 Estimated reading timeApproximately 9 minutes, total 3273 words.
Estimated reading timeApproximately 9 minutes, total 3273 words.
Introduction
Last week, we shared a commentary by Professor Zhang Jian and Dr. Jin Yizi from Fudan University Shanghai Cancer Center on the article “The Incidence of Oral Mucositis and Oral Ulcerative Mucosal Toxicities in Cancer Treatment” published in CA Journal. Did you find it insufficient?
Starting today, we will share a segmented reading of this article over the next three days, breaking it down and highlighting key points to assist your reading. Let’s take some time to read the literature together!

Review Experts

Dr. Zhang Jian, Chief Physician, Editorial Board Member of CA Chinese Version Breast Cancer Expert Group
Administrative Director of the Phase I Clinical Research Ward at Fudan University Shanghai Cancer Center
Recipient of Shanghai’s “Medical Star” Outstanding Young Talent Award
Standing Committee Member of the Breast Cancer Professional Committee of the Chinese Anti-Cancer Association
Vice Convener of the Youth Committee of the Breast Cancer Professional Committee of the Chinese Anti-Cancer Association
Chairman of the Yangtze River Academic Alliance Breast Cancer Group (YBCSG)
Vice Chairman of the Youth Committee of the Breast Professional Committee of the Chinese Research Hospital Association, and Vice Chairman of the National Antitumor Drug Clinical Application Monitoring Youth Committee
Vice Chairman of the Youth Committee of the National Expert Committee on Comprehensive Prevention and Treatment of Breast Cancer
Incoming Chairman of the Clinical Research Professional Committee of the Shanghai Anti-Cancer Association
Vice Chairman of the Pharmaceutical Professional Committee of the Shanghai Anti-Cancer Association
Standing Committee Member of the CSCO Expert Committee on Tumor Support and Rehabilitation Treatment
Standing Committee Member of the Tumor Rehabilitation Professional Committee of the Chinese Rehabilitation Medicine Association
Standing Committee Member of the CSCO Youth Expert Committee
Member of the CSCO Breast Cancer Expert Committee
Member of the Clinical Research Management Professional Committee of the Chinese Anti-Cancer Association
First batch of clinical reviewers for chemical drugs at the National Medical Products Administration CDE
Deputy Editor of Diseases & Research
Editorial Board Member of Translational Breast Cancer Research and Gland Surgery
Published over 40 SCI papers as first/corresponding author (including in The Lancet Oncology)
Scroll down to see all
Definition
Damage to the oral mucosa is referred to as oral mucositis (OM), which is one of the most common side effects of anticancer drugs and head and neck radiotherapy (RT) regimens. In severe OM (SOM), patients experience extreme pain from oral ulcers, hindering oral intake. Despite the devastating clinical consequences of OM, there are currently few methods available to prevent or alleviate mucositis for patients, making it a significant challenge faced by those undergoing cancer treatment.
Epidemiology
It is estimated that approximately 1.9 million new cancer cases will be diagnosed in the United States in 2022. Many patients will experience OM, particularly those receiving head and neck radiotherapy or myeloablative chemotherapy. The following data shows the estimated incidence of OM among different patient populations.
Hematopoietic Cell Transplantation (HCT):
OM is reported as the most severe toxicity by patients undergoing HCT (42%), with its prevalence and severity depending on the type of transplant and the conditioning regimen.
The incidence of OM among patients receiving active conditioning regimens, including total body irradiation, is associated with rates of SOM as high as 98%, as shown in the incidence rates of OM among patients receiving placebo treatment in clinical trials. In a multicenter trial involving hematologic malignancy patients undergoing HCT (19 centers, 1841 patients), 71% of patients were diagnosed with OM, and 21.6% experienced SOM, with the prevalence of SOM being higher in children (25.6%) and adults (24.4%) compared to the elderly (9.2%) (Figure 1).
