Introduction
The American Society of Clinical Oncology (ASCO) annual meeting is the largest and most authoritative clinical oncology conference in the world, with nearly 40,000 experts from over 100 countries participating. The focus is on cancer-related research, showcasing representative basic and clinical studies, and discussing current international advanced treatment methods. This year’s conference featured 234 abstracts on urological tumors, with prostate cancer abstracts (116) accounting for half of the urological tumors. According to disease stage classification, metastatic castration-resistant prostate cancer (mCRPC) related research was the most numerous, followed by metastatic hormone-sensitive prostate cancer (mHSPC). Based on treatment categories, new endocrine therapy (NHA) studies still accounted for the majority, followed by radionuclide and new treatments. This article will interpret the key research on mHSPC.

Expert Profile

Professor Xing Nianzeng
-
Chief Physician, Doctoral Supervisor and Postdoctoral Mentor
-
Assistant Director of the National Cancer Center/Chinese Academy of Medical Sciences Cancer Hospital, Director of Urology, General Director of Shanxi Hospital
-
Member of the National Committee of the Chinese People’s Political Consultative Conference
-
National-level Talent of the “Hundred Thousand Talents Project”
-
National “Outstanding Contribution Young and Middle-aged Expert”
-
National Famous Doctor
-
Enjoys Special Allowances from the State Council
-
President of the Urology Branch of the Chinese Medical Association
-
Chairman of the Urological Oncology Committee of the China Health Promotion Committee
-
Specializes in the diagnosis and treatment of urinary tumors and minimally invasive urological surgery, with multiple techniques at the domestic or international advanced level. Over 300 academic papers published domestically and internationally, and has received more than 10 provincial and ministerial-level scientific and technological awards.
Research Progress of NHA in mHSPC Stage
A. Darolutamide
The ARASENS study further analyzed the correlation between prostate-specific antigen (PSA) response and overall survival (OS) in patients.(1)
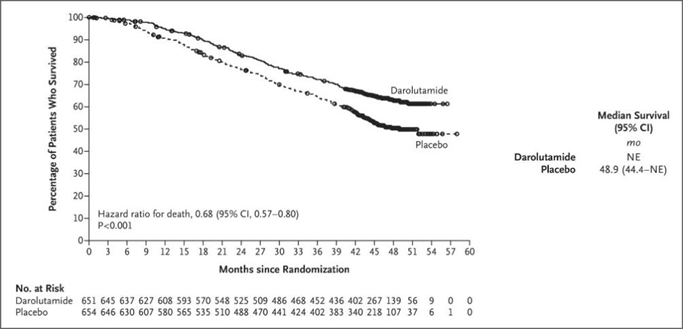
ARASENS is the world’s first prospective triple-drug combination scheme for mHSPC. The study included 1306 newly diagnosed or recurrent mHSPC patients, randomly assigned in a 1:1 ratio to the darolutamide + ADT + docetaxel group and the placebo + ADT + docetaxel group, to evaluate the efficacy and safety of darolutamide in treating mHSPC. On February 17, 2022, the results of the ARASENS clinical trial were simultaneously released at the 2022 ASCO GU and NEJM journals. The results showed that compared with placebo, darolutamide significantly reduced the risk of death by 32.5%. This post-hoc analysis of ARASENS analyzed PSA responses by measuring serum PSA levels at screening and every 12 weeks and used post-hoc Landmark analysis to assess the correlation between undetectable PSA at 24 and 36 weeks and overall OS. The results suggested that the darolutamide combination therapy group significantly prolonged the time to PSA progression (HR 0.255; 95% CI 0.208 – 0.313; p≤0.0001); compared with the placebo group, more patients in the darolutamide combination therapy group were undetectable for PSA at 24 weeks (48.7% vs 23.9%), and this proportion continued to increase at 36 and 52 weeks, respectively 57.1% vs 25.1% and 60.2% vs 26.1%. In the overall survival analysis, patients who were undetectable for PSA at 24 and 36 weeks had a significantly lower risk of death compared to those who had detectable PSA at 24 and 36 weeks, with a death risk reduction of 60% and 65% respectively(1).
