Bladder monitoring, including urinary incontinence management and bladder urine volume monitoring, is an important aspect of urological nursing. Urinary incontinence is a common condition affecting the quality of life of over 420 million people globally, and bladder urine volume is a crucial indicator for assessing bladder function and health status. Previous studies have explored non-invasive techniques for urinary incontinence management, bladder activity, and bladder urine volume monitoring. This scoping review outlines the prevalence of bladder monitoring, focusing on the latest developments in smart incontinence care wearable devices and the recent technologies using ultrasound, optical, and electrical bioimpedance techniques for non-invasive bladder urine volume monitoring. The results found are promising, and their application will improve the well-being of populations suffering from neurogenic bladder dysfunction and urinary incontinence management. Recent research advancements in bladder urine volume monitoring and urinary incontinence management have significantly improved existing market products and solutions, paving the way for the development of more effective future solutions.
Introduction
The bladder is a muscular organ that functions to store urine produced by the kidneys. The typical volume that an adult bladder can support before the urge to void occurs is estimated to be between 300-500 mL. Bladder monitoring is the process of measuring and assessing bladder function and health status. This is an important aspect of urological nursing as it allows healthcare professionals to evaluate the bladder’s ability to store and void urine and detect any abnormalities or issues that may be present.There are various methods of bladder monitoring, including both invasive and non-invasive techniques used for diagnosing and managing various urological disorders such as urinary incontinence, urinary tract infections, bladder cancer, and voiding dysfunction. They can also be used to assess treatment efficacy and identify potential changes or adverse events during treatment.
Urinary incontinence (UI) management and bladder urine volume (BUV) monitoring are two critical aspects of urological nursing. UI, or the loss of control over urinary function, can significantly impact the quality of life (QoL) of individuals with UI. Accurate and reliable diagnosis and management of UI are crucial for improving patient outcomes. On the other hand, BUV monitoring assesses bladder function and health status by measuring the bladder’s capacity to store and void urine, thereby identifying any potential deviations or issues. Both UI management and BUV monitoring can be performed using invasive and non-invasive techniques.
BUV monitoring holds significant clinical importance, as abnormal urine volume in the bladder may indicate various health issues. UI is one of the most common hygienic problems, affecting millions worldwide. According to population studies from different countries, the prevalence of any type of UI is reported to be around 25% to 45%. The prevalence increases with age, and it has been found to be even higher among nursing home patients. Additionally, over 40% of women over 70 years old are affected by this inconvenience. There are different forms of UI, including stress urinary incontinence, which is often the result of weakened muscles used to prevent urination; urge urinary incontinence, which results from overactivity of the detrusor muscle controlling the bladder; and total incontinence, where the bladder cannot store urine at all. Thus, it has been concluded that UI management is undoubtedly an important issue, and the available and prescribed treatment methods for effective UI management depend on the type, severity, and underlying cause of the incontinence.
Invasive techniques for UI management may include surgical options such as sling procedures, bladder augmentation, and artificial urinary sphincters. These methods involve surgical repair or replacement of the damaged structures causing UI. Invasive techniques for BUV monitoring are still widely used in hospitals, such as (1) catheterization, which is the process of inserting a catheter through the urethra into the bladder; (2) urodynamics, which measures the pressure and flow of urine during voiding; and (3) cystoscopy, which uses a small camera to observe the inside of the bladder and urethra. These methods involve inserting devices into the bladder or urethra to drain urine or measure its pressure and volume. The use of invasive techniques can provide highly accurate information; however, patients may experience discomfort, pain, bladder perforation, leakage, or urinary tract infections, posing risks.
Recent technological advancements have led to the development of new and innovative non-invasive approaches for UI management and BUV monitoring, in addition to several well-known and utilized methods to support UI patients. Examples include (1) pelvic floor muscle exercises (Kegel exercises) that help strengthen the muscles controlling urine flow; (2) bladder training, which helps improve urinary retention capacity and avoid accidents; (3) measuring urine pH, flow rate, and post-void residual urine, which aids in assessing bladder function; (4) medications that help relax the bladder muscles, alleviating symptoms of urinary incontinence. Wearable devices such as urine collection devices and external catheters are also promising methods for improving UI management in women and the elderly. Some of these prototype products are designed to detect urine leakage and its quantity in diapers or incontinence pads, while others aim solely to identify the frequency of urination.
A study conducted by Root et al. in the emergency department showed that using a female external urine collection device is a good alternative to indwelling urinary catheters (IUC) and should be considered for preventing catheter-associated urinary tract infections. Another effective solution for reducing the use of diapers among nursing home residents is ultrasound-assisted prompting for urination (UAPV). When monitoring BUV using ultrasound devices, patients are prompted to urinate when the volume exceeds 75% of the bladder capacity. The results showed a significant reduction in absorption costs, improved working conditions for caregivers, and increased efficiency in managing UI.
