A 65-year-old male presented to the emergency department with a complaint of upper abdominal pain for 48 hours, radiating to the back. His medical history indicated a 5 cm ascendingaortic aneurysm. The patient had no previous surgical history and no significant family history. He exhibited no fever, normal blood pressure, and tachycardia. Physical examination revealed tenderness in the upper abdomen with muscle rigidity, but no rigidity or rebound tenderness. A non-contrast spiral abdominal CT scan showed a soft tissue mass just above the gastroesophageal junction, requiring differential diagnosis with a lipoma or liposarcoma (Figure 1-2). Due to the unclear diagnosis, the physician arranged for a chest MRI. The MRI revealed a large omental hernia through the esophageal hiatus (Figure 3-4), with fluid around the herniated omentum, suggesting strangulation. In the sagittal view of the MRI, the abdominal omentum was seen entering the thoracic cavity (Figure 2-4).Figure 1. Cross-sectional view showing a lipomatous mass behind the heart, with surrounding fluid consistent with strangulated lesions.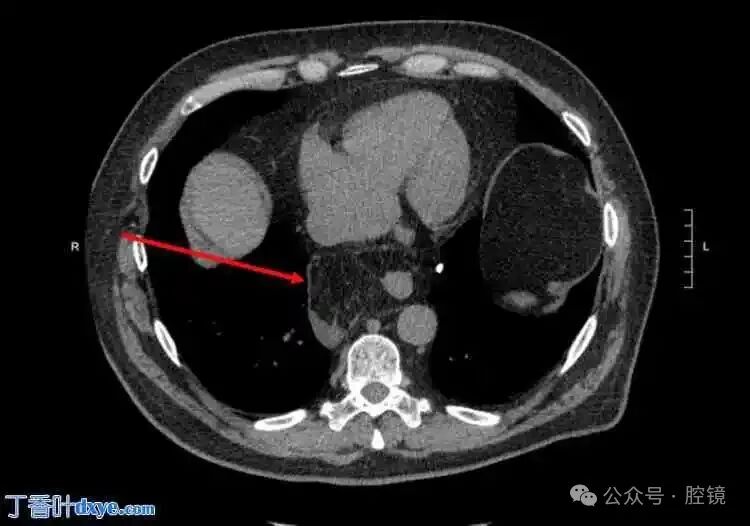 Figure 2. Sagittal view of the mass behind the heart.
Figure 2. Sagittal view of the mass behind the heart.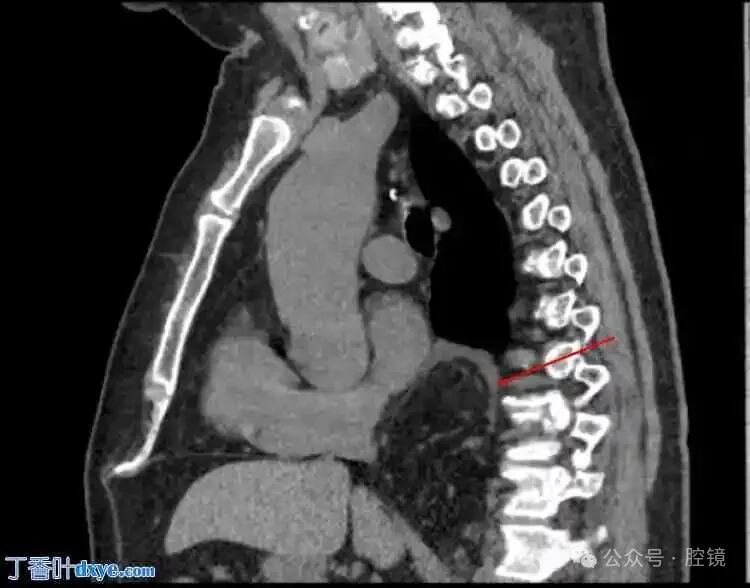 Figure 3. Cross-sectional view of the omentum in the thoracic cavity.
