| Source |
| Liu Yachao, Cheng Nuo, Li Yungang, et al. The Value of (68)Ga-PSMA-11 PET/CT Imaging Application of miPSMA Scoring in Diagnosing Prostate Cancer. Chinese Journal of Medical Imaging, 2021, 29(01): 47-50+55 |
| Abstract |
| Objective To explore the diagnostic efficacy of molecular imaging prostate-specific membrane antigen (miPSMA) scoring for prostate cancer, and whether the maximum standardized uptake value (SUVmax) of prostate cancer lesions can predict theD‘Amico risk classification.Materials and Methods A retrospective analysis was conducted on the imaging and clinical data of 38 patients with suspected prostate cancer who underwent 68Ga-PSMA-11 PET/CT. Patients with miPSMA≥2 were diagnosed with prostate cancer, and the final diagnosis was confirmed by biopsy pathology as the “gold standard” to calculate the diagnostic efficacy of miPSMA scoring for prostate cancer. According to the D‘Amico risk group stratification, prostate cancer patients were divided into high-risk and intermediate-low-risk groups, and the differences in SUVmax between the two groups were compared.Results Among the 38 patients, there were 32 cases of prostate cancer and 6 cases of benign prostatic hyperplasia; the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of miPSMA scoring for diagnosing prostate cancer were 90.63% (29/32), 66.67% (4/6), 86.84% (33/38), 93.55% (29/31), and 57.14% (4/7), respectively. The SUVmax of the high-risk group (21 cases) and the intermediate-low-risk group (11 cases) were 24.99±28.18 and 11.29±10.66, respectively, with no statistically significant difference (P=0.133).Conclusion miPSMA scoring for diagnosing prostate cancer has high sensitivity, accuracy, and positive predictive value, but lower specificity and negative predictive value; relying solely on SUVmax cannot predict the D‘Amico risk classification of prostate cancer.【Keywords】Prostate tumor; Positron emission tomography; Computed tomography; Gallium radioisotope; Tumor markers; miPSMA scoring; D’Amico risk classification; Diagnosis; Differential diagnosis; Pathology; Surgery【Classification Number】R737.25; R730.44 【DOI】10.3969/j.issn.1005-5185.2021.01.012 |
The prostate-specific membrane antigen (prostate-specific membrane antigen, PSMA) is highly expressed in prostate cancer cells and is an ideal target for prostate cancer diagnosis and treatment[1]. Radioisotopes 68Ga or 18F labeled PSMA PET has high accuracy for diagnosing and staging prostate cancer.18F or 68Ga labeled PSMA PET tracers vary widely and have their own biological characteristics, such as physiological distribution and excretion pathways in the human body. Therefore, the prostate cancer molecular imaging standardized evaluation (prostate cancer molecular imaging standardized evaluation, PROMISE) standard was introduced to standardize the interpretation of PSMA PET imaging results[2]. This standard proposes to reference the average uptake levels of blood pool, liver, and salivary glands, using the molecular imaging prostate-specific membrane antigen (molecular imaging prostate-specific membrane antigen, miPSMA) scoring system to quantify the PSMA PET uptake in suspicious tumor sites, with scores reported as 0, 1, 2, or 3. For primary prostate lesions, a miPSMA score of ≥2 is diagnosed as prostate cancer, while a score of ≤1 is diagnosed as benign prostatic lesions.D’Amico et al.[3] developed a comprehensive staging system based on clinical TNM staging, preoperative prostate-specific antigen (PSA) levels, and biopsy Gleason scores, classifying the risk of biochemical recurrence (PSA>0.2 ng/ml) after radical prostatectomy into low, intermediate, and high-risk groups. Due to the universality and overall simplicity of the D‘Amico risk stratification model, it has been widely applied in practice and clinical trial design.68Ga-PSMA-11 is the most widely used PSMA PET tracer. This study aims to explore the diagnostic value of 68Ga-PSMA-11 PET/CT imaging, focusing on whether the miPSMA score can predict the D‘Amico risk classification of prostate cancer.1 Materials and Methods1.1 Study Subjects A retrospective analysis was conducted on imaging and clinical data of patients with suspected prostate cancer who