Technological advancements have facilitated the emergence of non-invasive techniques for monitoring bladder activity and collecting related information through various technologies, including ultrasound, near-infrared spectroscopy (NIRS) optical monitoring, and electrical bioimpedance. These solutions often provide valuable information regarding bladder volume and function as they can monitor the bladder over time, offering numerous benefits such as accurate information, ease of use, and enhanced patient comfort. Therefore, they can be used to improve the diagnosis and management of urological diseases. The aim of this scoping review is to present the latest research advancements in non-invasive technologies for bladder monitoring in real human volunteers from an engineering perspective, focusing on urinary incontinence management and bladder urine volume monitoring. This will provide researchers, urologists, and healthcare professionals with a comprehensive understanding of the available non-invasive technologies while highlighting their differences (materials and techniques) and defining their potential as applicable solutions in real life.
Thus, the focus of this scoping review is to address the following research questions: What non-invasive technologies allow patients to perform BUV monitoring and UI management? What is the current state of the art (SoA) for BUV monitoring and UI management? What further research is needed in the context of BUV monitoring and UI management?
2. Methods
The methodological framework used in this work is a scoping review, as detailed by Tricco et al. [38]. The choice of this method is to provide a comprehensive overview of the various techniques recently developed for UI management and BUV monitoring and to identify the strengths and weaknesses of these techniques.
2.1. Identification of Relevant Studies
To address the research questions, a systematic search was conducted for English articles published between 2015 and 2022, which were retrieved from the PubMed, IEEE Xplore, ScienceDirect, Scopus, and Web of Science library databases. Initially, keywords such as bladder monitoring, urinary incontinence, and wearable devices were used to identify relevant items. The results of the initial search were used to optimize the search strategy, refining the keywords used during the search to more specific terms, including ultrasound, optical technologies, electrical bioimpedance, urine leakage collection, and technologies tested on humans.
The articles considered aimed to provide information on the following aspects: (1) non-invasive technologies applied to BUV monitoring and UI management, (2) the fundamental characteristics and recent advancements of these technologies, and (3) information on other widely used technologies for BUV monitoring and UI management. In summary, this review only considered articles that introduced non-invasive technologies for human volunteers or patients. Studies involving animals, invasive techniques, phantom evaluations, and case reports were excluded.
2.2. Article Selection
The articles included in this scoping review were selected through a four-step process, which included identification, screening, eligibility, and final selection of articles. In the identification step, the first author (A.H.), second author (S.D.), and third author (C.A.) jointly reviewed the titles and abstracts of the identified articles. Authors (A.H.) and (S.D.) reviewed the full articles during the screening and eligibility steps. All authors participated in the final step to ensure that the articles included in this scoping review met the inclusion criteria and did not meet the exclusion criteria. The literature search for this review was conducted from 2021 to 2022. Figure 1 provides a PRISMA flowchart of the process followed to select the articles constituting this work. Figure 1
The PRISMA flowchart illustrates the process of selecting articles for inclusion in this scoping review.
2.3. Data Charting
Initially, data were cataloged and sorted using Mendeley 2.6 and spreadsheets. Data were aggregated and entered into spreadsheets, organized by publication year, article purpose, technology, use in healthy volunteers or patients, and significant outcomes.
2.4. Summary and Reporting of Results
Compared to systematic reviews, scoping reviews identify a broad range of studies regardless of their research design and quality to outline all materials selected for inclusion in the review [38]. The objectives and types of technologies used for UI management and/or BUV monitoring are presented. The methods used, technical details, target populations, and outcomes obtained from each study are also described.
3. Results
This section is divided into two main parts: Section 3.1 introduces the technologies related to non-invasive BUV monitoring and explains their operational modes and the latest advancements of each technology, while Section 3.2 presents solutions for UI management.
The database searches identified 207 articles, of which 34 met the inclusion criteria for further analysis.
3.1. Bladder Urine Volume Measurement and Monitoring
The technologies used for non-invasive BUV monitoring are diverse. The most common are ultrasound technology, optical technology, and electrical bioimpedance technology. This section describes the different key characteristics of each technology and provides examples of other technologies used for BUV monitoring.
3.1.1. Ultrasound Technology
Ultrasound technology is an imaging technique that provides rich information related to voiding dysfunction. The working principle of ultrasound is based on sending and receiving sound waves at frequencies beyond human hearing range. An ultrasound transmitter and receiver are attached to the skin above the bladder to scan the bladder and determine its shape. The operational method of ultrasound technology can be seen in Figure 2.
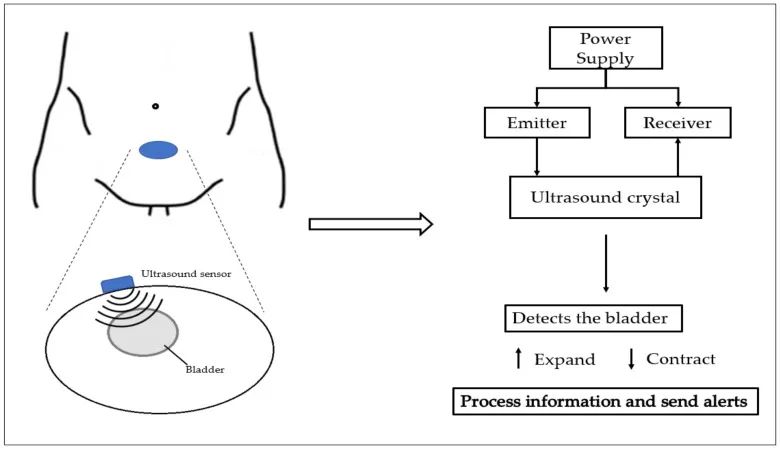
Figure 2
Schematic diagram of the operational method of ultrasound technology.