An open-label study comparing darolutamide + ADT vs ADT in treating mHSPC using an external control group(ARASEC, NCT05059236)(2)
ARASEC is a phase II single-arm, external control study conducted in the United States. The study will include mHSPC patients with imaging-confirmed metastases and ECOG scores ≤2. Subjects will receive darolutamide (600mg, twice daily) plus ADT treatment. The external control group will consist of mHSPC patients who received ADT treatment alone in the CHAARTED study (393 patients). The primary endpoint is progression-free survival (PFS), and secondary endpoints include overall survival, time to CRPC, and safety. Patient recruitment is ongoing, and the ARASENS study has confirmed the benefits of early intensified triple therapy in the mHSPC stage, while this ARASEC study will supplement the data comparing dual therapy with ARANOTE against monotherapy.
ARANOTE study: A randomized controlled phase III clinical study comparing darolutamide + ADT versus ADT alone in mHSPC patients
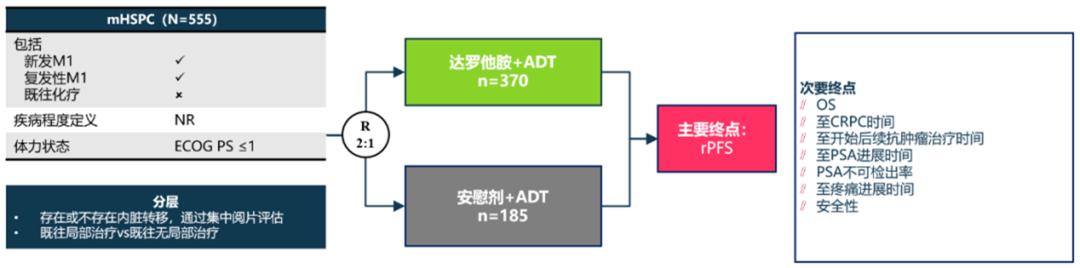
ARANOTE is an international, multicenter, randomized, double-blind, placebo-controlled phase III study designed to compare darolutamide 600mg twice daily plus ADT versus placebo plus ADT in mHSPC patients. A total of 555 patients were randomized in a 2:1 ratio to receive darolutamide or placebo in combination with ADT. The primary endpoint is rPFS; secondary endpoints include overall survival, time to CRPC, time to PSA progression, and safety. Patient recruitment is ongoing, with an expected completion date of September 2025. ARANOTE is led by the Chinese Academy of Medical Sciences Cancer Hospital in China.
B. Enzalutamide
ARCHES post-hoc analysis: Consistency analysis of prostate-specific antigen (PSA) progression and imaging progression in metastatic hormone-sensitive prostate cancer (mHSPC) patients(3)
The ARCHES study has clarified the role of enzalutamide in mHSPC. This study analyzed the consistency between PSA progression and imaging progression in mHSPC patients. mHSPC patients (n=1150) were randomly assigned in a 1:1 ratio to the ENZA (160 mg/d) + ADT group or the placebo (PBO) + ADT group, assessed according to PCWG2 criteria. A total of 267/1150 patients had imaging progression (ENZA + ADT, n=79; PBO + ADT, n=188). At the time of radiological progression, the median PSA (range) for patients treated with ENZA + ADT was 2.25 ng/mL (0-1062.3 ng/mL), while for patients treated with PBO + ADT it was 17.47 ng/mL (0-1779.5 ng/mL). Most patients treated with ENZA + ADT (67%) did not have PSA progression defined by PCWG2 at the time of imaging progression, while 57% of patients treated with PBO + ADT showed progression. Before and after imaging progression, the median absolute and percentage increase in PSA for ENZA + ADT were 0.77 ng/mL and 200%, respectively, while for PBO + ADT they were 12.23 ng/mL and 367%. This post-hoc analysis suggests that imaging progression and PSA progression according to PCWG2 criteria are often inconsistent, thus regular imaging checks are recommended, as continuous PSA monitoring alone may be insufficient to detect imaging progression in many patients.
