Editor’s Note
On May 11, at the 18th Gastric Cancer Academic Conference (CGCC 2024), Professor Ying Jie’Er from Zhejiang Provincial Cancer Hospital delivered an academic report titled “Treatment of Elderly Patients with Advanced Gastric Cancer”. The content is organized as follows for readers.


1. Epidemiology and Prognosis of Elderly Patients with Advanced Gastric Cancer
According to the latest global cancer burden data (Globocan 2020), there are 1.089 million new cases of gastric cancer worldwide, ranking 5th among malignant tumors, with 768,000 deaths, ranking 3rd (Figure 1). Among these, 478,000 (43.94%) new cases and 373,000 (48.62%) deaths occurred in China, with the vast majority of patients diagnosed at an advanced stage, resulting in a poor overall survival rate of only 35.7% over five years. Currently, China has become one of the countries with the heaviest burden of gastric cancer in the world.
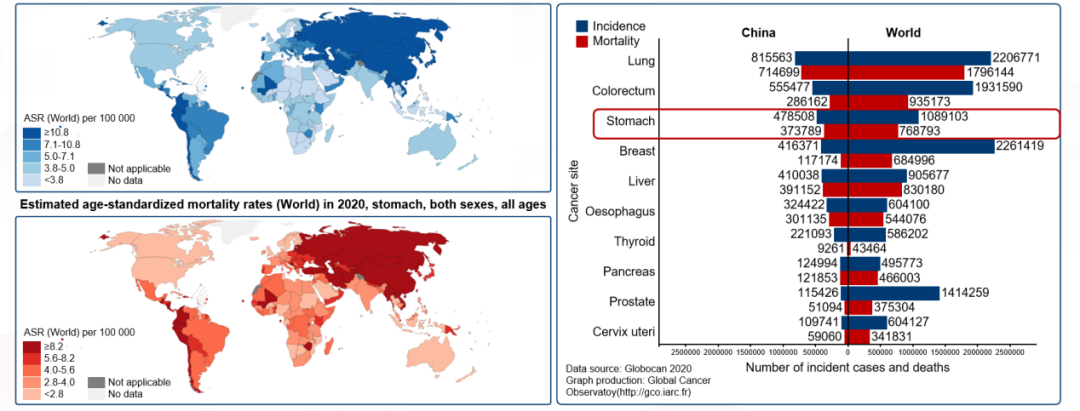
Figure 1. Globocan 2020 Data ChartDespite the trend of increasing incidence of gastric cancer in younger individuals due to the popularization of endoscopy and other technologies in recent years, “advanced age” remains a significant factor for the increased incidence of gastric cancer. Moreover, as the average lifespan of humans increases, the incidence of gastric cancer in the elderly is also rising year by year.Elderly gastric cancer patients exhibit the following characteristics due to multiple factors including decreased metabolic and immune functions: (1) Higher incidence in males, higher proportion of intestinal metaplasia in gastric mucosa, more common Lauren classification as intestinal type, and more frequent cancerous lesions in the gastric antrum.(2) Higher mutation rates in elderly gastric cancer patients. This is mainly reflected in elderly gastric cancer patients having a higher TMB level, with the mutation rates of TP53 being comparable between elderly and younger patients, while other genes show more mutations in elderly patients. (3) Differences in tumor-related gene mutation sites exist among gastric cancer patients of different ages. Elderly patients show more mutations in the ALK, FBXW7, GNA11, FGFR3, PTPN11 sites, while younger patients have more mutations in the CDH1, FGFR2, CTNNB1, ATM sites. (4) Changes in the immune microenvironment of elderly gastric cancer patients. Many studies have shown that aging affects the tumor microenvironment (TME) of normal cells, promoting tumor progression and metastasis. Fibroblasts and immune cells are particularly susceptible to age-related effects. Immune cell transformation, inflammation, and immune senescence are driving factors for age-induced tumor progression. (5) Low treatment rates among elderly gastric cancer patients. A study by Dutch scholars analyzing the treatment and prognosis of gastric cancer patients from 1989 to 2013 found that the treatment rate among elderly patients was low, with about 40% of patients not receiving treatment. (6) Poor prognosis for elderly gastric cancer patients. Statistics from Korea from 1993 to 2022 showed that as age increases, the mortality rate of cancer patients also increases (Figure 2).