Ultrasound technology can visualize the bladder and prostate, helping to identify issues such as bladder protrusions of the prostate or detrusor diameter and revealing the presence of diverticula (small pockets that can form in the bladder wall and cause obstruction and pain) [39,40,41,42].
The first wearable ultrasound device for bladder monitoring was developed by Petrican et al. in 1998 [43]; since then, the convenient accessibility of commercial portable ultrasound devices, combined with the non-invasive, safe, and painless nature of the technology, has made it one of the preferred methods for BUV monitoring [22,37,44].
In recent decades, advancements in technology have led to improvements and optimizations in ultrasound devices for BUV monitoring [3,37,45,46,47,48]. Van Leuteren et al. [45] proposed another wearable ultrasound device called SENS-U, which is positioned on the lower abdomen using skin-friendly adhesive. It is based on a combination of four ultrasound transducers within a 30° field of view, transmitting ultrasound waves in a direction perpendicular to the abdominal wall along the bladder. The sensor continuously estimates the BUV status and notifies the user to void when the balloon is full. During urodynamic testing (diagnostic studies involving bladder pressure), the clinical performance of SENS-U was evaluated in 30 children, where a set of tests including measurements of lower urinary tract function was conducted. In the study population, the device was able to detect bladder filling with a success rate of 90% and notify the user nearly 90% of the time. However, it was also reported that proper sensor positioning and childhood obesity are factors to consider when using the device in daily clinical practice [45].
Van Leuteren et al. [46] also proposed one of the advanced improvements, developing a wearable and wireless ultrasound device called the URIKA Bladder Monitor (UBM). It is primarily used to detect the total filling status of the bladder in children with voiding dysfunction. To evaluate UBM, a study was conducted on 14 children with voiding dysfunction who were scheduled for clinical bladder training in pediatric urology. UBM estimates the anterior-posterior dimensions of the bladder. When exceeding a critical threshold, it notifies the patient of bladder filling. The average accuracy of UBM in detecting bladder filling was reported to be 85%. The detection rate was 71% for patients over 10 years old and 100% for patients under 10 years old [46].
Hofstetter et al. conducted a pilot study involving 18 subjects using the DFree device [47]. DFree is a small portable device that uses ultrasound technology and must be connected to the lower abdomen to measure BUV. The study aimed to investigate the impact of such ultrasound devices on the quality of life and satisfaction of patients by assessing their usefulness, ease of use, and level of autonomy provided. Participants, who had various types of bladder dysfunction, used the DFree device for at least 3 hours daily over a period of 12 months. The study concluded that the device could be beneficial in supporting patients with bladder dysfunction; however, further technical development is needed to enhance its reliability [47].
Table 1 presents a multidimensional comparison of three commercially available portable ultrasound devices (UBM, SENS-U, and DFree), including portability, their use for real-time analysis, the participant groups used during testing, and their accuracy in detecting bladder filling.
Table 1
Overview of the comparison of commercially available portable ultrasound devices UBM, SENS-U, and DFree.
| Device | Wearable | Wireless | Real-time Analysis | Tested in Children | Tested in Adults | Accuracy in Detecting Bladder Filling |
|---|---|---|---|---|---|---|
| SENS-U | ✓ | ✓ | ✓ | ✓ | – | 90% |
| UBM | ✓ | ✓ | – | ✓ | – | 85% |
| DFree | ✓ | ✓ | ✓ | – | ✓ | – |
Fournelle et al. [48] introduced a new low-cost portable ultrasound device for research purposes called MoUsE. It is used for long-term and automated BUV monitoring utilizing machine learning segmentation technology. The device includes 32 transmitters and receivers, along with a 32 MHz probe with a three-chip phased array. It is based on data digitization for signal reconstruction and subsequent image processing, with all reconstruction algorithms executed on a GPU for real-time reconstruction and imaging. To evaluate the training algorithms and system accuracy, MoUsE was used to obtain varying bladder filling levels from four volunteers. The results indicated that the proposed method has sufficient sensitivity for applications where significant increases in BUV may occur. However, further performance enhancements are needed for applications requiring precise quantitative assessments of BUV. Additionally, further research is needed to improve the system’s performance, with particular attention to increasing the size of the neural network to enhance the system’s functionality on mobile devices with limited computing resources. Despite these limitations, the results obtained indicate that MoUsE could be a valuable tool for ultrasound imaging research and educational purposes [48].
3.1.2. Optical Technology
Near-infrared spectroscopy is an optical technology used for BUV monitoring applications. It is based on measuring light absorption, which is proportional to the bladder’s fullness. The system is typically placed on the skin above the midline of the lower abdomen and consists of a light-emitting LED light source with specific wavelengths and a photodetector measuring the absorption of emitted light [49,50].
This technology can detect real-time changes in oxygenation within tissues by measuring chromophore variations [49], BUV, and other bladder parameters (such as lower urinary tract dysfunction, bladder outlet obstruction, and bladder overactivity and/or underactivity), which can be measured and estimated using near-infrared spectroscopy [37, 50]. A schematic diagram of the operational method of optical technology can be seen in Figure 3.
