

Transcatheter left atrial appendage closure (LAAC) is an effective measure to prevent thromboembolic events in patients with atrial fibrillation. The residual leaks at the edge of the occluder (PDL) and thrombus on the occluder surface (DRT) are key concerns and management points post-operation. Similar to LAAC, patients with cerebral aneurysms often undergo coil embolization (CE) treatment, where the edge PDL of the coils is also a major limitation. In experimental models of cerebral aneurysms, endovascular dissection (ED) can effectively eliminate the gap between the coil and the aneurysm wall, while promoting endothelialization on the coil surface.
The anatomical structure of the LAA is similar to that of aneurysms, so can we draw on the methods for managing PDL post-cerebral aneurysm embolization to address PDL post-LAAC?
Recently, the journal Heart Rhythm O2 published a review that elaborated on this issue in detail, which is worth referencing.
Application of ED in Aneurysm CE Treatment
Coil embolization is a revolutionary advancement in the treatment of cerebral aneurysms, outperforming surgical clipping; however, PDL remains a primary issue. A research team from the University of Montreal attempted to explore methods for managing PDL post-aneurysm embolization in animal models, with the following specific process: (1) Constructing an animal model: First, a saccular aneurysm (VPA) was constructed at the bifurcation of the carotid artery, which has a prominent neck that can be coiled but is prone to forming PDL; (2) Radioactive coil embolization: Radioactive coils were used for VPA embolization, yielding better results than traditional spring coils. The radioactive coils can damage the nearby vascular endothelium and accelerate the endothelialization process; (3) Mechanical ED: Mechanically damaging the local endothelium of the aneurysm (Figure 1), with effects similar to that of radioactive coil embolization; (4) Causing endothelial damage through radiofrequency ablation (RFA): The research team combined CE and RFA in aneurysm treatment, finding it could completely close the aneurysm (Figures 2-3).
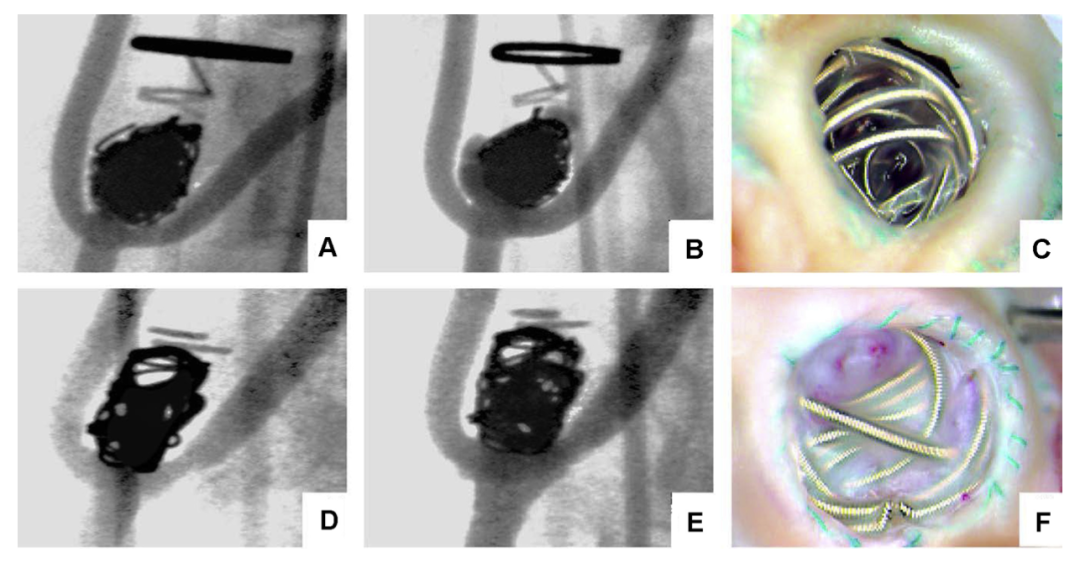
Figure 1: Angiography and visual views during the treatment of experimental pig aneurysms with coil embolization and/or mechanical ED. (A, D) are immediate angiography images after coil embolization, (B, E) are angiography images after 3 months. (A, B) without mechanical ED, (D, E) with mechanical ED. Visibly, the experimental pig undergoing mechanical ED (F) shows more complete embolization compared to those without ED (C), with more thorough endothelialization on the coil surface.