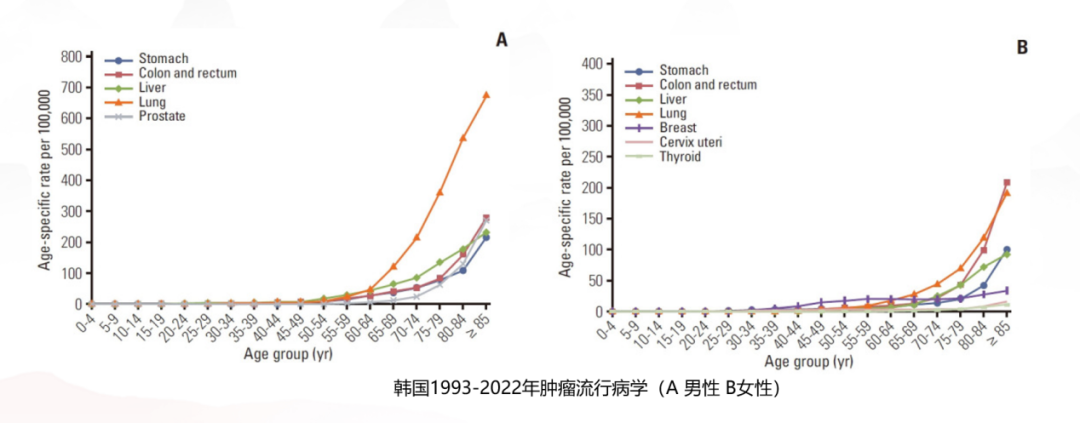
Figure 2. Cancer Epidemiology in Korea 1993-2022 (A Male B Female)
Effectiveness and Safety of Comprehensive Treatment for Elderly Patients with Advanced Gastric Cancer
The pathogenesis and physiological characteristics of elderly gastric cancer patients differ from those of younger patients, hence clinical treatment should be approached with “distinction.” Currently, both in the domestic CSCO gastric cancer diagnosis and treatment guidelines and in foreign NCCN and ESMO guidelines, chemotherapy ± immunotherapy has become the first-line standard treatment for patients with advanced gastric cancer (Figure 3). However, how effective are the various regimens in elderly patients with advanced gastric cancer, and how should clinicians make optimal choices? Researchers have conducted multiple clinical studies on this.
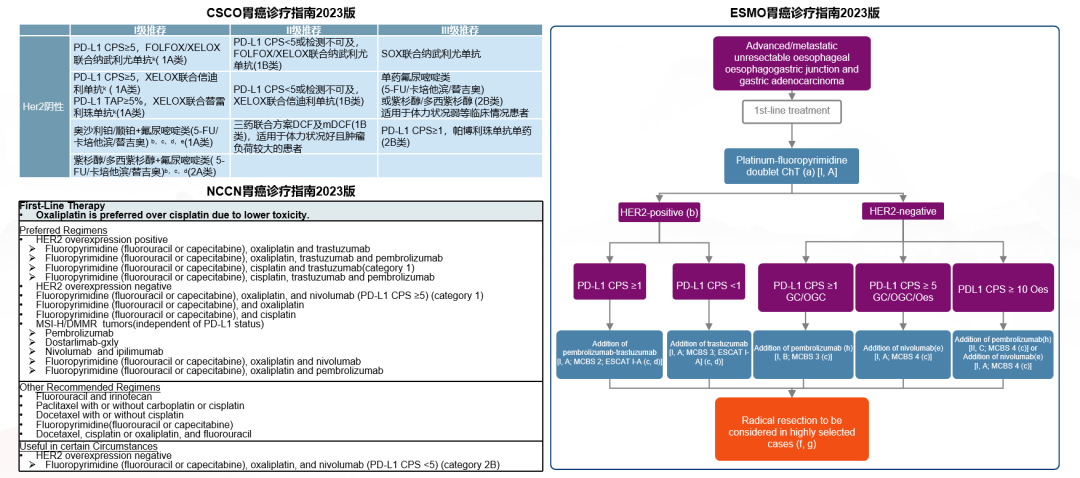
Figure 3. Recommendations from Domestic and Foreign Guidelines
01
First-Line Chemotherapy Regimen
- Capecitabine or S-1?
