Diabetes occurs due to dysfunction of pancreatic β cells and insufficient biological effects of insulin (insulin resistance), leading to increased blood sugar and decreased insulin levels.
The changes in serum insulin/C-peptide concentrations measured at fasting and 30 minutes, 1 hour, 2 hours, and 3 hours after oral glucose during an Oral Glucose Tolerance Test (OGTT) are referred to as the insulin release test/C-peptide release test.
Insulin Release Test / C-Peptide Release Test Method
(1) Discontinue any medications that may affect the test, such as contraceptives, diuretics, or phenytoin, for 3 to 7 days prior to the test.
(2) Patients should maintain a carbohydrate intake of at least 150 g daily (but not exceeding 250-300 g) and continue normal activities starting 3 days before the test.
(3) Starting between 7 and 9 AM, the patient fasts for 8 to 10 hours and then orally consumes 75 g of anhydrous glucose powder dissolved in 300 mL of warm water. If using 1 mole of glucose, it should be 82.5 g. For children, the dosage is 1.75 g per kilogram of body weight, with a maximum of 75 g.
The glucose solution should be consumed within 3 to 5 minutes. Timing begins from the first sip of glucose, and blood samples should be collected from the forearm for blood sugar, insulin/C-peptide levels before and at 0.5 h, 1 h, 2 h, and 3 h after glucose consumption.
(4) During the test, the subject should refrain from drinking tea or coffee, smoking, and vigorous exercise, but absolute bed rest is not required. Blood samples should be sent for testing as soon as possible.
(5) The test generally requires the subject’s fasting fingertip blood sugar to be less than 10 mmol/L. If fasting blood sugar exceeds 10 mmol/L, it indicates that the subject has hyperglycemic toxicity, and the data may not accurately reflect the subject’s pancreatic function.
Furthermore, high fasting blood sugar can exacerbate hyperglycemia, causing unnecessary harm to the subject.
Metabolism of Insulin and C-Peptide
Proinsulin in the rough endoplasmic reticulum of pancreatic β cells is cleaved to produce proinsulin, which is then transported to the Golgi apparatus, where it is broken down into insulin and C-peptide and stored in secretory granules. Upon stimulation, insulin and C-peptide are released in equimolar amounts into the bloodstream.
Insulin enters the liver via the portal vein, where 40% to 50% is degraded. The undegraded insulin enters systemic circulation, with a half-life of 5 to 6 minutes.
In contrast, the liver takes up very little C-peptide (< 10%), with most entering systemic circulation. C-peptide has a longer half-life (10 to 13.5 minutes), and its molar concentration in peripheral blood is 5 to 10 times that of insulin, being metabolized by the kidneys and excreted.
Currently, when clinically assessing insulin secretion capacity, both insulin and C-peptide are often measured. The metabolic pathways of insulin and C-peptide differ, allowing for their respective characteristics to be utilized.
C-peptide is not affected by insulin antibodies, proinsulin, or exogenous insulin, and it is almost not taken up and metabolized by the liver. Its half-life is more than twice that of insulin, making serum C-peptide levels a more accurate reflection of pancreatic β cell secretion function.
The area under the curve (AUC) of the C-peptide release during OGTT represents the amount of insulin secreted by β cells, while the AUC of the insulin release only represents the amount of insulin that enters systemic circulation via the liver. The difference between the two indicates the amount of insulin taken up by the liver.
Detection Methods
Methods include Radioimmunoassay (RIA), Chemiluminescent Immunoassay (CLIA), and Electrochemiluminescent Immunoassay (ECLIA).
When measuring insulin and C-peptide using RIA in clinical practice, the insulin and C-peptide measured have cross-reactivity with proinsulin, referred to as immunoreactive insulin and immunoreactive C-peptide, and do not represent the true levels of insulin and C-peptide in the blood.
Recent CLIA or ECLIA methods for measuring insulin can eliminate the interference of proinsulin, and the insulin measured is referred to as true insulin, accurately reflecting serum insulin levels and better indicating pancreatic β cell function.
However, in patients with positive insulin antibodies or those who have undergone insulin therapy, measuring C-peptide is more reliable in evaluating endogenous insulin secretion capacity.