ARCHES post-hoc analysis: DNA damage repair pathway mutation frequency analysis in ARCHES study participants(4)
In mHSPC patients, DDR alterations are associated with poor prognosis, including shorter overall survival (OS). In the ARCHES study, patients treated with ENZA + ADT had a reduced risk of imaging progression or death compared to those treated with PBO + ADT, leading to improved OS. This post-hoc analysis evaluated the prevalence of DDR alterations and associated baseline characteristics in mHSPC patients in the ARCHES study. Germline DDR mutation detection was performed on blood samples using Ambry Genetics CustomNextCancer panel, with 664 samples available for analysis (ENZA + ADT, n=326; PBO + ADT, n=326). Results indicated that the mutation rate in DDR+ patients was lower than expected (n=34/652, 5.2%). 13 DDR+ patients (38.2%) had low tumor burden disease, while DDR- patients were 228 (36.9%). 21 DDR+ patients (61.8%) and 390 DDR- patients (63.1%) had high tumor burden disease. Among DDR+ patients, 6 (17.6%) were M0 at initial diagnosis, while DDR- patients were 145 (23.5%). Advanced patients (M1) at initial diagnosis were found in 28 (82.4%) DDR+ patients and 465 (75.2%) DDR- patients (4). This post-hoc analysis showed a lower incidence of DDR mutations compared to previous reports, and baseline disease characteristics could not be determined based on DDR mutation status.
Furthermore, this conference will update the latest OS data from ENZAMET.
C. Apalutamide
Assessing the correlation between genomic mutations in some patients in the TITAN study and prognosis(5)
The TITAN study has clarified the therapeutic role of apalutamide in mCSPC, and this will utilize NGS to detect ctDNA and prostate cancer-related 17 genes (including AR). A total of baseline (BL) data of 114 cases and end of study (EOST) data of 129 cases were collected. Genomic mutations are defined as SNV detected in ctDNA, gene inactivation due to heterozygous/homozygous deletions, and gene activation due to amplifications and SNVs. Univariate or multivariate analyses and Cox proportional hazards models were used to assess the correlation between ctDNA/alterations detected at BL or EOST and OS, as well as biomarker correlations detected at EOST during subsequent treatment; results were stratified by treatment group. Results indicated that 36% of patients had detectable ctDNA, and among the mutations assessed, multivariate analysis suggested that baseline ctDNA or any AR mutation (HR, 1.9, 6.7; all p<0.05) and any AR mutation or PI3K mutation detected after treatment (1.7, p<0.05 and 2.2, p<0.001) were significantly correlated with OS. In patients receiving chemotherapy, OS was only associated with EOST PI3KCA activation, PI3K pathway activation, or TP53 inactivation (3.7, p<0.05; 2.4, p<0.05; 3.0, p<0.01).
D. SHR3680
SHR3680 in combination with ADT compared to bicalutamide in treating high tumor burden metastatic hormone-sensitive prostate cancer (mHSPC): a multicenter, randomized, controlled phase III clinical study (CHART) (NCT03520478)(6)
This study is a randomized, open-label phase III study. mHSPC patients (pts) were randomized 1:1, with a total of 654 patients included. The primary endpoints were radiographic progression-free survival (rPFS) and overall survival (OS) assessed by an independent review committee (IRC). At the cutoff date, the average follow-up time in the SHR3680 group was 22.1 months, while in the bicalutamide group it was 20.4 months. Compared to bicalutamide, SHR3680 significantly reduced the risk of imaging progression or death (HR, 0.44; 95% CI, 0.33-0.58; p<0.0001; median, not reached vs 25.1 months). OS data are immature, but there was an improvement in OS in the SHR3680 group compared to bicalutamide (HR, 0.58; 95% CI, 0.42-0.80; p=0.0009). All secondary efficacy endpoints showed benefits for the SHR3680 + ADT group. The incidence of adverse events of any grade for any reason was similar between groups. In the SHR3680 and bicalutamide groups, 19.2% and 13.9% of patients experienced ≥3 grade treatment-related adverse events, respectively. No seizures were reported in the SHR3680 group. This suggests that SHR3680 + ADT significantly improves rPFS in high tumor burden mHSPC patients, with an ideal safety profile.