underwent 68Ga-PSMA-11 PET/CT at the First Medical Center of the PLA General Hospital from July 2018 to May 2020. Inclusion criteria: elevated PSA, digital rectal examination, ultrasound, or MRI suggesting suspected prostate cancer. Exclusion criteria: ①biochemical recurrence after radical prostatectomy (PSA>0.2 ng/ml); ②68Ga-PSMA-11 PET/CT imaging without subsequent prostate biopsy. A total of 38 patients with primary prostate lesions were included, with an average age of (66±10) years. All subjects signed informed consent, and the study was approved by the Ethics Committee of the PLA General Hospital (Approval No.: S2019-053-02).1.2 68Ga-PSMA-11PET/CT Imaging and Image Analysis The imaging was performed using Siemens Biography 64 and GE Discovery 710, with the 68Ga-PSMA-11 tracer synthesized in our center, with a radiochemical purity of >98%. Patients were not required to fast, and were encouraged to hydrate well before the examination for 2 hours. Subjects received a venous injection of 68Ga-PSMA-11 2.0 MBq/kg, rested quietly for 60 minutes, and then voided their bladder before undergoing torso PET/CT image acquisition.Two experienced nuclear medicine physicians analyzed the PET/CT images without reference to prostate biopsy or pathological diagnosis after radical prostatectomy. The average standardized uptake value (SUVmean) and maximum standardized uptake value (SUVmax) were measured: a circular region of interest with a diameter of 2 cm was placed at the center of the aortic arch to measure the blood pool; a circular region of interest with a diameter of 3 cm was placed in the right lobe of the normal liver to measure the liver; a circular region of interest with a diameter of 1.5 cm was placed at the center of the right parotid gland to measure the salivary gland; and a circular region of interest with a diameter of 1 cm was placed at the center of the maximum uptake in the prostate to measure the prostate lesions.1.3 miPSMA Scoring and Diagnostic Criteria miPSMA scoring: below blood pool is 0, above blood pool but below liver is 1, above liver but below salivary gland is 2, and above salivary gland is 3. A miPSMA score of ≤1 is diagnosed as benign prostatic lesions, while a score of ≥2 is diagnosed as prostate cancer.1.4 D’Amico Risk Stratification Using pathological diagnosis as the “gold standard”, prostate cancer was classified according to the D‘Amico risk stratification[4]: low risk: clinical stage T1c~T2a, PSA≤10 ng/ml, biopsy Gleason score ≤6; intermediate risk: clinical stage T2b, 10 ng/ml<PSA≤20 ng/ml, biopsy Gleason score 7; high risk: clinical stage T2c, PSA>20 ng/ml, biopsy Gleason score 8~10.1.5 Statistical Methods SPSS 17.0 software was used to calculate the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of miPSMA scoring for diagnosing prostate cancer, using pathological diagnosis as the “gold standard”. Independent sample t tests were used to compare the differences in SUVmax between the D‘Amico intermediate-low-risk and high-risk groups, with P<0.05 indicating statistical significance.2 Results2.1 PET/CT Findings Among the 38 cases of primary prostate lesions, there were 6 cases of benign prostatic lesions and 32 cases of prostate cancer; the Gleason scores (primary structure score + secondary structure score) were 3+3 for 5 cases, 3+4 for 8 cases, 4+3 for 6 cases, 4+4 for 9 cases, 5+4 for 1 case, 4+5 for 2 cases, and 5+5 for 1 case. The D’Amico high-risk group had 21 cases, the intermediate-risk group had 8 cases, and the low-risk group had 3 cases. Typical and atypical findings of prostate cancer patients on 68Ga-PSMA-11 PET/CT are shown in Figures 1 and 2.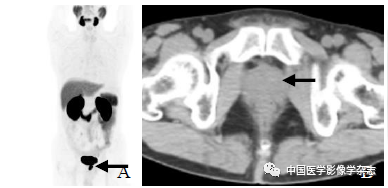
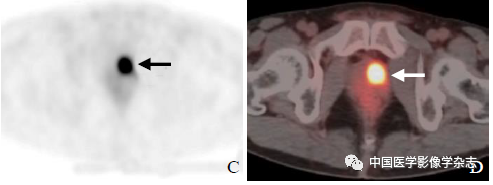 Figure1 Male, 60 years old, prostate cancer, total PSA 11.2 ng/ml, 68Ga-PSMA-11 PET/CT imaging: maximum intensity projection shows abnormal radioactive accumulation in the prostate (arrow, A); CT shows no significant abnormality in prostate density (arrow, B); PET (C) and PET/CT (D) show abnormal radioactive accumulation in the prostate (arrow, D), with a miPSMA score of 3, biopsy and pathological diagnosis after radical prostatectomy confirmed prostate cancer, with a Gleason score of 4+3.