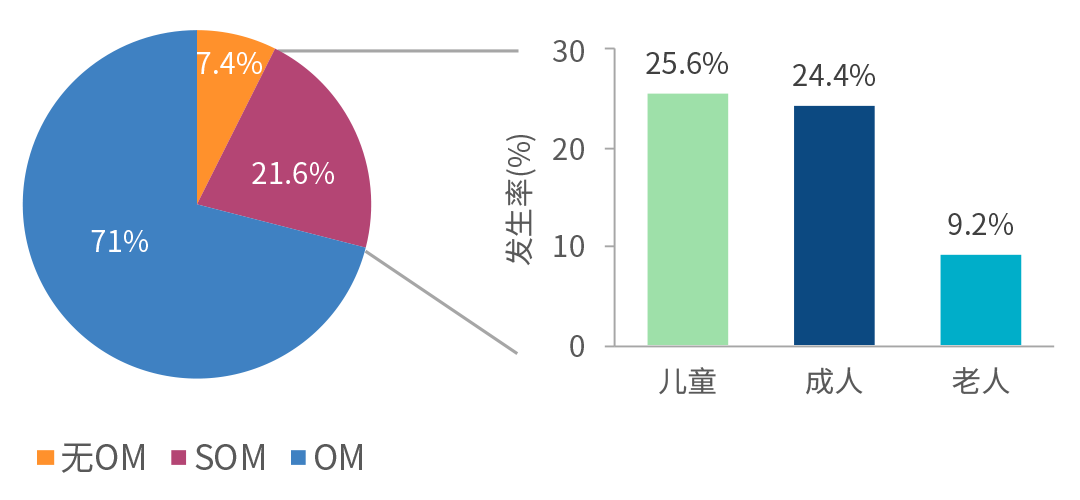
Figure 1. Incidence of OM in a multicenter trial of hematologic malignancy patients undergoing HCT
Comparing the incidence of OM among patients receiving reduced-intensity conditioning regimens to those receiving myeloablative regimens shows that the proportion of patients experiencing any OM is 73.2% for reduced-intensity regimen patients (395 patients, 8 qualifying studies) and 86.5% for myeloablative regimen patients (245 patients, 6 studies) (P<0.0001). Among patients treated with reduced-intensity regimens, 22% to 45.5% experienced mild OM, while 5% to 53.8% experienced SOM. In contrast, among patients treated with myeloablative regimens, 15.9% to 56.7% experienced mild OM, and 19.4% to 83% experienced SOM.
Head and Neck Radiotherapy:
Among patients with head and neck tumors receiving radiotherapy (RT) or concurrent chemoradiotherapy (CRT), 59.4% to 100% experience OM, with approximately 65% experiencing SOM. The incidence of OM is influenced by the tumor site, radiation field, radiotherapy technique, and the use of concurrent chemotherapy. A meta-analysis included 12 prospective trials (1373 head and neck tumor patients) comparing the efficacy and toxicity of high-dose versus low-dose cisplatin CRT, with the incidence of SOM being 75% and 40%, respectively (P=0.0202).
Chemotherapy:
The incidence and severity of OM vary significantly among different treatment regimens. (Figure 2). A meta-analysis assessed the incidence of chemotherapy-related OM using data from phase I-IV clinical trials, revealing an average incidence of 65% for OM among breast cancer patients receiving docetaxel, doxorubicin, and cyclophosphamide (a >1400 patients), with approximately 5% experiencing SOM. Among lung cancer patients receiving platinum-based/gemcitabine therapy (b >1500 patients), the average incidence of OM is approximately 15% (1% SOM). In colon cancer patients receiving 5-fluorouracil chemotherapy (c 898 patients), the average incidence of all grades of OM is 14% (1.7% SOM). However, in colon cancer patients receiving the FOLFIRI regimen (leucovorin, fluorouracil, irinotecan), the incidence of OM is higher (overall OM incidence of 35%, SOM incidence up to 5%). In patients with non-Hodgkin lymphoma (d 1444 patients), the estimated risk of OM is 6.6%.
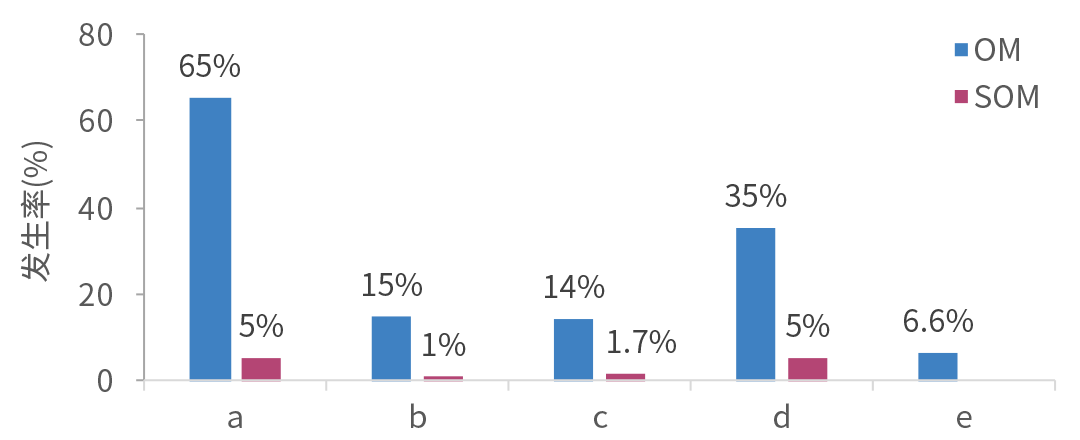
Figure 2. Incidence of OM in different treatment regimens
Pathogenesis
Traditionally, mucosal damage is thought to be caused by the indiscriminate effect of radiotherapy or chemotherapy on normal cells in tissues such as the gastrointestinal mucosa. However, current research indicates that direct cell damage/direct DNA double-strand breaks (DSB) account for only about one-third of the observed damage. Recognizing the complexity of this mechanism, researchers have summarized it into a model dividing the process into five stages (Figure 3): initiation, upregulation and activation (primary damage response), signal amplification, ulceration, and healing. Due to the interconnections and overlaps among stages and associated biological processes, this model briefly summarizes the complex, nonlinear progression of damage.