Comparison of Insulin Release Test and C-Peptide Release Test
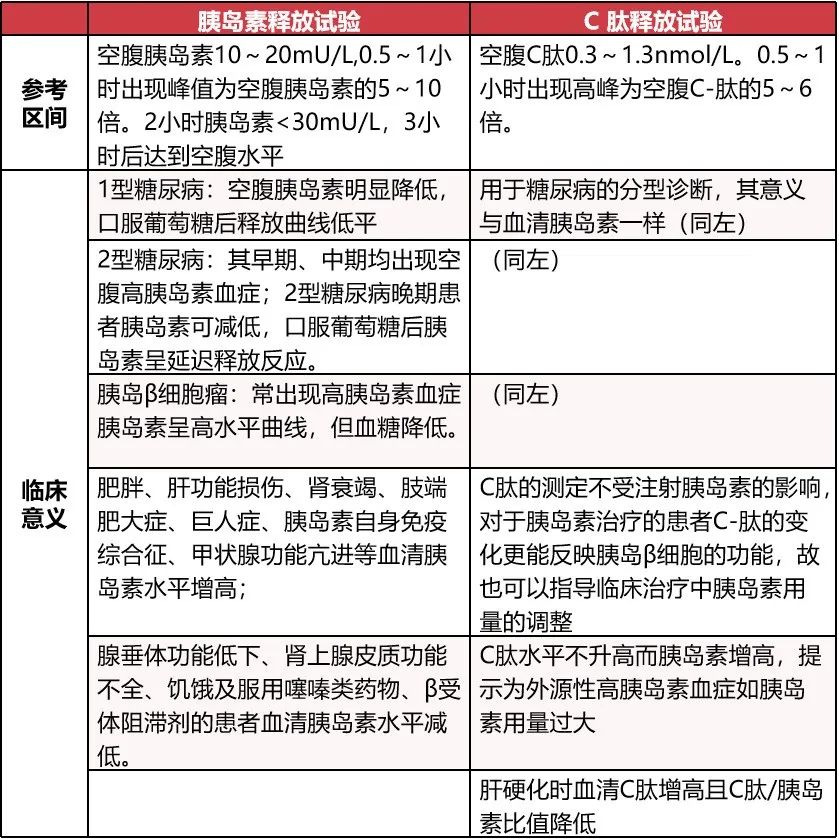
Image source: Compiled by the author
Common Diseases Associated with Abnormal Fasting Insulin and C-Peptide
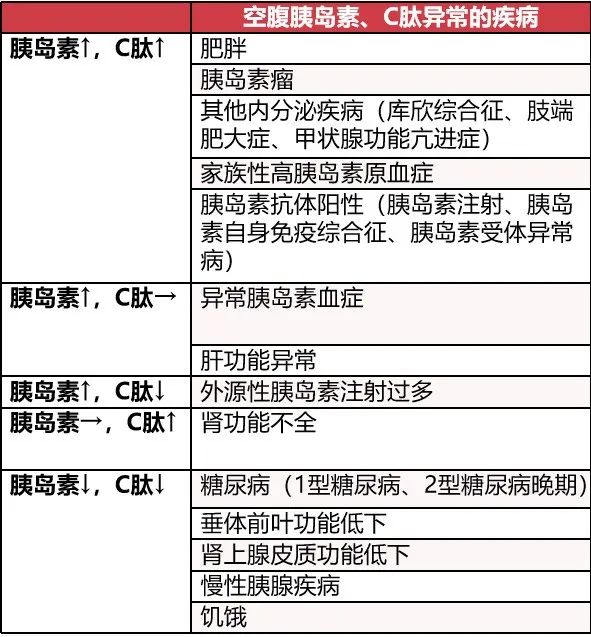
Image source: Compiled by the author
The measurement of blood insulin and C-peptide is significant for differentiating between type 1 and type 2 diabetes and guiding treatment.
C-peptide testing has more advantages than insulin: as mentioned, it is almost not taken up and metabolized by the liver, with a half-life more than twice that of insulin. Additionally, it is not affected by exogenous insulin, allowing for a more accurate reflection of pancreatic β cell function.
Moreover, C-peptide does not have immunological cross-reactivity with insulin (while proinsulin does), allowing for a more complete reflection of the secretion function of pancreatic cells.
Insulin and C-peptide levels change in parallel, but in patients who produce insulin antibodies after using exogenous insulin, insulin levels may be higher and separate from C-peptide.
If insulin and C-peptide are separated, patients who have never used insulin should be considered for insulin autoimmune syndrome. In insulin autoimmune syndrome, insulin levels can exceed 500 to 1000 mU/L.
Separate Measurement or Combined Measurement?
Insulin resistance accompanied by pancreatic β cell dysfunction is the main pathophysiological feature of type 2 diabetes. In type 2 diabetes, the insulin release curve mainly shows elevated insulin levels and delayed physiological peaks.
In clinical practice, the insulin measured during the insulin release test is actually the sum of insulin and other proinsulin cleavage products. In the pathological state of type 2 diabetes, the proportion of proinsulin cleavage products released changes disproportionately, leading to an increase in non-biologically active insulin release that is not fully processed.
Due to their similar immunological response characteristics, the insulin measured in clinical tests is the total sum of biologically active insulin, proinsulin, and other cleavage products, making it difficult to accurately reflect the functional state of pancreatic β cells.
Additionally, serum insulin levels are easily affected by the use of exogenous insulin and the presence of insulin antibodies in the body; therefore, measuring insulin release concentration alone cannot reflect the true state of pancreatic function in patients.
Since C-peptide and insulin are released from pancreatic β cells in equimolar amounts and are stored in the same secretory granules, and C-peptide is not cleared by the liver, it is more stable in the body and less affected by various factors. Therefore, it is recommended to use the C-peptide release test for a more accurate assessment of pancreatic β cell function.
Combining the C-peptide release test with the insulin release test can provide a more accurate assessment of pancreatic cell function, which is significant in newly diagnosed type 2 diabetes patients.
At the initial diagnosis of type 2 diabetes, a comprehensive analysis should be performed combining the insulin release test, C-peptide release test, and patient history. If conditions allow, insulin and proinsulin concentrations can be measured separately.
When the peaks of insulin and C-peptide release occur simultaneously, both assessments show no significant difference in pancreatic β cell function. However, when they are not synchronized, the C-peptide release test can better reflect the true pathophysiological state of the patient than insulin.
Planning | Dai Dongjun
Submission | [email protected]
Cover Image | Zhanku Hai Luo