Figure1 Male, 60 years old, prostate cancer, total PSA 11.2 ng/ml, 68Ga-PSMA-11 PET/CT imaging: maximum intensity projection shows abnormal radioactive accumulation in the prostate (arrow, A); CT shows no significant abnormality in prostate density (arrow, B); PET (C) and PET/CT (D) show abnormal radioactive accumulation in the prostate (arrow, D), with a miPSMA score of 3, biopsy and pathological diagnosis after radical prostatectomy confirmed prostate cancer, with a Gleason score of 4+3.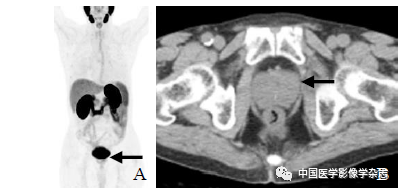
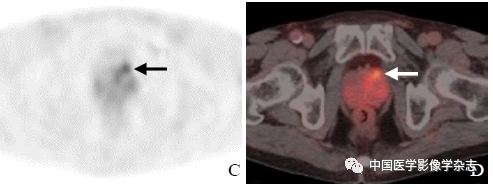 Figure2 Male, 69 years old, prostate cancer, total PSA 8.6 ng/ml, 68Ga-PSMA-11 PET/CT imaging: maximum intensity projection shows localized mild accumulation in the prostate (arrow, A); CT shows no clear abnormality in prostate density (arrow, B); PET (C) and PET/CT (D) show localized mild accumulation in the prostate (arrow), with a miPSMA score of 1, biopsy and pathological diagnosis after radical prostatectomy confirmed prostate cancer, with a Gleason score of 3+3.2.2 miPSMA Scoring for Diagnosing Prostate Cancer Among the 38 cases of primary prostate lesions, a miPSMA score of ≥2 was diagnosed as prostate cancer, while a score of ≤1 was diagnosed as benign prostatic lesions. Using prostate biopsy or postoperative pathology as the “gold standard”, the sensitivity of miPSMA scoring for diagnosing prostate cancer was 90.63%, specificity was 66.67%, accuracy was 86.84%, positive predictive value was 93.55%, and negative predictive value was 57.14% (Table 1).
Figure2 Male, 69 years old, prostate cancer, total PSA 8.6 ng/ml, 68Ga-PSMA-11 PET/CT imaging: maximum intensity projection shows localized mild accumulation in the prostate (arrow, A); CT shows no clear abnormality in prostate density (arrow, B); PET (C) and PET/CT (D) show localized mild accumulation in the prostate (arrow), with a miPSMA score of 1, biopsy and pathological diagnosis after radical prostatectomy confirmed prostate cancer, with a Gleason score of 3+3.2.2 miPSMA Scoring for Diagnosing Prostate Cancer Among the 38 cases of primary prostate lesions, a miPSMA score of ≥2 was diagnosed as prostate cancer, while a score of ≤1 was diagnosed as benign prostatic lesions. Using prostate biopsy or postoperative pathology as the “gold standard”, the sensitivity of miPSMA scoring for diagnosing prostate cancer was 90.63%, specificity was 66.67%, accuracy was 86.84%, positive predictive value was 93.55%, and negative predictive value was 57.14% (Table 1).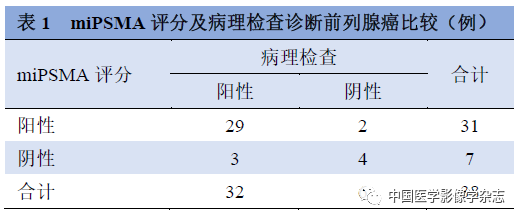 2.3 Differences in SUVmax and SUVmean between D’Amico Low-Intermediate Risk and High-Risk Groups Among the 32 cases of prostate cancer, there were 11 cases in the D’Amico intermediate-low-risk group and 21 cases in the high-risk group. The SUVmax of the intermediate-low-risk group and high-risk group were 11.29±10.66 and 24.99±28.18, respectively, with no statistically significant difference (t=-1.54, P=0.133); the SUVmean of the intermediate-low-risk group and high-risk group were 8.21±8.38 and 17.39±19.74, respectively, with no statistically significant difference (t=-1.459, P=0.153).3 DiscussionIn PSMA PET imaging, visual analysis and quantitative analysis (such as SUVmax) are commonly used methods for differentiating prostate cancer, but due to the variety of PSMA PET tracers, there are certain discrepancies in the results of various studies, leading to low mutual reference value. The PROMISE proposed miPSMA scoring addresses this issue. This study innovatively evaluated the diagnostic efficacy of 68Ga-PSMA-11 PET imaging for prostate cancer and analyzed the differences in SUVmax of prostate cancer lesions between the D‘Amico high-risk and intermediate-low-risk groups, showing that miPSMA scoring has high sensitivity, accuracy, and positive predictive value for diagnosing prostate cancer. There was no significant difference in SUVmax between the high-risk and intermediate-low-risk groups. This method is simple and feasible and can be applied to other PSMA PET imaging. The results of this study require further validation through multi-center, large-sample studies. There is extensive research on the use of PSMA PET imaging for biochemical recurrence after radical prostatectomy and castration-resistant prostate cancer[5-9], while studies on the sensitivity and specificity of 68Ga-PSMA-11 PET/CT imaging for detecting primary prostate cancer lesions are limited. Jiang Cuiping et al.