Artificial Rupture of Membranes (ARM), commonly known as “amniotomy”, is a method of manually intervening to rupture the amniotic membrane at the cervical opening to observe the color of the amniotic fluid, enhance uterine contractions, and accelerate the progression of labor. It is a common induction method during natural childbirth.
1. History of ARM and Scholars’ Perspectives
ARM has been used in obstetric clinical practice since the 11th century, as documented in literature. In the late 20th century, scholars began to question the surgical method of ARM, leading to differing opinions. Obstetric practitioners have reached a consensus that this invasive procedure is no longer considered a necessary intervention during labor.
2. Clinical Applications of ARM
►►►
Inducing Contractions – Labor Induction
01 ARM for Induction
Indications:
(1) Conditions suitable for vaginal trial of labor induction (IOL). (2) Cervical Bishop score ≥ 7.
Relative Contraindications: (1) Fetal head not engaged in the pelvis. (2) Fetal head not firmly against the cervix. The standard procedure for ARM is shown in Figure 1.
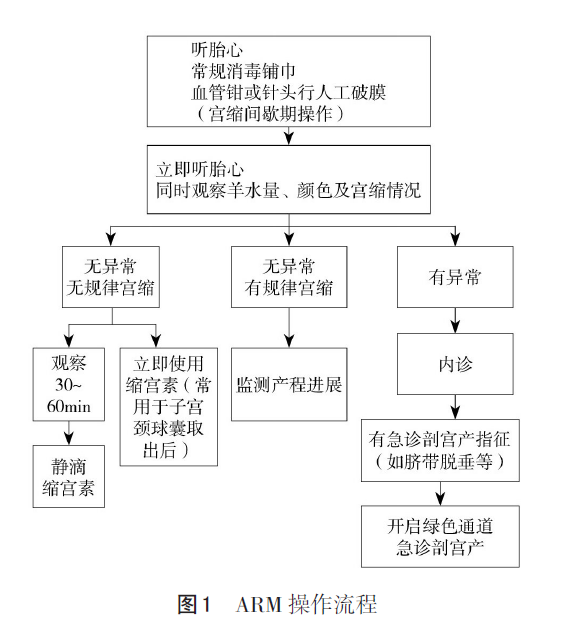
02 Performing ARM After Balloon Catheter for Cervical Ripening
ARM is more commonly used after inducing regular contractions using medication or mechanical methods. For example, if the cervical Bishop score ≤ 6, a balloon catheter is placed for induction, and after 12 hours, it is removed. Following ARM, it is recommended to immediately administer oxytocin intravenously; if the balloon does not effectively ripen the cervix or if ARM cannot be performed, sequential use of dinoprostone for cervical ripening may be considered, or the balloon catheter may be reinserted after 24 hours.
Currently, some scholars in China suggest that after ARM, monitoring should last for 30-60 minutes, and if contractions do not strengthen, a small dose of oxytocin may be used again.
►►►
Shortening Labor – Augmentation
01 Routine ARM During Labor Not Recommended
The 2020 Clinical Practice Guidelines for Normal Labor established by the Obstetrics Group of the Chinese Medical Association and the Perinatal Medicine Group clearly state that routine ARM during labor is not recommended.
02 ARM Recommended in Active Phase, Not During Latent Phase
After entering the active phase, ARM generally refers to performing amniotomy when the cervix is ≥ 5 cm dilated. If there is a lack of coordinated contractions after ARM, oxytocin may be used to promote labor progression. The combination of ARM and intravenous oxytocin can shorten the time from induction to delivery. If the membranes remain intact after full dilation, affecting fetal descent, ARM may be performed during contraction intervals to facilitate fetal descent and manual rotation of the fetal head.
►►►
Adjusting Fetal Position (ARM + Manual Rotation)
For pregnant women with abnormal fetal positions entering the second stage of labor, or when the cervix is nearly fully dilated, ARM followed by manual rotation of the fetal position is a primary corrective measure when the biparietal diameter of the fetal head reaches the level of the ischial spines or lower.
►►►
ARM in Vaginal Birth After Cesarean (VBAC)
A systematic review and meta-analysis by Wingert et al. in 2019 examined VBAC induction methods and delivery outcomes from 1985 to 2019, showing no difference in success rates between ARM and spontaneous labor (RR 1.06, 95% CI 0.88-1.28). These studies assessing the vaginal delivery rates of VBAC lacked high-quality evidence to support that ARM increases the vaginal delivery rate of VBAC.
►►►
ARM in Twin Vaginal Delivery
ARM is not recommended during the first stage of labor. In our clinical practice, an interval of 5-10 minutes between the deliveries of two fetuses is advisable. After the first fetus is delivered, the second fetus should be quickly positioned in a longitudinal lie. If the presenting part is the feet, the fetal ankle can be grasped through the relaxed cervical opening, and traction can be applied to deliver the second fetus during contraction intervals. If the second fetus is vertex-presenting, an assistant may gently push down on the fundus during contractions, and ARM may be performed during contraction intervals once the fetal head engages in the pelvis.