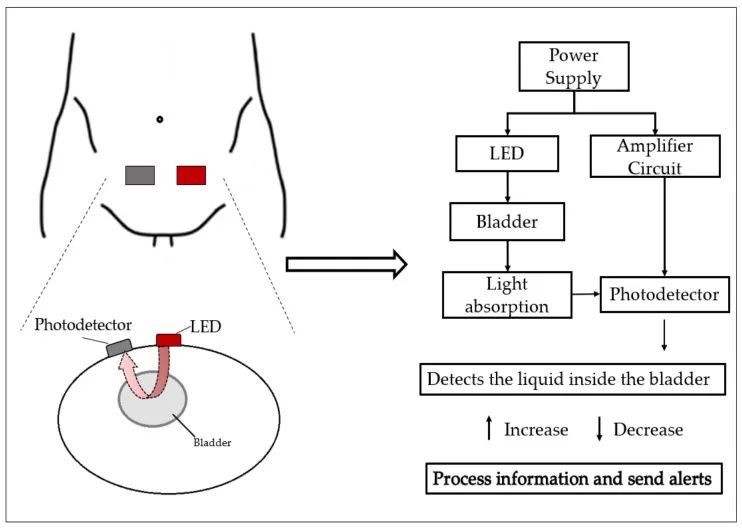
Figure 3
Schematic diagram of the operational method of optical technology.
Macnab et al. have been researching NIRS technology since 2007 for various bladder functions, such as bladder outlet obstruction, bladder overactivity, bladder underactivity, or BUV [51].
Macnab et al. designed, described, and tested a prototype continuous wave near-infrared spectrometer for bladder monitoring in rural clinics in Africa [52]. The design was optimized to enhance photon transport and minimize interference from skin features such as melanin pigmentation and hair. The prototype is equipped with three dual-wavelength LEDs, a silicon photodiode detector, and a long-pass filter to improve photon migration and skin contact. It is powered by a rechargeable battery or AC power supply and communicates with a control computer via Bluetooth. Pilot testing was conducted on 15 male volunteers aged 21-87 recruited from rural medical clinics. The results indicated that the reproducibility of chromophore concentration data suggests that near-infrared spectroscopy can monitor changes in chromophore concentration during urination in pigmented subjects. Successful monitoring is attributed to the technical specifications of the device, optimized application methods, and new protocols for improving device positioning and reducing signal contamination [52].
Fong et al. [53] investigated the application of near-infrared spectroscopy in developing a wearable BUV sensing device that provides alerts for patients with spinal cord injuries. The optical components used in the measurement system consisted of multiple high-power LEDs with peak wavelengths of 970 nm and a single-chip silicon photodiode. They conducted an experiment that included measuring light intensity immediately before urination (i.e., when the bladder is full) for one minute on healthy volunteers, followed by one minute of measurement after urination to determine if any changes in light intensity occurred. They observed a significant drop in light intensity detected by the photodiode between the obtained full bladder dataset and the empty bladder dataset. The experiments helped demonstrate the feasibility of obtaining reasonable signals using the LED setup. This is an important step for using the system in clinical trials with more human volunteers [53].
Macnab et al. [54] also developed a system for wireless near-infrared measurements simultaneously for the bladder and brain. This system consists of two parallel dual-wavelength near-infrared spectrometer devices and proprietary software. The study monitored the natural bladder filling and spontaneous urination of two volunteer subjects using a 23-channel array on the frontal cortex and a 4-channel grid on the bladder. The results showed simultaneous capture of brain and bladder data, indicating localized brain activity during bladder sensation and function. This study provides a new physiological dimension for evaluating bladder control and function [54].
3.1.3. Electrical Bioimpedance Technology
Another promising technology is the use of electrical bioimpedance, where BUV is estimated by measuring the impedance changes of the bladder during its activity. This technology is used to measure the electrical properties of biological tissues, based on applying a small high-frequency electrical current on specific body segments and measuring the voltage produced in that segment using conventional or dry electrodes [22, 37, 55]. Some studies have used electrical bioimpedance technology to obtain different information, such as the bladder state (full or not full) at any time and for monitoring BUV [3, 36, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66]. A schematic diagram of the operational method of bioimpedance technology can be seen in Figure 4.
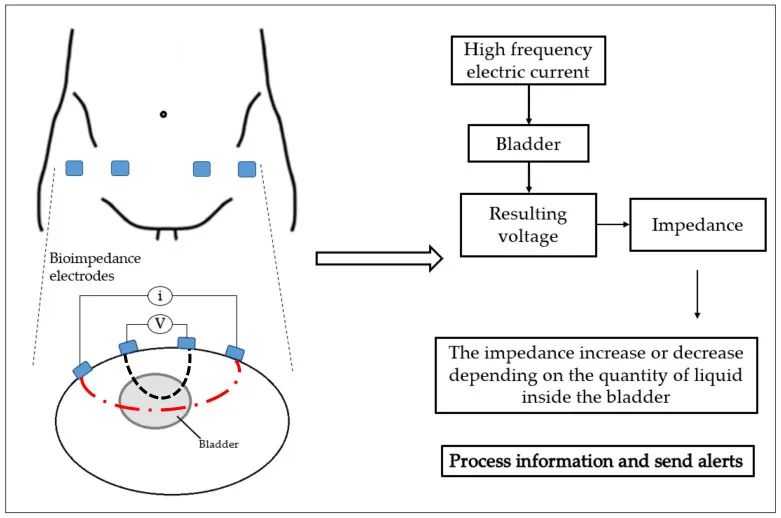
Figure 4
Schematic diagram of the operational method of bioimpedance technology.