[10] included 20 cases of prostate cancer and used visual analysis, showing that the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 68Ga-PSMA-11 were 95.0%, 69.2%, 84.9%, 82.6%, and 90.0%, respectively. Fendler et al.[11] used semi-quantitative indicators and set SUVmax=6.5 as the standard for distinguishing benign and malignant prostatic lesions, showing that the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 68Ga-PSMA-11 for diagnosing prostate cancer were 67.0%, 92.0%, 72.0%, 97.0%, and 42.0%, respectively. Compared to the studies by Jiang Cuiping et al.[10] and Fendler et al.[11], the sensitivity, specificity, and accuracy of this study are similar to the former, while the positive predictive value and negative predictive value are closer to the latter; the sensitivity and accuracy are higher than the latter, but the specificity is lower; the positive predictive value is higher than the former, but the negative predictive value is lower. The reasons may include: ① different diagnostic criteria: Jiang Cuiping et al.[10] broadly used focal radioactive uptake in the prostate as the basis for diagnosing prostate cancer; Fendler et al.[11] used focal radioactive uptake in the prostate with SUVmax>6.5 as the basis for diagnosing prostate cancer; while this study diagnosed prostate cancer with a miPSMA score of ≥2. ② different study populations: Jiang Cuiping et al.[10] included individuals already diagnosed with prostate cancer; Fendler et al.[11] and this study included individuals with both pathologically confirmed prostate cancer and benign prostatic lesions. This study, based on miPSMA scoring, has high sensitivity, accuracy, and positive predictive value, but lower specificity and negative predictive value. A miPSMA score of 1 was found in 5 cases, with pathological results showing 3 cases as prostate cancer and 2 cases as benign prostatic hyperplasia, indicating that relying solely on miPSMA scoring is not suitable for excluding prostate cancer, and should be combined with clinical history and other imaging examinations for comprehensive assessment.When diagnosing prostate cancer, the patient’s risk depends on factors such as PSA levels, Gleason scores, and tumor extent[11-12].SUVmax or SUVmean are important quantitative analysis indicators of 68Ga-PSMA-11 PET/CT imaging. Currently, the correlation results of SUVmax or SUVmean with Gleason scores or PSA are inconsistent. Fendler et al.[11] showed that SUVmax was not correlated with Gleason scores, but was significantly correlated with PSA. Tulsyan et al.[13] showed that SUVmax was significantly correlated with Gleason scores, while SUVmean was correlated with both Gleason scores and PSA. Eiber et al.[14] showed that SUVmax was not correlated with either PSA or Gleason scores. Ergül et al.[15] showed that SUVmax was correlated with both PSA and Gleason scores. The prostate cancer D’Amico risk group classification combines pre-treatment PSA, clinical staging, and prostate biopsy Gleason scores, classifying it into low, intermediate, or high risk. Hernandez et al.[16] included 6652 prostate cancer patients, showing that the overall biochemical recurrence rate after radical prostatectomy was 84.6%, with D‘Amico low, intermediate, and high-risk groups being 94.5%, 76.6%, and 54.6%, respectively.Boorjian et al.[17] included 7591 prostate cancer patients and showed that compared to low-risk patients, high-risk and intermediate-risk patients had a risk of prostate cancer death that was 11.5 and 6.3 times higher, respectively.The D‘Amico risk stratification system is widely used in the guidelines of the American Urological Association and the National Comprehensive Cancer Network[18-20], being easy to use and able to predict the progression and overall survival rate after prostate cancer treatment. Zhao Qiang et al.