Research Progress of Chemotherapy in mHSPC Stage
(CHAARTED) trial analysis: Eight-year prognosis analysis in patients with metastatic hormone-sensitive prostate cancer (mHSPC)(7)
Previously, there was no follow-up analysis after 5 years of ADT±docetaxel (D). This report presents an 8-year survival analysis of this type, stratified by new metastasis and low tumor burden (LV), high tumor burden (HV), and K-M analysis of survival rates. A total of 790 patients were included (the last patient enrolled in December 2012), among which 238 patients were still alive, with a median follow-up time of 9.7 years for surviving patients. The median OS for the ADT+D group and ADT group in the overall population was 60.4 and 47.2 months, respectively (HR:0.77; 95% CI:0.65, 0.92; p=0.004). Compared with the ADT group (15.4%; HR:0.67; 95% CI:0.53, 0.84; p=0.0005), the 8-year OS rate in the new HV group (n=421) was significantly higher in the ADT+D group (28.5%) than in the ADT group (15.4%; HR:0.67; 95% CI:0.53, 0.84; p=0.0005). Notably, the 8-year OS rate for HV disease patients using early docetaxel nearly doubled (16% vs 30.2%, p<0.0001), which was observed in both newly diagnosed and primary metastatic HV mHSPC patients. Conclusion: In this long-term updated analysis, ADT+D continues to show significant improvement in OS in the overall population, with the most pronounced difference in newly diagnosed metastatic HV mHSPC patients. The study results emphasize the role of baseline prognostic risk stratification in predicting long-term survival and the benefits of intensified treatment.
Meta-analysis: More accurately defining the impact of docetaxel plus ADT on mHSPC patients(8)
ADT combined with docetaxel can improve survival rates in metastatic hormone-sensitive prostate cancer (mHSPC), but it is still unclear who benefits the most. This meta-analysis included GETUG-15, CHAARTED, and STAMPEDE studies for analysis. The primary outcomes were overall survival (OS), progression-free survival (PFS), and failure-free survival (FFS). A total of 2261 men were included, with a median follow-up of 6 years (all patients). The addition of docetaxel to ADT significantly benefited OS (HR=0.79, 95% CI 0.70 to 0.88, p<0.0001), PFS (HR=0.70, 95% CI 0.63 to 0.77, p<0.0001), and FFS (HR=0.64, 95% CI 0.58 to 0.71, p<0.0001). The relative effect of docetaxel on PFS varied with the volume of metastatic tumors (interaction p=0.027; high tumor burden HR=0.60, 95% CI 0.52-0.68; low tumor burden HR=0.78, 95% CI 0.64-0.94), and the timing of metastatic disease occurrence also differed (interaction p=0.077; initial presence of metastasis HR=0.67, 95% CI 0.60 to 0.75; subsequent metastasis HR=0.89, 95% CI 0.67 to 1.18). The OS results were similar. Considering the combined disease burden and timing of metastasis occurrence, docetaxel can improve PFS and OS for all patients, but patients with low tumor burden combined with subsequent metastatic cases do not benefit. Conclusion: This meta-analysis provides the most detailed assessment of the efficacy of docetaxel on mHSPC and suggests that patients with low tumor burden and subsequent metastatic disease should be considered differently from others.
