mg/kg, the cORR even reached 60%, further highlighting the outstanding efficacy of HLX43 in this subgroup after dose optimization.
Special subgroup efficacy: For the common population of NSCLC patients with brain metastases (n=11), HLX43 also provided significant benefits, with a confirmed ORR of 36.4% and a DCR of 100%. This suggests that HLX43 has the potential to overcome the poor prognostic factor of brain metastases, providing dual control over systemic and central nervous system. In patients with negative PD-L1 expression (TPS<1%) (n=21), HLX43’s ORR also reached 38.1%, with a DCR of 85.7%. The efficacy is almost unaffected by PD-L1 status, further confirming the “dual advantage” of PD-L1 ADCs, which can cover a broader population. Overall, whether in squamous or non-squamous, EGFR mutated or wild-type, PD-L1 high or low expression, or the presence of brain metastases, HLX43 has shown consistent preliminary efficacy, making it a broad-spectrum anti-tumor ADC.
Safety: High Efficacy with Low Toxicity
In addition to the exciting efficacy, HLX43 also performed excellently in terms of safety. 95.2% of patients experienced treatment-related adverse events (TRAEs), but these were mainly grade 1-2 routine toxicities, with a low incidence of severe adverse reactions. Notably, the hematological toxicities commonly seen with traditional ADCs, such as bone marrow suppression, were well controlled with HLX43:
Common grade ≥3 hematological toxicities included anemia (19.6%), leukopenia (19.6%), neutropenia (16.1%), and lymphopenia (12.5%), while thrombocytopenia was only 3.6%. Compared to previous chemotherapy agents, the incidence of these side effects is relatively low, validating the success of HLX43’s molecular design in reducing systemic toxicity. The TMALIN linker of HLX43 is highly stable in plasma, allowing the toxin C24 to be released and concentrated primarily in tumor tissues, thereby reducing systemic exposure and minimizing damage to normal tissues such as bone marrow.
Immune-related adverse events (irAEs): As a PD-L1 targeted drug, HLX43 retains the effect of immune checkpoint inhibition, thus immune-related toxicities were observed in some patients. A total of 12 patients (21.4%) experienced irAEs, with 8 cases (14.3%) of immune-related pneumonia (mostly grade 1-3, manageable). Interestingly, among patients with immune-related pneumonia, the objective response rate (cORR) increased to 50.0%, with a tumor shrinkage rate of 100%. This suggests that patients experiencing irAEs had better efficacy, supporting the synergistic effect of HLX43’s “tumor killing + immune activation” dual mechanism— on one hand, the cytotoxic agents released by ADC directly kill tumors, while on the other hand, the immune response triggered by PD-L1 antibodies also plays a role. This “dual approach” effect offers the potential for long-term survival benefits for patients, further distinguishing it from the toxicities exhibited by traditional chemotherapy.
Overall, HLX43 achieves a high response rate while maintaining good control over adverse reactions. The “high efficacy and low toxicity” characteristic lays the foundation for its future expansion into first-line treatment. Performing outstandingly in later-line therapies while being safe and controllable means HLX43 is expected to become a new pillar in lung cancer treatment, providing effective and tolerable treatment options for more patients.

02 Unique Design of HLX43 and Comparison with Competitors
HLX43’s achievements are attributed to its differentiated molecular design and technical platform support. In the new field of PD-L1 ADCs, there are currently very few projects in clinical development globally. HLX43 is the second PD-L1 ADC to enter phase II clinical trials, following Pfizer’s (which acquired Seagen) SGN-PDL1V (code PF-08046054). Notably, Pfizer’s PD-L1 ADC recently initiated phase III clinical trials, becoming the first of its kind to enter phase III, which further boosts industry confidence in the PD-L1 ADC field. However, from the disclosed data, HLX43 shows a trend of catching up in clinical progress speed and efficacy indicators.
Innovative TMALIN Platform: HLX43 was co-developed by Junshi Biosciences and MediLink (Yilian Bio), utilizing the latter’s proprietary “tumor microenvironment-activated linker” technology (TMALIN). The antibody component of HLX43 is derived from Junshi’s independently developed PD-L1 monoclonal antibody HLX20, while the payload is the next-generation topoisomerase I inhibitor C24. Compared to first-generation ADCs that commonly use toxins like DXd, C24 has 4-10 times higher in vitro activity but a shorter half-life in blood. Meanwhile, the TMALIN tripeptide linker ensures that the ADC is specifically cleaved only in the tumor microenvironment, allowing for high concentrations of toxins to be released at the tumor site. HLX43 has a drug-to-antibody ratio (DAR) of up to 8 (DAR≈8), significantly higher than SGN-PDL1V’s DAR=4. These designs enhance tumor-killing efficacy and strengthen the “bystander effect,” which is the ability of the toxin to penetrate adjacent tumor cells. Therefore, in solid tumors with widespread PD-L1 expression, HLX43 is expected to achieve stronger and more durable anti-tumor effects while reducing systemic toxicity.
