

Study Overview
Objective:
To investigate whether immediate complete revascularization during the first PCI is not inferior to staged multivessel PCI (19-45 days) in hemodynamically stable patients with STEMI and multivessel coronary artery disease.
Methods:
The trial included patients with acute STEMI (within 24 hours of symptom onset) and multivessel coronary artery disease, who were hemodynamically stable after successful first PCI of the infarct-related coronary artery. Patients were randomly assigned in a 1:1 ratio to receive immediate or staged (19-45 days) non-culprit vessel PCI.
Multivessel coronary artery disease was defined as having at least one coronary artery lesion with a diameter stenosis of ≥70% as shown on coronary angiography, with non-culprit coronary artery diameters of ≥2.25 mm and ≤5.75 mm.
The primary endpoint was a composite of all-cause mortality, non-fatal myocardial infarction, stroke, unplanned ischemia-driven revascularization, or hospitalization for heart failure within one year after randomization.
Results:
The trial enrolled 840 patients from 37 centers across Europe, with a mean age of 65 years, of which 21.2% were female. Among them, 418 patients underwent immediate PCI for non-culprit vessel lesions during surgery (mean age 66 years, 77% male), and 422 patients underwent staged PCI for non-culprit vessel lesions within 19-45 days after successful first PCI (mean age 64 years, 81% male).
Compared to the staged PCI group, the immediate PCI group had a lower incidence of primary endpoint events (8.5% vs 16.3%), and the estimated risk of primary endpoint events for patients in the immediate PCI group was reduced by nearly 50% after one year (HR, 0.52; 95% CI, 0.38-0.72; P non-inferiority <0.001; P superiority <0.001). The median time interval from randomization to staged surgery in the staged PCI group was 37 days (interquartile range 30-43 days).
Additionally, the observed risk reduction in the immediate PCI group compared to the staged PCI group was primarily due to a lower incidence of non-fatal myocardial infarction (2% vs 5.3%; HR, 0.36; 95% CI, 0.16-0.8) and unplanned ischemia-driven revascularization (4.1% vs 9.3%; HR, 0.42; 95% CI, 0.24-0.74).
There were no differences between the two groups in terms of all-cause mortality, stroke, and heart failure hospitalization rates at one year.
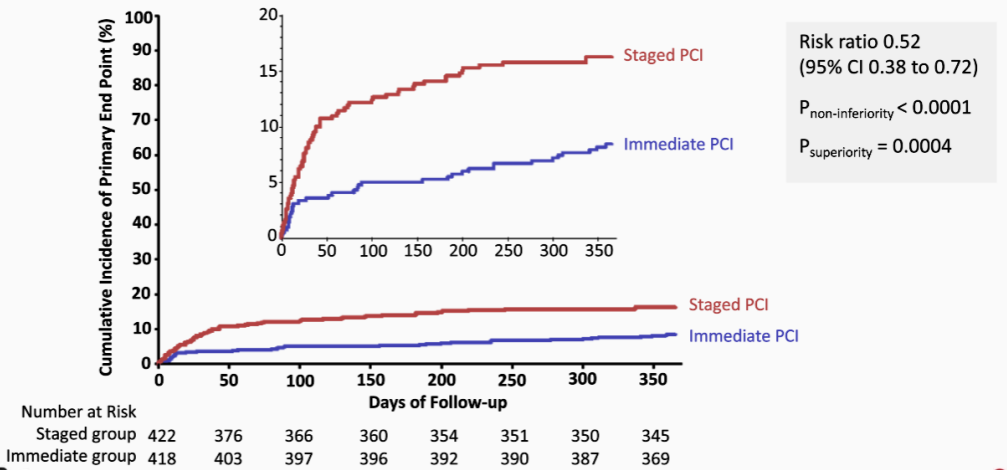
Figure 1 Primary Results
Researcher Comments
Dr. Barbara Stähli stated that the MULTISTARS-AMI trial demonstrates that, in patients with STEMI and multivessel disease, immediate multivessel PCI is not inferior to staged multivessel PCI based on the one-year composite event risk of all-cause mortality, non-fatal myocardial infarction, stroke, unplanned ischemia-driven revascularization, or hospitalization for heart failure.
The MULTISTARS AMI trial addresses the clinically important question of the optimal timing for complete revascularization in patients with STEMI and multivessel coronary artery disease. This trial shows that immediate PCI for non-culprit vessel lesions is equally effective and safe as staged PCI, which has implications for clinical practice. In pre-specified key subgroups, the results were generally consistent, particularly in women and men, younger and older patients, and those with or without diabetes.
The 2023 European Acute Coronary Syndrome (ACS) management guidelines released at this ESC Congress strongly recommend that, for hemodynamically stable STEMI patients with multivessel disease undergoing first PCI, complete revascularization should be performed (Class I A recommendation). The new ESC guidelines indicate that PCI for non-culprit lesions can be performed during the first PCI or within 45 days. Due to the lack of “adequately powered randomized trials with superiority design,” the ACS guidelines did not recommend immediate or delayed complete revascularization.
For STEMI patients with multivessel disease, MULTISTARS AMI provides partial evidence support for the optimal timing of complete revascularization, but this study is a relatively small non-inferiority trial.
Source: ESC Official Website