[21] showed that the D‘Amico low, intermediate, and high-risk groups had SUVmax of 9.39±4.60 and 13.68±10.39, with no statistically significant difference. The results of this study are consistent with this finding, as there were no significant differences in SUVmax and SUVmean between the D‘Amico high-risk and low-intermediate-risk groups, indicating that relying solely on SUVmax or SUVmean cannot predict the D‘Amico risk classification of prostate cancer.The limitations of this study mainly include a small sample size, especially a significant lack of samples in the D‘Amico low-risk group, leading to the combination of low-risk and intermediate-risk groups into one group. The small sample size may be the reason why SUVmax or SUVmean could not predict the D‘Amico risk classification in the study results. Additionally, this study is retrospective, which may cause selection bias in the results. In conclusion, miPSMA scoring has high sensitivity, accuracy, and positive predictive value for diagnosing prostate cancer, but lower specificity and negative predictive value; relying solely on SUVmax cannot predict the D‘Amico risk classification of prostate cancer.References omitted
2.3 Differences in SUVmax and SUVmean between D’Amico Low-Intermediate Risk and High-Risk Groups Among the 32 cases of prostate cancer, there were 11 cases in the D’Amico intermediate-low-risk group and 21 cases in the high-risk group. The SUVmax of the intermediate-low-risk group and high-risk group were 11.29±10.66 and 24.99±28.18, respectively, with no statistically significant difference (t=-1.54, P=0.133); the SUVmean of the intermediate-low-risk group and high-risk group were 8.21±8.38 and 17.39±19.74, respectively, with no statistically significant difference (t=-1.459, P=0.153).3 DiscussionIn PSMA PET imaging, visual analysis and quantitative analysis (such as SUVmax) are commonly used methods for differentiating prostate cancer, but due to the variety of PSMA PET tracers, there are certain discrepancies in the results of various studies, leading to low mutual reference value. The PROMISE proposed miPSMA scoring addresses this issue. This study innovatively evaluated the diagnostic efficacy of 68Ga-PSMA-11 PET imaging for prostate cancer and analyzed the differences in SUVmax of prostate cancer lesions between the D‘Amico high-risk and intermediate-low-risk groups, showing that miPSMA scoring has high sensitivity, accuracy, and positive predictive value for diagnosing prostate cancer. There was no significant difference in SUVmax between the high-risk and intermediate-low-risk groups. This method is simple and feasible and can be applied to other PSMA PET imaging. The results of this study require further validation through multi-center, large-sample studies. There is extensive research on the use of PSMA PET imaging for biochemical recurrence after radical prostatectomy and castration-resistant prostate cancer[5-9], while studies on the sensitivity and specificity of 68Ga-PSMA-11 PET/CT imaging for detecting primary prostate cancer lesions are limited. Jiang Cuiping et al.[10] included 20 cases of prostate cancer and used visual analysis, showing that the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 68Ga-PSMA-11 were 95.0%, 69.2%, 84.9%, 82.6%, and 90.0%, respectively. Fendler et al.[11] used semi-quantitative indicators and set SUVmax=6.5 as the standard for distinguishing benign and malignant prostatic lesions, showing that the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 68Ga-PSMA-11 for diagnosing prostate cancer were 67.0%, 92.0%, 72.0%, 97.0%, and 42.0%, respectively. Compared to the studies by Jiang Cuiping et al.[10] and Fendler et al.[11], the sensitivity, specificity, and accuracy of this study are similar to the former, while the positive predictive value and negative predictive value are closer to the latter; the sensitivity and accuracy are higher than the latter, but the specificity is lower; the positive predictive value is higher than the former, but the negative predictive value is lower. The reasons may include: ① different diagnostic criteria: Jiang Cuiping et al.