A randomized multicenter phase II clinical study compared the efficacy of single-agent capecitabine with single-agent S-1 in the first-line treatment of elderly patients with advanced gastric cancer. The study found that the ORR (26.1% vs. 28.9%), median PFS (4.7 vs. 4.2 months), and median OS (9.5 vs. 8.2 months) were similar in both groups. The treatment toxicities were also comparable, but the capecitabine group had a higher incidence of hand-foot syndrome. In summary, capecitabine is comparable to S-1 in terms of efficacy and safety.
- Doublet Chemotherapy or Monotherapy?
A multicenter, open-label, randomized phase III trial in Korea compared the efficacy of single-agent capecitabine with doublet chemotherapy of capecitabine combined with oxaliplatin in elderly patients with advanced gastric cancer. The results showed that elderly patients (>70 years) receiving reduced-dose doublet chemotherapy (oxaliplatin 110 mg/m² iv d1 + capecitabine 1000 mg/m² bid po d1~14, XELOX) achieved significantly better efficacy (mPFS 7.1 vs. 2.6 months, mOS 11.1 vs. 6.3 months) (Figure 4). In terms of safety, the reduced doublet regimen did not significantly increase the incidence of grade 3 or higher AEs. Furthermore, the quality of life for patients in the single-agent group was even slightly worse than that of the reduced XELOX group. Therefore, it can be concluded that reduced XELOX is more effective and has controllable safety.
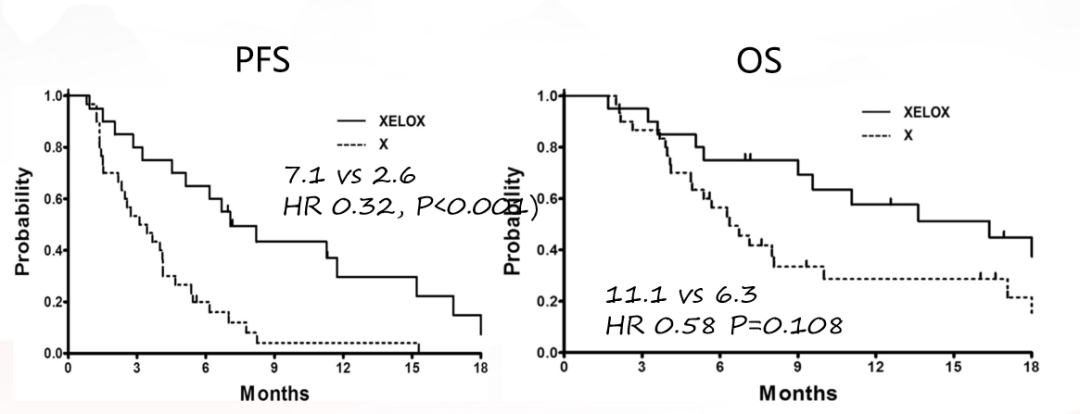
Figure 4. PFS (left), OS (right)
- Oxaliplatin or Cisplatin?
A phase III randomized controlled study compared the FLO regimen (5-FU/LV + oxaliplatin) with the FLP regimen (5-FU/LV + cisplatin) in elderly (>65 years) patients with advanced gastric cancer. The results demonstrated that the FLO group showed superior efficacy (ORR: 41.3% vs. 16.7%, P=0.012), with a longer duration of efficacy (5.4 vs. 2.3 months), and better median PFS (6.0 vs. 3.1 months), with a trend towards benefit in median OS (13.9 vs. 7.2 months) (Figure 5).