Figure 3. Cross-sectional view of the omentum in the thoracic cavity.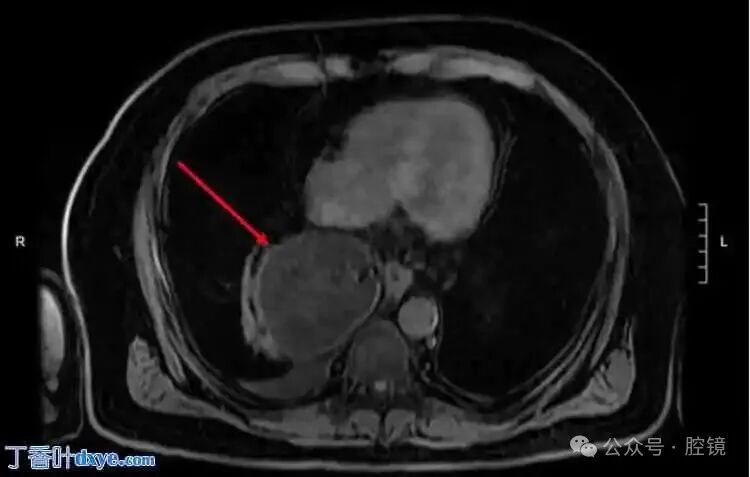 Figure 4. Sagittal view: the herniated area is located on the dorsal side of the diaphragm.
Figure 4. Sagittal view: the herniated area is located on the dorsal side of the diaphragm. At this point, the physician decided to use the Da Vinci Xi robotic system to take the patient to the operating room for robotic laparoscopic surgery. After induction of general anesthesia, the robotic cart was placed on the left side of the patient, and ports were placed in the same manner as for elective esophageal hiatal hernia repair. The author placed a camera through the suprapubic port, a Cadiere forceps through the left port, a vascular stapler through the middle right port, and an upward grasping device through the right port. In this case, the author also placed a 5 mm auxiliary port under the xiphoid to retract the liver, which is common in all of the author’s robotic repairs. Using the vascular stapler, the adhesions between the hernia sac and mediastinal structures were released, while gently reducing the herniated omentum back into the abdomen. After reduction, an omentectomy was performed on the strangulated omentum (Figure 5). The sac was excised, and the diaphragm and esophagus were separated. The defect in the esophageal hiatus was approximately 8 cm in diameter (Figure 6). Subsequently, a BIO-A biological mesh (Gore, Newark, Delaware, USA) was used to repair the esophageal hiatus. Due to the presence of necrotic omentum and the risk of possible infection, a biological mesh was utilized. The patient had a smooth recovery, was discharged on the third postoperative day, and tolerated diet without any complications.Figure 5. Reduction of the strangulated omentum from the thoracic cavity.Figure 6. Defect larger than 8 cm.Summary of training equipment (click here to view all)
At this point, the physician decided to use the Da Vinci Xi robotic system to take the patient to the operating room for robotic laparoscopic surgery. After induction of general anesthesia, the robotic cart was placed on the left side of the patient, and ports were placed in the same manner as for elective esophageal hiatal hernia repair. The author placed a camera through the suprapubic port, a Cadiere forceps through the left port, a vascular stapler through the middle right port, and an upward grasping device through the right port. In this case, the author also placed a 5 mm auxiliary port under the xiphoid to retract the liver, which is common in all of the author’s robotic repairs. Using the vascular stapler, the adhesions between the hernia sac and mediastinal structures were released, while gently reducing the herniated omentum back into the abdomen. After reduction, an omentectomy was performed on the strangulated omentum (Figure 5). The sac was excised, and the diaphragm and esophagus were separated. The defect in the esophageal hiatus was approximately 8 cm in diameter (Figure 6). Subsequently, a BIO-A biological mesh (Gore, Newark, Delaware, USA) was used to repair the esophageal hiatus. Due to the presence of necrotic omentum and the risk of possible infection, a biological mesh was utilized. The patient had a smooth recovery, was discharged on the third postoperative day, and tolerated diet without any complications.Figure 5. Reduction of the strangulated omentum from the thoracic cavity.Figure 6. Defect larger than 8 cm.Summary of training equipment (click here to view all)
For inquiries/customization, please contact:
Manager Jiang mobile 15916763572 (WeChat same number)
Click the bottom left corner “Read the original text” to view the original text/video
All sharing and opinions are for professional communication and reference only
References and images are sourced from the internet, copyright and patents belong to the original authors
For simulation training use only, not for clinical