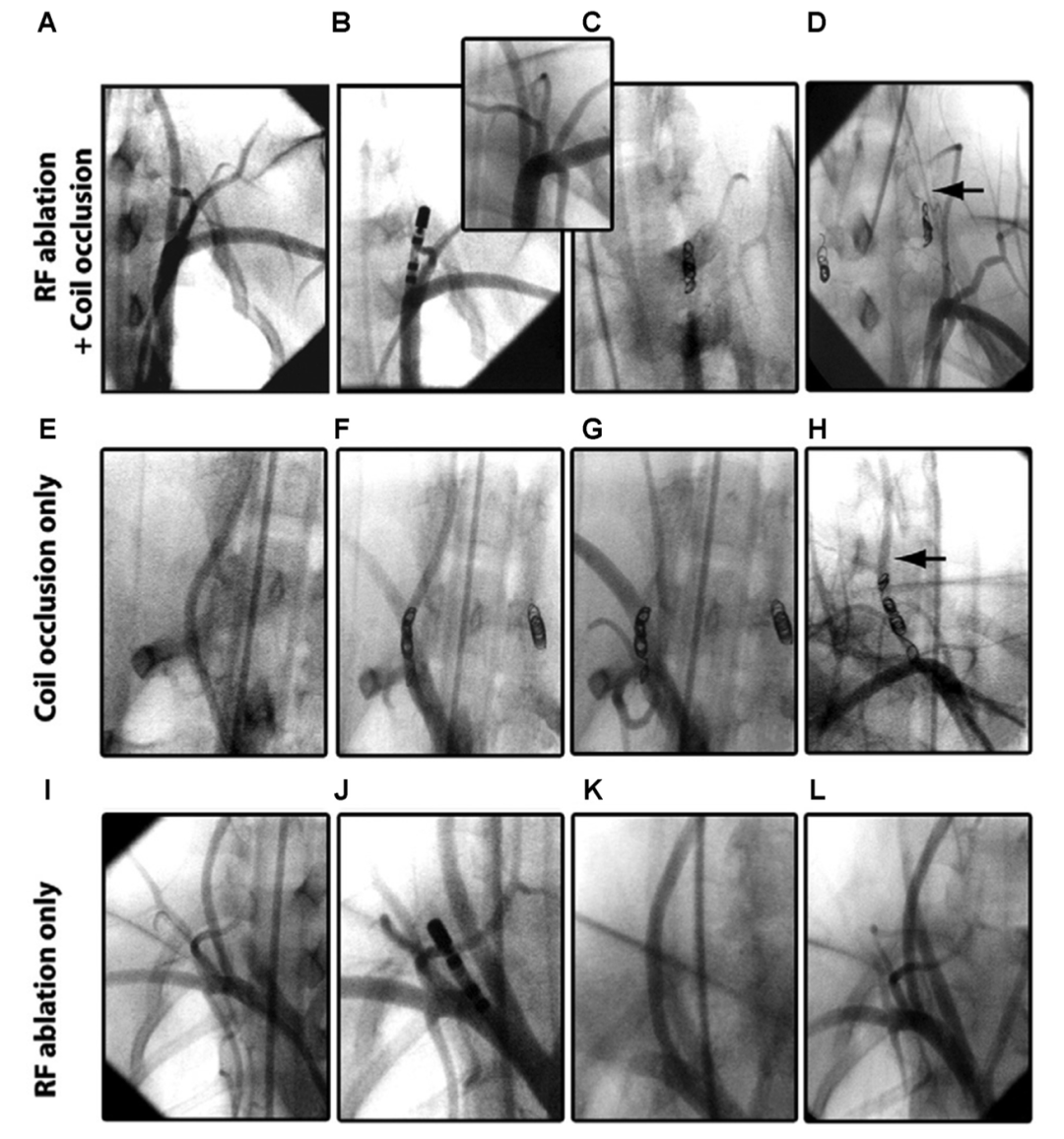
Figure 2: Angiographic results preventing re-canalization post-coil embolization of the vertebral artery in experimental pigs through RFA. (A, E, I) are pre-embolization images, (F) is immediate post-embolization, (C, G) are post-operative, (D, H) are one month post-operative. The vertebral artery undergoing simple embolization shows re-canalization (H marked with an arrow), while no re-canalization was observed in the artery undergoing RFA before embolization (B). Only performing ablation did not significantly affect the vascular angiography (J, K, L).