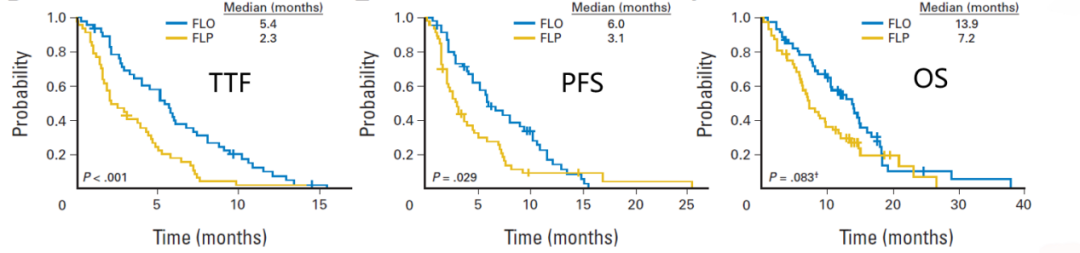
Figure 5. TTF (left), PFS (middle), OS (right)
- What is the Optimal Dose for Chemotherapy?
The GO2 study is a multicenter, non-inferiority, open-label randomized phase III clinical trial exploring the chemotherapy dosage for elderly and/or frail patients with advanced gastric cancer. Patients were randomly assigned to three dosage levels of the XELOX regimen: Level A was oxaliplatin 130 mg/m² d1 + capecitabine 625 mg/m² bid d1~21/q3w; Level B was 80% of Level A; Level C was 60% of Level A. The study endpoints were PFS and OTU (overall treatment utility, including efficacy, toxicity, quality of life, and patient acceptance).The results showed no significant differences in PFS or OS among the three dosage groups. In terms of safety and tolerability, Level C had better OTU and fewer AEs. In terms of quality of life, patients in Levels B and C both showed improvements, with Level C patients having the longest treatment duration (Figure 6).
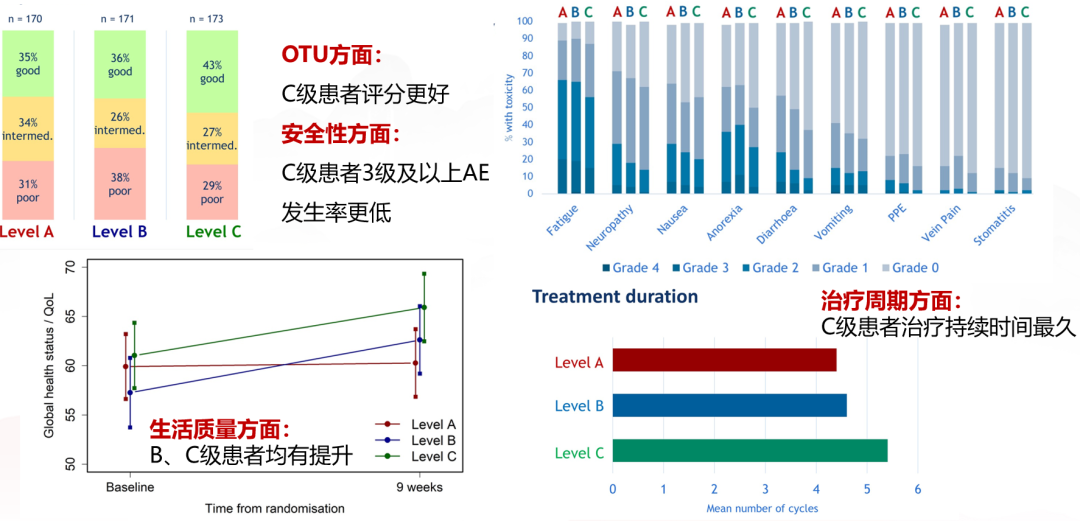
Figure 6. Safety and Tolerability of Three Dosage GroupsTherefore, the NCCN guidelines recommend that elderly patients consider reduced-dose chemotherapy, using the C-level dosage from the GO2 study. The CSCO guideline annotations also indicate that patients in the C-level dosage group not only have survival times that are not inferior to those in A and B levels but also the best patient experience.