To develop a device suitable for seated UI patients, Sakai et al. [56] implemented a prototype system based on electrical bioimpedance to estimate BUV and conducted an experiment. Using SoC AD5933 (Analog Devices, Wilmington, MA, USA) at a frequency of 50 kHz, impedance values were measured on a healthy 24-year-old male volunteer by placing two electrodes 5 cm away from the body’s midline. Through the experiment, they showed that when the bladder is full, the impedance value gradually decreases over time, even with physical movement. Thus, they could approximate BUV based on the obtained impedance values and compare them with BUV measurements obtained through conventional ultrasound devices. They also observed differences in urine storage tolerance and suggested considering urine storage tolerance parameters in future studies [56].
Wang et al. conducted a study [57] using electrical bioimpedance spectral analysis to reveal rhythmic neurogenic activity during natural bladder filling and detect the urge to urinate. They placed two stimulating electrodes and two measuring electrodes on the lower abdominal surface of the body. For continuous measurement of BUV changes during different control stages, 200 μA alternating current at 50 kHz was used and provided by the electrical bioimpedance measurement device. The measurement also required low-polarization wet Ag/AgCl electrodes and an LCR meter to measure voltage. The experiment was conducted on 12 healthy male volunteers who were asked to avoid drinking tea, coffee, or soda before the experiment and to void their bladders before starting the measurements, followed by immediately drinking 100 mL of water. The results indicated that during the natural bladder filling process, the high-frequency spectral power (0.15–0.4 Hz) decreased, the low-to-high frequency ratio increased significantly, while the low-frequency spectral power (0.04–0.15 Hz) showed no significant changes. Through their results, Wang et al. concluded that this method is useful for assessing urination demand and evaluating neuro-regulation during bladder filling [<>].
Noguchi et al. [58] studied a BUV measurement circuit with an electrical bioimpedance four-electrode configuration that can infer (1) the impedance change trend corresponding to BUV and (2) the phase difference change trend corresponding to bladder shape. In this circuit, four Ag/AgCl electrodes were placed on the left and right sides of the bladder, injecting a sine wave current at a frequency of 50 kHz and using a microcontroller (Arduino Due) to measure and calculate voltage. An experiment was conducted on a healthy 26-year-old male. Before the experiment began, the volunteer drank a total of 1.5 liters of isotonic drink and voided several times. During the experiment lasting up to 155 minutes, only phase differences were measured, but the authors noted that electrodes could be placed around the abdomen, and multi-channel phase difference measurements could be introduced. Using this setup, they hoped to extract detailed changes in bladder shape due to using electrical impedance tomography measurements and present these changes to the user [58].
Reichmuth et al. [59] developed a version of an electrical bioimpedance sensor system proposed in the future for measuring BUV during postsurgical surveillance. The battery-operated wearable and wireless system, which requires low power, uses four electrodes placed on the lower abdomen over the bladder. The measurement was performed on a healthy volunteer who drank a total of 1 L. The total duration of the experimental measurement exceeded 180 min. The results show that the device could be used for BUV measurement with only 80 µW power consumption at a 3 mHz sampling frequency. The low power consumption makes the device suitable as a long-term monitoring system [59].
Palla et al. [60] aimed to use a wearable system based on electrical bioimpedance to estimate BUV. They developed a device called Body Gate Way that records the electrical bioimpedance signals of a disposable patch on the user’s skin surface at a sampling frequency of 32 Hz, along with signals from a 50D accelerometer at a sampling frequency of 3 Hz [60]. By connecting medical electrodes to the lower part of the volunteer’s abdomen, they maximized the sensitivity of the measurements. The authors found a clear trend of electrical bioimpedance during bladder filling, although the presence of random noise, such as artifacts caused by volunteer movement, reduced the reliability of the measurements. To overcome this inconvenience, a Kalman filter was designed [61]. This filter is based on a constant speed model, where bladder volume (
Li et al. have researched the preferred electrode placement for accurate BUV measurements [62]. They conducted a simulation study based on a two-dimensional computational model to determine the optimal locations for the four-electrode configuration for BUV measurements. Subsequently, experiments were conducted on eight young healthy volunteers who were asked to drink a total of 1 liter of water and lie in bed to validate the simulation results and study the correlation between BUV and measured impedance values. The results indicated a strong negative correlation between the measured voltage and BUV during bladder activity. They also noted that both simulation studies and human studies suggested that the leftmost and rightmost points of the abdomen are the optimal points for placing the two electrodes injecting alternating current, and it is best to place the two voltage-sensing electrodes about 3 centimeters away from the abdominal center [62].