Meta-analysis: The impact of docetaxel (D) on survival outcomes of metastatic castration-sensitive prostate cancer (mCSPC) patients receiving new hormone therapies (NHTs)(9)
The ARASENS and PEACE-1 trials indicate that the addition of NHT to docetaxel + androgen deprivation therapy (ADT) can improve overall survival (OS) in mCSPC; however, there is currently a lack of effective studies evaluating the efficacy of docetaxel among them. This meta-analysis will assess the impact of docetaxel on survival outcomes in mCSPC combination regimens. A literature search was conducted from the PubMed and Embase databases, yielding 2565 records. After screening the available records, 6 phase III studies were included, involving 6701 patients (TITAN, ARCHES, ENZAMET, LATITUDE, STAMPEDE Abi-M1, and PEACE-1). The results suggested that adding NHT to SOC significantly improved PFS and OS. The benefits of NHT on PFS were similar whether or not docetaxel was used. The benefits of NHT on PFS and OS in mCSPC were not related to the use of docetaxel. Further, a randomized phase III study comparing docetaxel + NHT + ADT with NHT + ADT is needed to assess the contribution of docetaxel to survival outcomes in mCSPC patients receiving NHT + ADT.
Review of mHSPC Triple Intensified Treatment Data
PEACE-1
PEACE-1(10) is a phase III trial designed with a 2×2 factorial design to evaluate the addition of abiraterone acetate plus prednisone and/or local radiotherapy to standard treatment.1173 newly diagnosed mHSPC patients (57% in the high burden group, 43% in the low burden group) received SOC, SOC + abiraterone, SOC + RXT, or SOC + abiraterone + RXT treatment (710 patients received SOC as ADT + docetaxel).
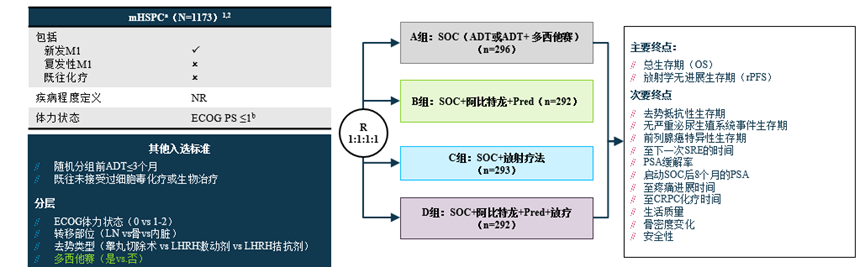
The study underwent three phases of SOC changes, specifically from single ADT from 2013-2015, allowing the use of docetaxel from 2015-2017, and mandatory docetaxel as part of standard treatment from 2017-2018. Compared to docetaxel + ADT, abiraterone + docetaxel + ADT significantly improved rPFS, reducing risk by 50%. In the ADT + docetaxel population, the combination of abiraterone also significantly improved OS (NR vs 4.4 years; HR 0.75, 95% CI: 0.59~0.96, P=0.021).
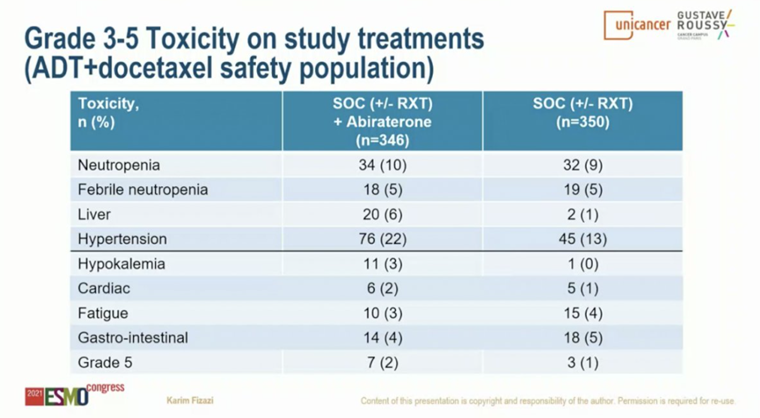
However, regarding adverse reactions, the incidence of hepatotoxicity and hypertension was significantly higher in the experimental group than in the control group.