02
First-Line Immunotherapy Combined with Chemotherapy
Although studies such as CheckMate-649, ORIENT-16, and KEYNOTE-859 have confirmed that immunotherapy combined with chemotherapy has become the new standard of first-line treatment for HER2-negative advanced gastric cancer, the benefits of using immunotherapy in elderly patients whose immunity is declining remain uncertain. In this regard, researchers have conducted further explorations.
- How Effective is Immunotherapy for Elderly Patients?
A 2019 meta-analysis of 34 clinical trials in advanced cancer, involving more than 20,000 elderly patients receiving immune checkpoint inhibitors (ICIs) as monotherapy and in combination, showed statistically significant improvements in OS for the ICI treatment group (under 65 years, 65 years and older, and under 75 years) compared to the control group, but the OS improvement for patients aged 75 and older was smaller. Studies included in the gastric cancer domain indicated that immunotherapy shows a trend of benefit regardless of the patient’s age. Additionally, analysis of treatment lines indicated that elderly patients may benefit more from first-line immunotherapy than from later lines.Several phase III gastric cancer studies (CheckMate-649, RATIONALE-305, ORIENT-16) have also suggested in subgroup analyses that age is not significantly related to the efficacy of immunotherapy, with patients aged 65 and older and those under 65 benefiting similarly from immunotherapy combined chemotherapy regimens, but optimal immunotherapy regimens for elderly gastric cancer patients still need further exploration.
- Safety of Immunotherapy
A retrospective analysis of melanoma, renal cell carcinoma, and NSCLC showed no significant differences in the occurrence of irAEs across different age groups, but endocrine toxicity was more common in patients under 65, while skin toxicity was more common in patients 75 and older. However, there is currently a lack of research exploring irAE situations in elderly gastric cancer patients.The “Expert Consensus on the Application of Immune Checkpoint Inhibitors in Special Populations” recommends that the use of ICIs in elderly patients over 75 years should be cautiously evaluated. Furthermore, due to the different spectrum of irAEs in elderly patients and the higher incidence of fatal irAEs, it is recommended to comprehensively assess the major organ functions, comorbidities, and cognitive functions before administering ICIs treatment.
03
Second-Line and Later Treatments: Targeted Therapy, Chemotherapy
Current CSCO gastric cancer guidelines recommend the following second-line and later treatments for advanced gastric cancer as shown in Figure 7. Researchers have also conducted further studies on the efficacy of the recommended regimens in elderly patients.