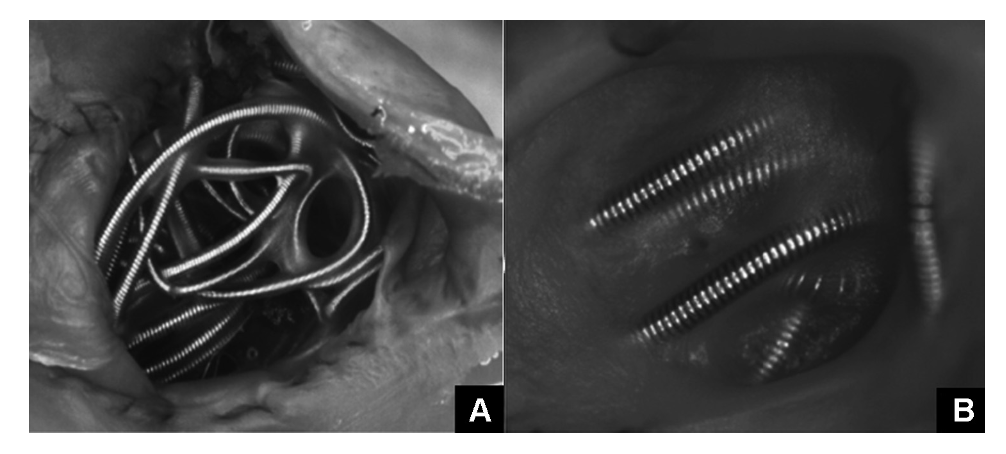
Figure 3: Visual view of the aneurysm three months post-RFA treatment after embolization. (A) only underwent coil embolization; (B) underwent RFA after embolization. It can be seen that the aneurysm undergoing RFA is completely closed, and the coil shows a faster endothelialization process.
Initial Exploration of ED in Cardiovascular Interventional Treatment
Recently, Professor Luigi’s team attempted to apply ED in the treatment of PFO for the first time. They mechanically or via RFA damaged the endothelium of the primary and secondary septum of the oval foramen. Follow-up ultrasound three months post-operation found that among the 10 patients enrolled, 9 showed spontaneous closure of PFO. This study confirmed the feasibility of ED in the field of cardiovascular interventional treatment.
Application of ED in LAAC Post-PDL Management
ED can effectively manage residual leaks post-aneurysm embolization, and can induce spontaneous closure of PFO; can it also be applied to PDL post-LAAC? A review of the literature shows that ED has already been inadvertently applied in LAAC. In some patients with long-term persistent atrial fibrillation, intervention on the LAA may be necessary during ablation, but electrical isolation of the LAA significantly increases the risk of thrombus formation; therefore, some centers perform LAAC simultaneously to prevent thromboembolic events. Panikker et al. used experimental dogs for a one-stop procedure of LAA electrical isolation + closure, finding that all LAA in 8 experimental dogs were completely closed after 45 days post-operation, suggesting that endothelial damage caused by LAA electrical isolation may help prevent the formation of post-operative PDL. Subsequent human trials confirmed this finding, with only 1 of 20 patients undergoing LAA electrical isolation + closure showing PDL.