Comparison with First-Tier Competitors: Pfizer’s SGN-PDL1V uses traditional MMAE (monomethyl auristatin E) cytotoxic payload, released through an impermeable linker, causing mitotic arrest in tumor cells. In contrast, HLX43’s topoisomerase inhibitor mechanism differs in its killing molecules and emphasizes tumor-selective release and transmembrane diffusion effects. At the 2025 ASCO conference, preliminary results of phase I clinical trials for both have been disclosed: for NSCLC patients who had received immunotherapy and progressed, HLX43 achieved a 37.5% ORR in approximately third-line patients, while SGN-PDL1V had an ORR of 32.0% in approximately second-line patients. Although this is a non-strict head-to-head data comparison, HLX43 still demonstrates a higher response rate in a more difficult-to-treat population. More importantly, HLX43 also shows significant activity in PD-L1 low-expression models (such as liver cancer), suggesting its efficacy may cover “cold tumor” patients with very low PD-L1 expression, which could be one of the challenges faced by traditional PD-L1 ADCs. Preclinical studies have also confirmed that HLX43 has strong inhibitory effects on tumor models resistant to PD-1/PD-L1 monoclonal antibodies, with anti-tumor activity significantly superior to SGN-PDL1V.
Global Development Speed: Since obtaining clinical approval in China and the US at the end of 2023, HLX43 completed phase I dose escalation and preliminary expansion in about one year, officially entering international multi-center phase II trials in the first quarter of 2025. Currently, phase II clinical trials for HLX43 have been initiated in China, the US, Japan, and Australia, with the first patient dosing successfully completed in China. In contrast, although Pfizer’s PD-L1 ADC has now initiated phase III, its early development progress has been relatively cautious. With HLX43’s “small steps, fast running” approach in launching phase II trials globally, it is expected to achieve more breakthroughs in subsequent indications, realizing a “curve overtaking” in the commercialization path. The competition between the two is not only a product rivalry but also indicates that the PD-L1 ADC category is entering an accelerated development phase, which may lead to significant multinational collaborations and transaction opportunities in the future.
【03 Overview of Competitors in EGFR Wild-Type NSCLC】
HLX43’s outstanding efficacy in EGFR wild-type NSCLC patients reignites hope in this long-standing challenging area. EGFR wild-type (i.e., not carrying sensitive EGFR mutations) lung cancer patients account for the majority of NSCLC (especially nearly all squamous and about half of lung adenocarcinoma). These patients cannot benefit from EGFR-targeted drugs, and standard treatments are often limited to chemotherapy and immunotherapy, with effective options scarce after multiple lines of treatment failure. Fortunately, a number of innovative therapies have gradually shown efficacy in this field in recent years, including ADCs, bispecific antibody-ADC fusion drugs, and cytokine fusion proteins. We will compare HLX43 with several representative therapies in development below:
Baillie Tianheng BL-B01D1 (EGFR×HER3 bispecific ADC): BL-B01D1 is a globally pioneering EGFR/HER3 bispecific antibody conjugate developed by Sichuan Baillie Tianheng and has been licensed for co-development with Bristol-Myers Squibb (BMS). In its phase I clinical trial, it explored dosing in EGFR wild-type advanced NSCLC (squamous + non-squamous) patients. The study included 62 EGFR wild-type NSCLC patients who had failed platinum-based chemotherapy and immunotherapy, achieving an ORR of 30.6% (confirmed ORR) and a DCR of 87.1%. Compared to the standard docetaxel’s approximately 16% efficacy, this result is encouraging. Interestingly, the drug showed even higher response rates in EGFR mutant NSCLC patients (phase I data ORR exceeding 60%), reflecting the dual potential of the dual-target design in both EGFR abnormal and wild-type populations. BL-B01D1 is currently advancing in multiple phase III clinical trials for lung cancer, nasopharyngeal cancer, esophageal cancer, etc., and has been included by CDE as a breakthrough therapy for PD-1/L1 resistant EGFR wild-type NSCLC. As another dark horse in the domestic ADC field, the success of BL-B01D1 also brings a new treatment approach for EGFR wild-type lung cancer.