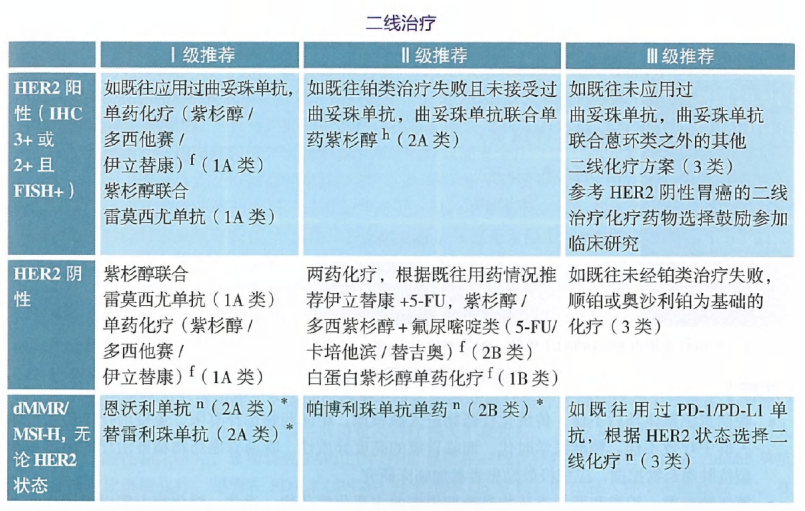
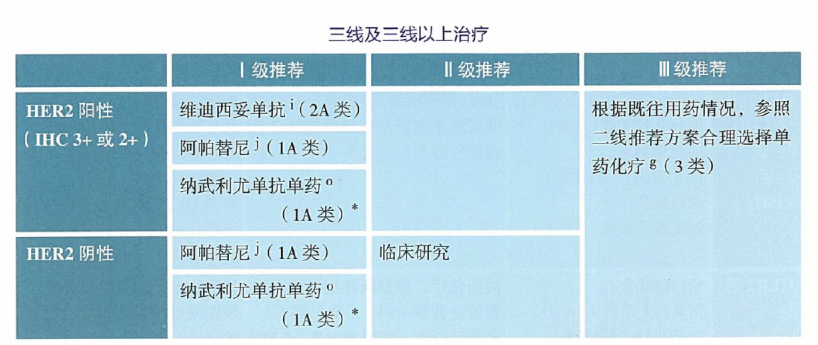
Figure 7. Recommendations for Second-Line and Later Treatments in Advanced Gastric Cancer from CSCO Guidelines
- Second-Line Chemotherapy: Paclitaxel or Irinotecan?
The WJOG 4007 study subgroup analysis suggested that for gastric cancer patients aged 65 and older, paclitaxel and irinotecan have comparable efficacy. In terms of safety, this study did not report AEs specifically for the elderly population, but the overall population analysis showed that AEs in both groups were tolerable, with no significant differences.
- What is the Optimal Dose for Targeted Therapy with Apatinib?
The AHEAD-G202 study analyzed the efficacy and safety of different doses of apatinib in gastric cancer patients aged 65 and older, finding that the low-dose group had better mPFS and mOS than the medium and high-dose groups, although it did not reach statistical significance; 11 patients (all in the medium and high-dose groups) had dose reductions due to treatment toxicity; the incidence of AEs was similar among the three dosage groups. Thus, it is evident that low-dose apatinib may bring greater benefits to elderly patients.
- How Effective is Ramucirumab Targeted Therapy in Elderly Patients?
The REGARD and RAINBOW studies retrospectively evaluated the treatment efficacy and safety of ramucirumab in advanced gastric cancer patients of different ages. The results showed similar PFS and OS in patients under 65, 65 and older, 70 and older, and 75 and older, and no significant correlation between adverse events (including grade 3 or higher AEs) and age. This confirms that the efficacy of ramucirumab is not significantly related to the age of advanced gastric cancer patients.Furthermore, for HER2-positive advanced gastric cancer patients, current guidelines recommend treatment regimens based on trastuzumab. Two phase II studies explored the efficacy and safety of trastuzumab combined with cisplatin, capecitabine, and S-1 in elderly gastric cancer patients. The results showed that all three treatment regimens demonstrated similar efficacy benefits, and patient safety was controllable.
Conclusion
Current research shows that elderly patients with advanced gastric cancer can achieve similar efficacy to non-elderly patients after receiving appropriate drug treatment. However, given the decline in organ reserve and physical condition in the elderly, clinical treatment can avoid and reduce adverse reactions by adjusting drug dosages. With the trend of global aging, more prospective studies focusing on the elderly are needed to provide more reliable evidence-based medical evidence to guide clinicians in formulating effective and safe treatment plans.