Rocca et al. were the first to apply ED in managing PDL post-LAAC; this study included 43 patients with moderate to severe PDL (greater than 4mm) post-LAAC, applying RFA to the LAA orifice (Figure 4). The median follow-up time for transesophageal ultrasound was 48 days, revealing that 23 patients had complete closure of the LAA, and 15 had near-complete closure. Additionally, the incidence of perioperative complications was extremely low. This study confirmed that ED intervention for PDL post-LAAC is safe and effective.
Research on ED applied to aneurysm embolization found that while closing PDL, it can also accelerate the endothelialization process on the coil surface. Panikker et al. demonstrated in animal experiments that ED can promote the endothelialization of the PET covering part of the Watchman occluder surface post-LAAC, but the endothelium did not cover the central metal part of the occluder. Studies show that the exposed metal part of the occluder is associated with DRT formation. Therefore, the design of the Watchman FLX significantly reduced the area of the metal part.
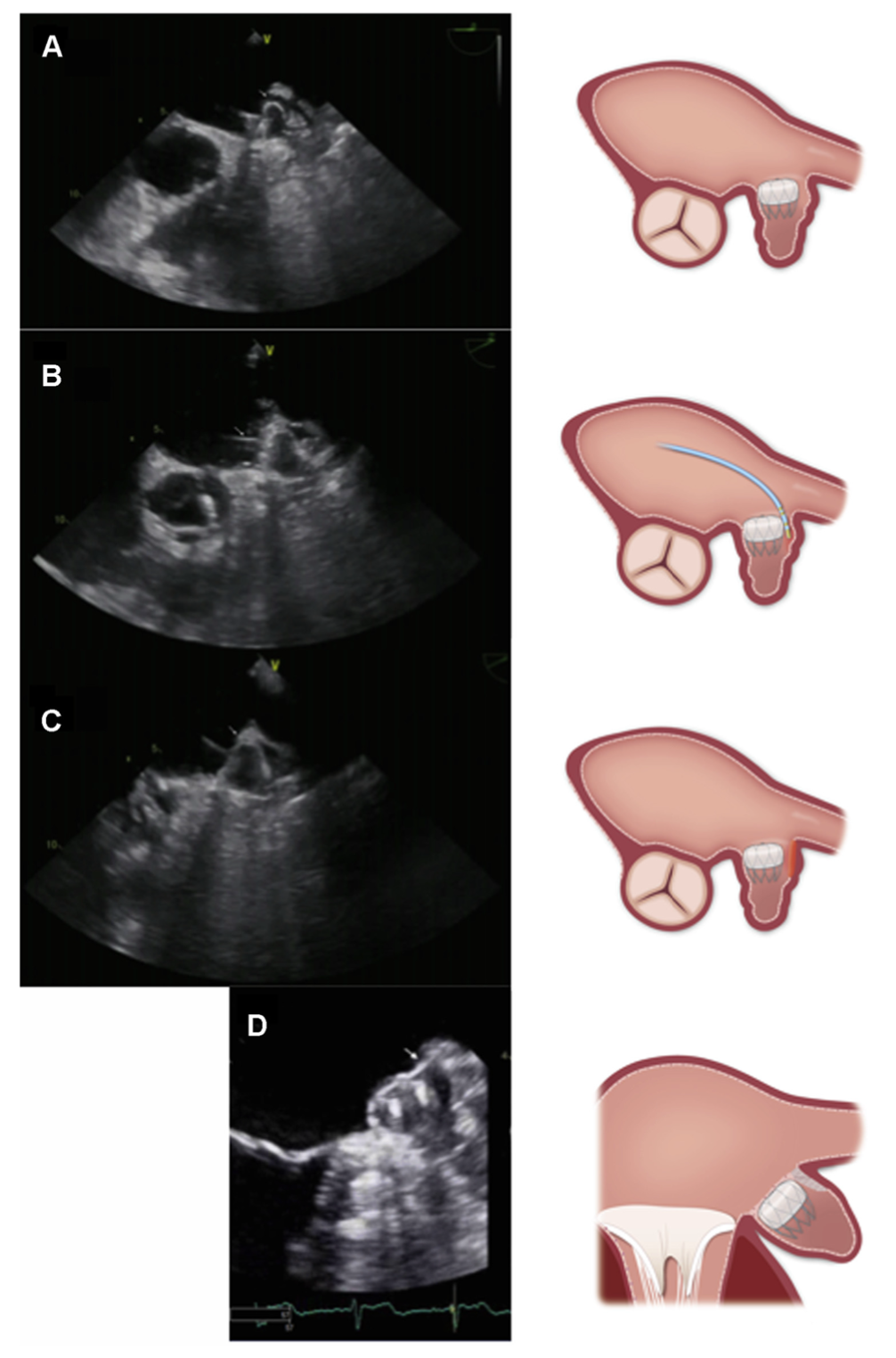
Figure 4: Example of RFA treatment for PDL post-LAAC. The patient was a 71-year-old elderly atrial fibrillation patient, who immediately showed a large PDL after implantation of a 27mm Watchman occluder (A). The ablation catheter was placed inside the PDL for ablation (B, white arrow), and after ablation, local edema was observed (C, white arrow). Follow-up ultrasound three months post-operation indicated disappearance of PDL and complete closure of the LAA (D).
Conclusion
Although animal experiments and human trials have confirmed the feasibility of ED application for PDL, they are still single-center small sample studies lacking long-term follow-up results. Furthermore, when using RFA to manage PDL, factors such as the location, range, timing, and power of ablation still require further exploration.