Innovent Biologics IBI363 (PD-1/IL-2 Dual-Function Fusion Protein): IBI363 is not a traditional ADC but an innovative immunotherapy that fuses a PD-1 antibody with a modified IL-2 cytokine. It aims to simultaneously block the PD-1 pathway and activate T-cell proliferation, thereby revitalizing immune responses in “cold tumors.” In the phase Ib data presented at the 2025 ASCO conference, IBI363 showed certain efficacy and survival benefit trends in patients with advanced lung adenocarcinoma (58 cases) who were resistant to immunotherapy. Among them, the high-dose group (3 mg/kg Q3W) had a confirmed ORR of 24.0%, a disease control rate of 76.0%, a median progression-free survival (PFS) of 5.6 months, and a 12-month overall survival rate of 71.6%. Although the ORR is slightly lower than that of ADC drugs, IBI363 shows potential for extended survival, with some patients remaining stable for a year after treatment. Notably, IBI363 demonstrated better efficacy in adenocarcinoma patients with a smoking history, with an ORR increasing to 33.3% and a median PFS of 5.3 months. The characteristics of IBI363 being independent of PD-L1 expression and effective in both squamous and adenocarcinoma align with HLX43’s broad-spectrum nature. Innovent plans to initiate phase III registration studies, and IBI363 has received multiple FDA fast-track and orphan drug designations, expected to become a representative of new forms of immunotherapy.
AbbVie ABBV-400 (c-Met Targeted ADC): ABBV-400 is a next-generation c-Met targeted ADC developed by AbbVie, also known as Telisotuzumab adizutecan. The c-Met protein is often highly expressed in EGFR wild-type NSCLC (especially lung adenocarcinoma), becoming one of the important therapeutic targets after EGFR. In the phase I expanded cohort data presented at the 2024 ESMO conference, ABBV-400 showed strong activity against non-squamous, EGFR wild-type NSCLC: among 48 treated patients (using doses of 2.4 or 3.0 mg/kg Q3W), the confirmed ORR was 43.8%, and the clinical benefit rate (CBR, equivalent to DCR) reached 85.4%. The main grade 3 and above adverse reactions were anemia (25%) and neutropenia (15%), with overall good tolerability. Notably, most of the enrolled patients had high c-Met expression and were all EGFR wild-type, which differs from HLX43’s focus on the broad PD-L1 population. However, both have ORRs in the same range, and ABBV-400’s performance demonstrates the general feasibility of ADCs in EGFR wild-type lung cancer. ABBV-400 has now entered phase II trials and has received breakthrough therapy designation from the FDA, indicating its potential for accelerated approval, providing effective new drugs for c-Met positive patients.
Summary: From the above comparisons, it is evident that both the dual-targeting BL-B01D1 and the immune-activating IBI363, as well as the c-Met ADC ABBV-400, have shown certain efficacy in EGFR wild-type NSCLC. Among ADCs (HLX43, BL-B01D1, ABBV-400), the ORR generally falls within the 30-45% range, while the fusion protein IBI363 has a relatively lower ORR but offers the long-tail effect of immunotherapy. Notably, HLX43’s ORR in the EGFR wild-type non-squamous population is close to 47%, with a DCR exceeding 93%, significantly leading other therapies. Additionally, HLX43’s efficacy in PD-L1 negative patients and its coverage of previously failed multiple lines of treatment reflect its mechanistic advantages. It can be said that HLX43 represents the embryonic form of the dominance of immune checkpoint ADCs in this field, significantly raising the “ceiling” of efficacy in later-line therapies. Looking ahead, the aforementioned new therapies each have their unique characteristics and are expected to flourish in the vast and unmet market of EGFR wild-type NSCLC, providing personalized options for patients with different molecular characteristics.
04 Summary and Outlook
With the impressive data showcased at WCLC, HLX43 is highly anticipated by the industry. Some analyses suggest it has the potential to become the “best-in-class” PD-L1 ADC. Summarizing HLX43’s unique advantages: it integrates precise delivery of effective toxins with immune activation, achieving a “IO+ADC” dual mechanism in a single drug, which is rare among existing lung cancer drugs. For the large population of EGFR wild-type NSCLC patients, HLX43 has already demonstrated breakthrough efficacy in preliminary clinical trials, directly elevating the efficacy of later-line treatments to unprecedented heights. Furthermore, its independence from PD-L1 expression, enhanced efficacy at high doses, and controllable safety all indicate that HLX43 is likely to break through the limitations of existing therapies and redefine treatment paradigms.
In terms of development strategy, HLX43 is pursuing a “broad-spectrum” approach with multiple indications simultaneously. As of now, Junshi Biosciences has initiated clinical studies for HLX43 targeting various solid tumors, including lung cancer, hepatocellular carcinoma, esophageal cancer, gastric cancer, nasopharyngeal cancer, head and neck cancer, thymic carcinoma, and cervical cancer globally. This extensive layout benefits from PD-L1 being a universally high-expressed antigen in tumors, also indicating that HLX43 has the potential to become a “foundational bomb” product covering multiple tumor types. If subsequent trials continue to prove its efficacy and safety across different cancer types, HLX43 could very well grow into a blockbuster drug with annual sales in the tens of billions. Internationally, HLX43 has already received regulatory approvals in China, the US, Japan, and Australia, entering clinical stages in multiple countries, while also attracting significant interest from multinational pharmaceutical companies. It is foreseeable that once key phase II/III trials achieve success, HLX43 may become another benchmark case for Chinese biopharmaceutical companies to go global.
★