In another work, Li et al. [63] proposed using electrical bioimpedance technology as an imaging technique. They introduced a BUV imaging system based on electrical impedance tomography (EIT). EIT is a specific application of electrical bioimpedance technology. The measurement used zero electrodes. To validate the system, a study was conducted on six healthy volunteer subjects, and a parameter called the average conductivity index was derived from the EIT images. The results showed a high positive linear correlation between the average conductivity index parameter and BUV for all subjects (correlation coefficient R = 98.0±01.63). In their study conclusions, they noted that EIT could be used to estimate BUV and has potential as a practical technology for assessing BUV [<>].
Leonhäuser et al. [64] conducted a comparative study between EIT technology and ultrasound technology for measuring the process of BUV. For this, commercial equipment (Goe MF II) was used for EIT measurements, which employed 16 electrodes placed horizontally on the lower abdomen of the subjects. Ultrasound technology used two methods to estimate maximum BUV and residual urine: US-ellipsoid/US-L×W × H and bedside bladder scanners. Five healthy volunteers (5 females and 31 males, aged 5±64 years) participated in the comparative study. The obtained results indicated a significant deviation between the measurements and actual BUV. EIT showed considerable potential compared to ultrasound technology. However, the accuracy of EIT needs to be improved by minimizing the effects of motion artifacts and optimizing electrode placement [<>].
In another study, Noyori et al. [65] were inspired by EIT technology to estimate BUV through eight-electrode impedance measurements. They developed a device based on the HUZZAH32 board and the AFE4300 system-on-chip, AFE833, which is an integrated analog front end using a four-electrode I-V method for each impedance measurement channel. The amplitude for the alternating current was set to <> μAp-p at a frequency of 50 kHz, with a resolution of 17 mΩ. The proposed small device was used for feasibility testing in continuous measurements with young healthy volunteers. The obtained results indicated that BUV can be estimated using eight-electrode electrical bioimpedance measurement technology [65].
Body impedance analysis (BIA) is an application of electrical bioimpedance technology. Shin et al. [66] designed a comfortable belt device as a continuous BUV monitoring system based on BIA. The sensors are worn on the abdomen and connected to the body via Ag/AgCl electrodes. A Samsung bio-processor was used as the sensor circuit for impedance measurements. In their study, they injected a 50 kHz current to monitor the bladder and used a 10 kHz current source as their algorithm, with both currents having an amplitude of 100 μAp-p. To minimize inevitable motion artifacts, they proposed a motion artifact reduction algorithm utilizing multiple frequency sources. The participants were 66 healthy volunteers, and the results indicated a close relationship between BUV and impedance changes. This confirmed the feasibility of their system in detecting enuresis events [<>].
Table 2 provides an overview of studies included for electrical bioimpedance technology used for BUV monitoring, highlighting the main findings and setups of the studies.
Table 2
Overview of studies on electrical bioimpedance technology for BUV monitoring.
| Citation | Year | Technical Features (Current/Frequency/N° Electrodes) | N° Healthy Volunteers | Results |
|---|---|---|---|---|
| [60] | 2015 | 100 μA/50 kHz/4 | 1 | During bladder filling, there is a significant and detectable trend in electrical bioimpedance, although the presence of random noise reduces the reliability of the measurements. |
| [57] | 2016 | 200 μA/50 kHz/4 | 12 | This method can be used to check the necessity for voiding, as during natural bladder filling, the high-frequency spectral power (0.15-0.4 Hz) decreases (p = 0.05), and the low-to-high frequency ratio increases significantly (p = 0.001). |
| [63] | 2016 | 1 mAp-p/50 kHz/16 | 6 | In all subjects, there is a high positive linear correlation between the average conductivity index parameter and BUV (correlation coefficient R = 0.98 ± 0.01), while the performance of the four-electrode method is much poorer (R = -0.27± 0.82). |
| [66] | 2017 | 100 μA/10, 50 kHz/3 | 3 | The results indicate a close relationship between BUV and impedance changes. This confirms the feasibility of their system in detecting enuresis events. |
| [64] | 2018 | 5 mA/50 kHz/16 | 10 | There is no significant difference in the average error in estimating maximum bladder capacity between ultrasound estimation methods (ellipsoid (37±17%) and L × W × H (36 ± 15%) and EIT (32 ± 18%). |
| [58] | 2018 | 500 μA/50 kHz/4 | 1 | This circuit can infer the trend of impedance changes corresponding to BUV and the trend of phase difference changes corresponding to bladder shape. The rates of change of impedance and phase difference differ. |
| [62] | 2019 | 1 mAp-p/10 kHz/4 | 8 | During bladder activity, there is a strong negative correlation between the measured voltage and BUV. The leftmost and rightmost points of the abdomen are the optimal points for placing the two electrodes injecting alternating current, and it is best to place the other two voltage sensing electrodes about 3 centimeters away from the abdominal center. |
| [56] | 2019 | -/50 kHz/- | 1 | In all experiments, the tolerated time for urine storage varies. The impedance values were observed to gradually decrease over time, even with physical movement. |
| [59] | 2020 | -/-/4 | 1 | The device can be used for long-term monitoring, as the results indicate the sensor’s accuracy and power consumption of only 3 μW at 80 mHz. |
| [65] | 2021 | 833 μAp-p/50 kHz/8 | 1 | This portable device achieved an SNR of 79.1 dB, with a resolution of 0.017 Ω. It can estimate BUV, although significant estimation errors occur when the voiding volume is small. |
In a separate window
3.1.4. Other Technologies
Another interesting work provides information on recent advancements in UI management, which is a study conducted by Rodas et al. [67], estimating bladder emptying in paraplegics and elderly individuals. To accurately determine when spinal cord injury patients should void their bladders, they proposed a non-invasive approach that combines electrical bioimpedance, lower abdominal temperature, and artificial feedforward neural networks. For the electrical bioimpedance measurements, four Ag/AgCl electrodes were used, along with a sine wave current of 50 kHz and 1 mA injected. A chip MAX30205 was used for real-time measurement of bladder area temperature. The data obtained during bladder emptying from over 18 patients were input into a three-layer feedforward neural network using the BFGS quasi-Newton algorithm. The results showed a high correlation between electrical bioimpedance and lower abdominal temperature during bladder emptying. When the bladder is full, the electrical bioimpedance is lower and the temperature is higher; when the bladder is emptied, the electrical bioimpedance is higher and the temperature is lower. The neural network achieved an accuracy of up to 99.80%, with a reported mean square error very low (1.08 × 1012) [67].