However, this finding undoubtedly provides a more proactive strategy for managing PDL post-LAAC, and as evidence from evidence-based medicine continues to improve, ED treatment for PDL will begin to emerge.

References
PMID: 34430948
Editor | Review: Du Xianfeng
Translation: Wang Binhao
Editor: Fang Renyuan
Previous Recommendations
Dealing with Occluder Edge Leaks: This Time We Look at Micro-Coil Embolization
Can Antidiabetic Drugs Reduce the Incidence of Atrial Fibrillation and Atrial Flutter?
How is the Left Atrial Appendage Function in Patients with Rheumatic Heart Disease?
AMULET IDE Study: A Head-to-Head RCT Study of Amulet and Watchman Occluders
Can CKD Patients Undergo Left Atrial Appendage Closure?
[Case Sharing] Bipolar Ablation of Intervals Origin Ventricular Tachycardia
Inheriting Classics · Gathering Elites | The Shuxin Sword Law 2021 was a great success again
What is the Prognosis of Left Atrial Appendage Thrombus or Spontaneous Enhancement Detected by TEE?
Is the Thickness of the Left Atrial Wall Related to Voltage Levels?
Which is Better for Improving Cognitive Function: Left Atrial Appendage Closure or Oral Anticoagulants?
Can Duration of Voltage be Used as a Measurement Indicator and Guide Ventricular Tachycardia Ablation?
Improving Neurological Symptoms After Cerebral Infarction: LAAO vs NOACs
High-Risk Atrial Fibrillation Patients: The Game Between LAAC and NOACs
Does Atrial Fibrillation Type Affect Left Atrial Appendage Closure Outcomes?
Which Low-Risk Atrial Fibrillation Patients are More Prone to Stroke?
What is the Impact of Thrombocytopenia on Left Atrial Appendage Closure?
Relationship Between Epicardial Fat Pad Thickness of the Left Atrial Posterior Wall and Recurrence After Atrial Fibrillation Ablation
Can Bivalirudin Replace Heparin During Left Atrial Appendage Closure?
Is T-Wave Inversion in COVID-19 Patients Significant?
What is the Impact of Left Atrial Appendage Closure on AF Progression? FLAAC Registry Study