Expert Profile

Professor Ying Jie’Er
Chief Physician, Department of Gastrointestinal Oncology, Zhejiang Provincial Cancer Hospital, University of Chinese Academy of SciencesMember of the Special Committee on Targeted Therapy of the Chinese Anti-Cancer AssociationMember of the Special Committee on Colorectal Cancer of the Chinese Anti-Cancer AssociationMember of the Special Committee on Gastric Cancer of the Chinese Anti-Cancer AssociationMember of the MDT Special Committee of the Surgical Physician Branch of the Chinese Medical Doctor AssociationExecutive Committee Member of the Gastric Cancer Special Committee of CSCOExecutive Committee Member of the Cholangiocarcinoma Special Committee of CSCOMember of the Liver Cancer Special Committee of CSCOMember of the Colorectal Cancer Special Committee of CSCOChairman of the Special Committee on Tumor Metastasis of the Zhejiang Anti-Cancer AssociationVice Chairman of the Special Committee on Medical Oncology of the Zhejiang Anti-Cancer AssociationVice Chairman of the Special Committee on Tumor Nutritional Support of the Zhejiang Anti-Cancer AssociationVice Chairman of the Oncology Nutrition and Treatment Branch of the Zhejiang Medical AssociationVice Chairman of the Precision Treatment Special Committee of the Zhejiang Medical Association



References
(Swipe Up to View)[1] Data source: Globocan 2020[2] Data source: https://seer.cancer.gov/statfacts/html/stomach.html[3] Jung, Kyu-Won et al. Cancer research and treatment?vol. 56,2 (2024): 372-379. doi:10.4143/crt.2024.252[4] Changing trends of disease burden of gastric cancer in China from 1990 to 2019 and its predictions: Findings from Global Burden of Disease Study, Chinese Journal of Cancer Research, CJCR, 2021[5] Long, Li,Yin, Li,Li, Lin et al. Mutational characteristics of young and elderly gastric cancer: a comparative study.[J] .J Gastrointest Oncol, 2022, 13: 0.[7] How the ageing microenvironment influences tumour progression: Nat Rev Cancer: 2020 Feb[8] Nelen, S D et al. Gastric cancer: official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association?vol. 20,6 (2017): 919-928. doi:10.1007/s10120-017-0708-7[9] 2023 CSCO Gastric Cancer Diagnosis and Treatment Guidelines.[10] Gastric Cancer NCCN Guidelines Version 2.2023.[11] ESMO Gastric Cancer Living Guideline, v1.2 October 2023.[12] Lee, J-L et al. British journal of cancer?vol. 99,4 (2008): 584-90. doi:10.1038/sj.bjc.6604536[13] Hwang, In Gyu et al. “A multi-center, open-label, randomized phase III trial of first-line chemotherapy with capecitabine monotherapy versus capecitabine plus oxaliplatin in elderly patients with advanced gastric cancer.”?Journal of geriatric oncology?vol. 8,3 (2017): 170-175. doi:10.1016/j.jgo.2017.01.002[14] Hall, Peter S et al. “Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Quality of Life and Cancer Control Among Older and Frail Patients With Advanced Gastroesophageal Cancer: The GO2 Phase 3 Randomized Clinical Trial.”?JAMA oncology?vol. 7,6 (2021): 869-877.[15] Huang, Xuan-Zhang et al. “Efficacy of immune checkpoint inhibitors and age in cancer patients.”?Immunotherapy?vol. 12,8 (2020): 587-603.[16] Kimura, Yutaka et al. “Multicenter phase II study of trastuzumab plus S-1 alone in elderly patients with HER2-positive advanced gastric cancer (JACCRO GC-06).”?Gastric cancer: official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association?vol. 21,3 (2018): 421-427.[17] Zhu, Bo et al. “A Retrospective Comparison of Trastuzumab Plus Cisplatin and Trastuzumab Plus Capecitabine in Elderly HER2-Positive Advanced Gastric Cancer Patients.”?Medicine?vol. 94,34 (2015): e1428.
(Source: Tumor Outlook – Digestive News)
Statement
All original articles are copyright of “Tumor Outlook”. Sharing and reprinting are welcome. This article is for medical professionals to understand the latest medical information and is not representative of this platform’s views. This information cannot replace professional medical guidance in any way and should not be considered as medical advice. If this information is used for purposes other than information, the site and the author bear no related responsibility.