Kurihara et al. [68] developed a BUV measurement model that does not require sensors to be connected to the skin. Instead, a hyperspectral camera (Resonon Inc: PikaXC2) was used, which can capture images in the wavelength range of 398.67 nm to 1016.78 nm. The prediction is based on measuring the urine absorption spectrum obtained immediately after urination. They conducted a series of experiments on a healthy volunteer to evaluate the proposed method. They calculated the error rate of their proposed method compared to the error rate of the ultrasound device attached above the bladder. The proposed method achieved an average error rate of 15.46%, while the ultrasound device’s average error rate was 23.42%. Thus, the proposed method is more accurate than the ultrasound device [68].
3.2. Urine Leakage Collection and Detection
UI management research aims to collect and analyze various technology-based solutions to reduce reliance on IUC and traditional pads, replacing them with external catheters, while others aim to develop smart pads and underwear for urine leakage detection. This section presents wearable devices, external catheters, and the most commonly used urine leakage detection technologies.
Individuals with UI use different types of catheters that are inserted in various ways to collect urine. However, patients prefer external catheters as they can be used for home use and have non-invasive features. For example, Beeson et al. [69] studied an EUFC made of a super-soft absorbent fabric designed to absorb urine and wick it away from the skin. They concluded that IUC is a good alternative to IUC and should be considered for preventing hospital-acquired diseases [69]. Sakamoto et al. [70] developed a self-powered wireless UI sensor system that can determine the amount of urine in a diaper, with a resolution of approximately 100 cm.3 in about 7 minutes. The urine-activated battery of the system consists of two long and flexible electrodes. One electrode is based on activated carbon, while the other is based on aluminum. During the measurement, the two electrodes are placed under the absorbent material of the diaper, which has a grooved structure [70].
In another project, Long et al. [71] introduced a UI solution called TACT3. They developed and manufactured a prototype of underwear capable of alerting the wearer before the pad leakage reaches the outerwear. This is a washable fitted panty with sewn conductive wires that track the most common leakage locations of the pad. The conductive wires connect to a detachable signaling unit, which vibrates three times when any part of the conductive wire gets wet. In their experiment, 81 participants with an average age of 67 were asked to wear the underwear prototype for 2 weeks. Over 90% of the participants rated the overall impression of the prototype product as “good” or “okay.” Subjects confirmed the effectiveness and acceptability of the underwear prototype and reported positive psychosocial impacts [71].
As mentioned in Section 1, Root et al. conducted work implementing EUFC in the emergency department [33]. They implemented a cylindrical catheter covered with soft absorbent filling material designed to be placed externally on the female genitalia. When the patient voids, the urine is drawn from the patient into a wall jar. This maintains the perineum dry and moisture-free from urine. Over a period of 3 months, 187 EUFCs were used on female patients. They noted that patients had no skin irritation throughout the period, indicating that replacing IUC with EUFC in the emergency department is feasible [33].
Su et al. developed a low-cost wearable solution for detecting urine leakage in normal daily life and analyzing urinary biomarkers [72]. This system integrates an electrochemical biosensor in the diaper capable of detecting moisture and chemical characteristics or biomarkers; a portable detection device; and a smartphone data processing application. A healthy volunteer wore the wearable solution for real-time urine analysis. The results obtained showed that urine detection and analysis had high sensitivity, linearity, and selectivity. Compared to traditional hospital-based instrument urine analysis, the developed solution offers advantages such as easier operation and more flexible data access, making it suitable for urine leakage monitoring and urinary biomarker analysis [72]. Compared to traditional hospital-based instrument urine analysis, the developed solution offers advantages such as easier operation and more flexible data access, making it suitable for urine leakage monitoring and urinary biomarker analysis [72].
4. Discussion and Conclusion
This scoping review attempts to outline the latest advancements in bladder monitoring solutions by emphasizing current non-invasive technologies and future research directions in UI management and BUV monitoring. Various ultrasound-based technologies have been utilized, and recently, electrical bioimpedance has been reported as a modern technology.
