Antibody-drug conjugates (ADCs) in antitumor therapy, also known as “biological missiles,” are a new type of drug that combines targeting and antitumor activity. By linking cytotoxic drugs to targeted drugs, when the targeted drug acts on the corresponding target, the drug enters the tumor cells through phagocytosis, causing lysis and releasing the cytotoxic drug to kill tumor cells. Among these drugs, there is a new type of PDL1 ADC drug that can utilize monoclonal antibodies targeting PD-L1 to precisely deliver cytotoxic drugs to the surface of tumor cells expressing PD-L1, while simultaneously relieving the inhibitory effect of tumor cells on T cells, thus achieving a dual effect.
1. Mechanism of Action
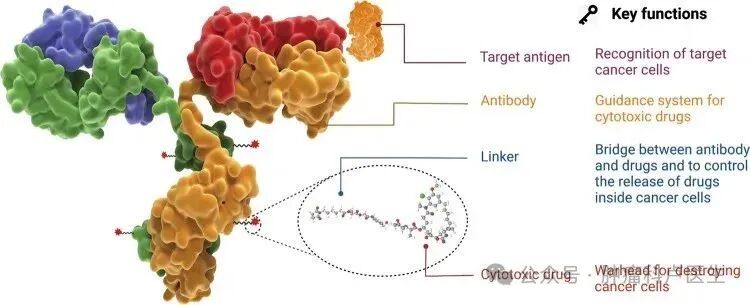
This new type of PDL1 ADC drug consists of three parts: an anti-PD-L1 antibody, a linker, and a cytotoxic drug, making it a precision therapeutic drug. The PD-L1 antibody part of the PDL1 ADC specifically recognizes and binds to the PD-L1 protein on the surface of tumor cells, thereby relieving the immune suppression effect of the PD-1/PD-L1 pathway and restoring T cell cytotoxicity against tumor cells. On the other hand, the formed ADC-antigen complex is internalized by tumor cells, and after the linker breaks, the cytotoxic drug is released, inducing apoptosis and directly killing tumor cells. Through these mechanisms, PDL1 ADC drugs not only relieve the inhibitory effect of tumor cells on T cells but also precisely deliver cytotoxic drugs to PD-L1 high-expressing tumor cells, producing a synergistic effect of “cytotoxicity + immune response.”
2. Clinical Advantages
1. Since PD-L1 is expressed on the surface of tumor cells in various solid tumors, it serves as a pan-tumor target. Currently, many tumors have been approved for clinical use of PD-1 monoclonal antibodies and PD-L1 monoclonal antibodies. Therefore, these tumor types can also use PDL1 ADC drugs, giving this drug a wide range of clinical applications.
2. Even in patients who develop resistance after treatment with PD-1/PD-L1 antibodies, as long as the tumor cells express PD-L1, reusing PD-L1 ADC can “occupy” PD-L1 and release potent toxins to kill tumor cells, allowing patients to potentially benefit clinically even in the context of immune resistance.
3. For immune “cold tumors” that do not respond well to immunotherapy, the response rate to simple immune checkpoint inhibitors is often low, and the therapeutic effect is poor. PD-L1 ADC can utilize the cytotoxic effects of ADC to directly kill tumor cells, thereby promoting the release of more tumor antigens and activating antitumor immune responses, transforming “cold tumors” into “hot tumors.”
4. The systemic exposure of traditional cytotoxic drugs is high, leading to significant side effects on normal tissues and organs while exerting antitumor effects. In contrast, PD-L1 ADC accumulates only on tumor cells with high PD-L1 expression, achieving localized drug release within the tumor microenvironment, theoretically minimizing the impact on normal tissue cells and significantly reducing systemic toxic side effects.
3. Conclusion
The new PD-L1 ADC drug is an antitumor ADC targeting the pan-tumor target PD-L1, which not only relieves the activation and proliferation inhibition of T cells, restoring T cells’ ability to kill tumor cells but also directly achieves cytotoxic killing effects, ultimately exerting a dual mechanism of antitumor action. Its wide application range makes it an ideal antitumor therapeutic drug for pan-tumors. Currently, this type of drug is in clinical research stages, and it is believed that it will soon be applied clinically, benefiting a large number of cancer patients.
 Previous Articles: 1. Outpatient Reimbursement Policies for Tumor Diseases 2. Issues Regarding Calcium Supplementation for Cancer Patients 3. Tumor Markers 4. Radiation Therapy Process 5. How Can Cancer Patients Improve Immunity? 6. How to Interpret Tumor Pathology Reports 7. Highly Malignant Tumor Types 8. Factors Affecting Prognosis in Cancer Patients 9. Radiation Therapy Considerations for Head and Neck Cancer Patients 10. Can Advanced Cancer Still Be Operated On? 11. Diagnosis and Treatment Process for Malignant Tumors 12. Tumor Heterogeneity 13. Ten Treatment Methods for Malignant Tumors 14. Treatment of Bone Metastases 15. Considerations for Cancer Patients Seeking Medical Treatment in Different Locations 16. Clinical Trials of Antitumor Drugs 17. Misconceptions About Cancer Issues 18. Nodules vs. Tumors 19. Targeted Therapy for Malignant Tumors 20. Differences Between Lung Adenocarcinoma L858R Mutation and Exon 19 Deletion.
Previous Articles: 1. Outpatient Reimbursement Policies for Tumor Diseases 2. Issues Regarding Calcium Supplementation for Cancer Patients 3. Tumor Markers 4. Radiation Therapy Process 5. How Can Cancer Patients Improve Immunity? 6. How to Interpret Tumor Pathology Reports 7. Highly Malignant Tumor Types 8. Factors Affecting Prognosis in Cancer Patients 9. Radiation Therapy Considerations for Head and Neck Cancer Patients 10. Can Advanced Cancer Still Be Operated On? 11. Diagnosis and Treatment Process for Malignant Tumors 12. Tumor Heterogeneity 13. Ten Treatment Methods for Malignant Tumors 14. Treatment of Bone Metastases 15. Considerations for Cancer Patients Seeking Medical Treatment in Different Locations 16. Clinical Trials of Antitumor Drugs 17. Misconceptions About Cancer Issues 18. Nodules vs. Tumors 19. Targeted Therapy for Malignant Tumors 20. Differences Between Lung Adenocarcinoma L858R Mutation and Exon 19 Deletion.