After the first fetus is delivered, oxytocin should be administered as needed based on contraction patterns.
3. Special Considerations for ARM
01 HSV Infection and ARM
The risk of vertical transmission of HSV from mothers to newborns during vaginal delivery is 30%-50%. Even in asymptomatic cases, it is advisable to minimize invasive procedures during labor (ARM, forceps, surgical assistance, etc.) to reduce the duration of fetal exposure to vaginal secretions and the probability of viral infection.
02 Group B Streptococcus (GBS) Infection and ARM
There is evidence that ARM does not increase the risk of early-onset GBS infection in newborns (Evidence Level: D). Any GBS detected in urine during pregnancy should receive intrapartum antibiotic prophylaxis (IAP) without the need for late pregnancy GBS screening. All other pregnant women should be screened for GBS colonization in the vagina and rectum between 35-37 weeks. Except for cesarean sections performed with intact membranes, all GBS-positive women should receive IAP at the time of delivery or when membranes rupture. The optimal timing for IAP is 4 hours before birth; if there is no GBS urinary tract infection, antibiotics should not be used before delivery to clear GBS colonization (Evidence Level: Expert Consensus).
>>>> Indications for prophylactic antibiotic use for GBS during labor include:
(1) Positive GBS screening before labor (AII). (2) GBS bacteriuria during pregnancy (AII). (3) History of GBS infection in newborns (AII). (4) Unknown GBS colonization status with any of the following conditions (AII):
① Preterm labor; ② Premature rupture of membranes > 18 hours; ③ Maternal fever ≥ 38℃; ④ Positive GBS nucleic acid amplification test during labor; ⑤ History of positive GBS in previous pregnancies.
03 Hepatitis Virus Infection and ARM
The 2017 WHO clinical guidelines state that in areas with high rates of hepatitis virus infections among pregnant women, it is advisable to maintain membrane integrity to prevent vertical transmission from mother to child. When a newborn is “immersed” in virus-containing fluid during delivery, care should be taken to gently clear the newborn’s mouth and nasal passages to avoid excessive force that could damage the skin and mucous membranes, allowing the virus to enter the newborn’s body.
04 HIV Infection and ARM
The 2019 guidelines from the UK HIV Association on the management of HIV during pregnancy and postpartum state that invasive prenatal diagnostic procedures can be performed if the HIV RNA load is <50 copies/mL. Pregnant women with ruptured membranes before delivery should aim to deliver within 24 hours if the viral load is low.
4. Precautions for ARM and Emergency Management of Cord Prolapse
01 Emergency Management of Cord Prolapse After ARM
A significant complication of ARM is cord prolapse. Most cases of cord prolapse occur within minutes after membrane rupture; one study found that 57% occurred within 5 minutes, and 67% within 1 hour after rupture. If fetal heart rate decelerations or variable decelerations occur shortly after ARM, especially if abnormal fetal heart monitoring is noted immediately after rupture, cord prolapse should be suspected. If diagnosed, vaginal delivery is not possible in the short term, and an immediate cesarean section should be performed. If blood-stained amniotic fluid is noted after ARM, with or without abnormal fetal heart rate, there is a high suspicion of placental abruption.
In summary, the clinical applications of ARM are:
(1) When the cervical conditions are immature, with a Bishop score ≤6, solely using ARM not only has a low success rate for induction but also cannot predict the timing of labor onset. The prolonged time from membrane rupture to delivery may lead to infection, hence it is not recommended to use ARM alone for cervical ripening. When cervical conditions are mature, with a Bishop score ≥7, ARM can be combined with oxytocin for induction.
(2) In cases of previous cesarean section and a Bishop score ≤6, a balloon catheter is placed for induction, removed after 12 hours, and oxytocin is administered immediately after ARM. If the balloon does not effectively ripen the cervix, sequential use of dinoprostone may be considered or the balloon catheter may be reinserted after 24 hours.
(3) The 2020 guidelines for normal delivery clearly state that routine ARM during labor is not recommended. (4) ARM during the latent phase is not advocated; if indications for ARM exist, it is recommended to perform it during the active phase.
(5) Special cases of ARM must have indications, and all GBS-positive women should receive IAP at delivery or when membranes rupture.
In our department, when performing ARM, we emphasize the “three musts”: there must be indications, physician orders, and records, and it must be executed after good communication with the mother and family.
Disclaimer
This article is published by this platform; if there is any infringement, please contact us for deletion!
Source:Midwife Notes
Recommended Reading



Contact Us
Original Submission | [email protected]
Live Conference | Ms. Zhao 18030732857
Business Cooperation | Mr. Li 13671145702

Click “Share” to help more people
Good articles are being readby everyone