A large number of solutions with high potential for urinary management and analysis have been developed, primarily targeting women, the elderly with neurogenic bladder, and UI. These solutions are based on active external collection devices, smart pads, or underwear equipped with UI sensor systems. They also aim to provide major alternatives to IUC, as they can detect urine leakage and potentially provide more precise timing estimates for when to change pads after urination. Ideally, these solutions are often portable, self-powered, wireless, and comfortable to wear. Validation needs to be evaluated with more volunteers in real-life settings, and further development work is needed to scale up the mass production process.
In estimating and monitoring BUV, although ultrasound devices are widely used, they may pose challenges to users in terms of size and lack of portability. These limitations typically restrict measurements to clinical or medical environments and may also lead to inaccurate measurements. Studies have shown that the measurement errors can be as high as 10% when comparing the volume of urine measured by ultrasound devices with that recorded using frequency volume charting tools, a medical technique used to record bladder voiding frequency and volume. However, due to recent advances in miniaturization and portability, along with their availability in the market, these devices are still widely used among UI patients.
Despite the broad potential of near-infrared spectroscopy for BUV monitoring, there has been a lack of quantitative assessments to date. A significant limitation of near-infrared spectroscopy is the need for large, permanently connected sensing devices for continuous measurements, which may inconvenience patients. This limitation may lead to limited research interest in utilizing this technology.
Electrical bioimpedance technology has been proposed as a practical method for estimating individual BUV. However, the accuracy of these measurements may be affected by factors such as skin area, skin fold thickness, urine conductivity, and motion artifacts. Despite these limitations, reliable and accurate results have been achieved by correctly positioning electrodes and appropriately selecting the intensity and frequency of injected current. Furthermore, advances in textile electrodes, miniaturized circuit designs, and ultra-low power systems, along with the integration of machine learning algorithms, have the potential to facilitate the development of wearable electrical bioimpedance-based devices for BUV monitoring and UI management applications in the future.
Other methods for determining individual BUV have been proposed, such as using specific cameras or measuring physical parameters like temperature. However, the application of these technologies in human subjects has not been widely studied, leaving the accuracy and reliability of these technologies for BUV monitoring uncertain. Technologies such as infrared thermography, 3D imaging, and microwave bladder state monitoring have also been examined as non-invasive alternatives for BUV monitoring, but studies investigating their accuracy in human subjects are limited, and more research is needed to fully understand their potential in real-world scenarios.
The development, acceptance, and use of modern technology in real life are influenced by various parameters, such as accuracy, cost, and ease of use. This also applies to BUV monitoring and UI management technologies. For instance, ultrasound technology has moderate to high levels of precision, but it requires high-frequency sensors and ultrasound gel, increasing costs and potentially reducing ease of use. On the other hand, optical technologies, particularly near-infrared spectroscopy (NIRS) devices, are low-cost and easy to use, but they are not as accurate as ultrasound-based devices. Electrical bioimpedance technology seems to offer a good middle ground, as it aims to be low-cost, easy to use, and highly responsive in detecting changes in the human body. However, the accuracy of electrical bioimpedance technology varies depending on the equipment used and the population studied.
Wearable technologies, such as external catheters, represent a promising UI management solution as they are non-invasive, easy to use, and can effectively manage various types of UI. These devices consist of a small catheter located externally, connected to a collection bag, allowing urine to flow freely. They are comfortable to wear, discreet, and can enhance patient autonomy. However, it is important to note that while wearable technologies are an emerging field that is rapidly advancing, the results obtained to date are promising, yet they have primarily been evaluated under experimental laboratory conditions and only in studies involving a limited number of healthy subjects. Therefore, future research needs to involve more UI patients and study populations in real-life conditions to fully understand the potential of using wearable technologies for BUV monitoring. Additionally, recommendations or suggestions can be provided to avoid specific issues encountered when using wearable solutions to ensure optimal results during use. By (1) regularly cleaning and disinfecting the catheter and surrounding area with appropriate skin care products, and (2) monitoring the skin for any signs of irritation or infection, specific issues such as skin irritation and infection can be minimized. Additionally, using devices made from hypoallergenic materials can also help reduce the risk of skin irritation and infection.
In summary, advancements in non-invasive technologies for BUV monitoring and UI management have shown potential for improving the QoL of patients with bladder dysfunction. While some technologies, such as ultrasound and pads, have been developed and are currently available on the market, ongoing research is still needed to discover new and improved solutions.
The use of non-invasive technologies provides a safe and effective alternative to invasive procedures and enables healthcare professionals to assess the bladder’s ability to store and void urine and detect various abnormalities or issues that may be present. Therefore, further investigation in this field is crucial to ensure that patients have access to optimal options for managing bladder dysfunction.
The integration of machine learning technology, a subfield of artificial intelligence, is a promising approach to enhancing the accuracy and precision of BUV monitoring systems. Additionally, further research aimed at developing personalized treatment plans for UI patients, considering factors such as age, gender, and underlying conditions, is needed. The electronic health field is expected to play an increasingly important role in UI management, as it can facilitate remote monitoring of patients’ conditions and provide means for communication with healthcare professionals.
Hafid A, Difallah S, Alves C, Abdullah S, Folke M, Lindén M, Kristoffersson A. State of the Art of Non-Invasive Technologies for Bladder Monitoring: A Scoping Review. Sensors (Basel). 2023 Mar 2;23(5):2758. doi: 10.3390/s23052758. PMID: 36904965; PMCID: PMC10007578.