ARASENS
ARASENS(11) is a randomized, double-blind, placebo-controlled trial and the world’s first prospective triple-drug combination scheme.The study included 1306 newly diagnosed or recurrent mHSPC patients, randomly assigned in a 1:1 ratio to darolutamide + ADT + docetaxel or darolutamide + ADT + placebo treatment groups to evaluate the efficacy and safety of darolutamide in treating mHSPC.
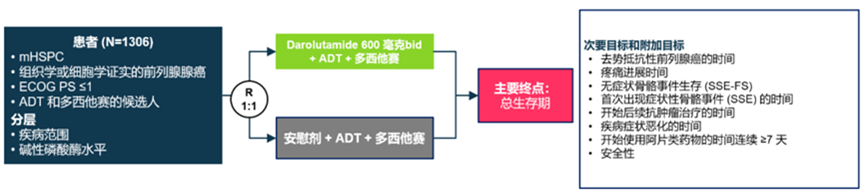
On February 17, 2022, the results of the ARASENS clinical trial were simultaneously released at the 2022 ASCO GU and NEJM journals. The results showed that compared with placebo, darolutamide significantly reduced the risk of death by 32.5%, and significant OS benefits were consistently observed across all subgroups; simultaneously, the darolutamide combination therapy group significantly delayed the time to CRPC; in terms of safety, the darolutamide combination therapy group did not increase safety risks compared to the placebo combination therapy group. Additionally, over 200 Chinese patients were included in the ARASENS study, making the results more applicable to Chinese clinical practice.
Expert Commentary
Currently, the standard treatment regimen for mHSPC has shifted from monotherapy to a two-drug combination therapy of ADT + chemotherapy/new endocrine therapy, but there are still unmet clinical needs.This ASCO meeting featured multiple post-hoc analyses on the impact of NHA on mHSPC treatment, as well as analyses of the treatment effects of the classic drug docetaxel in combination regimens, along with explorations of prognostic molecular biomarkers, collectively providing further evidence and solutions for the treatment of mHSPC.Additionally, the PEACE-1 trial confirmed that the combination of abiraterone, ADT, and docetaxel significantly prolongs overall survival, but there are significant adverse reactions such as hepatotoxicity and hypertension.
The darolutamide ARASENS study, as the first prospective triple-drug combination scheme, reduced the risk of death by 32.5% compared to previous traditional regimens, with the 4-year survival rate increasing from 50.4% in the control group to 62.7%, and benefits were observed across the entire population. Additionally, the strong regimen also significantly delayed the time to CRPC and the time to pain progression, with adverse reactions being similar to the control group. The ARASENS study included over 200 Chinese patients, making the results more applicable to Chinese clinical practice, and is expected to better guide the application of the triple-drug regimen after darolutamide is approved for new indications. The post-hoc analyses reported at this ASCO meeting further clarified the effective and sustained reduction of PSA by darolutamide, which directly promotes survival benefits for patients, and is expected to fundamentally change the treatment concept for mHSPC. Moreover, research on darolutamide in mHSPC and early prostate cancer is ongoing, continuously bringing better survival benefits to patients.
References
1. 2022 ASCO Post Session 5078
2. 2022 ASCO Post Session TPS5111
3. 2022 ASCO Post Session 5072
4. 2022 ASCO Post Session 5074
5. 2022 ASCO Post Session 5066
6. 2022 ASCO Oral Abstract Session 5005
7. 2022 ASCO Post Session 5081
8. 2022 ASCO Post Session 5070
9. 2022 ASCO Post Session 5079
10. ClinicalTrials.gov identifier: NCT01957436. Accessed May 18, 2021
11. Smith MR, et al. N Engl J Med. 2022. ePub.
For academic communication with healthcare professionals only.