[10] broadly used focal radioactive uptake in the prostate as the basis for diagnosing prostate cancer; Fendler et al.[11] used focal radioactive uptake in the prostate with SUVmax>6.5 as the basis for diagnosing prostate cancer; while this study diagnosed prostate cancer with a miPSMA score of ≥2. ② different study populations: Jiang Cuiping et al.[10] included individuals already diagnosed with prostate cancer; Fendler et al.[11] and this study included individuals with both pathologically confirmed prostate cancer and benign prostatic lesions. This study, based on miPSMA scoring, has high sensitivity, accuracy, and positive predictive value, but lower specificity and negative predictive value. A miPSMA score of 1 was found in 5 cases, with pathological results showing 3 cases as prostate cancer and 2 cases as benign prostatic hyperplasia, indicating that relying solely on miPSMA scoring is not suitable for excluding prostate cancer, and should be combined with clinical history and other imaging examinations for comprehensive assessment.When diagnosing prostate cancer, the patient’s risk depends on factors such as PSA levels, Gleason scores, and tumor extent[11-12].SUVmax or SUVmean are important quantitative analysis indicators of 68Ga-PSMA-11 PET/CT imaging. Currently, the correlation results of SUVmax or SUVmean with Gleason scores or PSA are inconsistent. Fendler et al.[11] showed that SUVmax was not correlated with Gleason scores, but was significantly correlated with PSA. Tulsyan et al.[13] showed that SUVmax was significantly correlated with Gleason scores, while SUVmean was correlated with both Gleason scores and PSA. Eiber et al.[14] showed that SUVmax was not correlated with either PSA or Gleason scores. Ergül et al.[15] showed that SUVmax was correlated with both PSA and Gleason scores. The prostate cancer D’Amico risk group classification combines pre-treatment PSA, clinical staging, and prostate biopsy Gleason scores, classifying it into low, intermediate, or high risk. Hernandez et al.[16] included 6652 prostate cancer patients, showing that the overall biochemical recurrence rate after radical prostatectomy was 84.6%, with D‘Amico low, intermediate, and high-risk groups being 94.5%, 76.6%, and 54.6%, respectively.Boorjian et al.[17] included 7591 prostate cancer patients and showed that compared to low-risk patients, high-risk and intermediate-risk patients had a risk of prostate cancer death that was 11.5 and 6.3 times higher, respectively.The D‘Amico risk stratification system is widely used in the guidelines of the American Urological Association and the National Comprehensive Cancer Network[18-20], being easy to use and able to predict the progression and overall survival rate after prostate cancer treatment. Zhao Qiang et al.[21] showed that the D‘Amico low, intermediate, and high-risk groups had SUVmax of 9.39±4.60 and 13.68±10.39, with no statistically significant difference. The results of this study are consistent with this finding, as there were no significant differences in SUVmax and SUVmean between the D‘Amico high-risk and low-intermediate-risk groups, indicating that relying solely on SUVmax or SUVmean cannot predict the D‘Amico risk classification of prostate cancer.The limitations of this study mainly include a small sample size, especially a significant lack of samples in the D‘Amico low-risk group, leading to the combination of low-risk and intermediate-risk groups into one group. The small sample size may be the reason why SUVmax or SUVmean could not predict the D‘Amico risk classification in the study results. Additionally, this study is retrospective, which may cause selection bias in the results. In conclusion, miPSMA scoring has high sensitivity, accuracy, and positive predictive value for diagnosing prostate cancer, but lower specificity and negative predictive value; relying solely on SUVmax cannot predict the D‘Amico risk classification of prostate cancer.References omitted