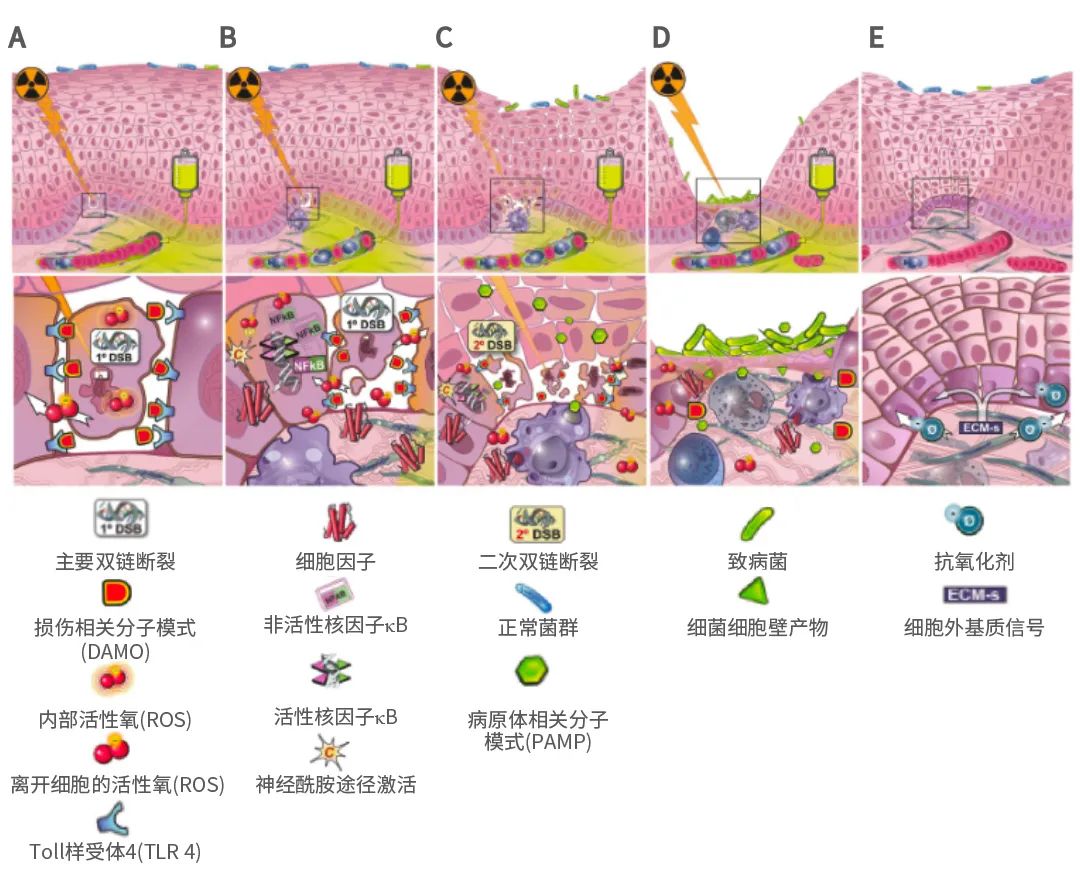
Figure 3. The biological process of mucositis pathogenesis is divided into five stages
Initiation:
The initiation stage occurs immediately after patients receive chemotherapy or RT, where radiation-induced or chemotherapy-induced double-strand breaks represent about 30% of basal cell damage. However, most damage is initiated by the production of reactive oxygen species (ROS) and the activation of the innate immune response. These three events occur simultaneously, interacting within the initiation biological cascade, leading to the apoptosis and necrosis of basal stem cells. The cytotoxic agents directly affect damaged cells, producing damage-associated molecular patterns (DAMPs). The ROS produced by drug-induced cellular damage exhibit high biological activity.
Upregulation and Activation:
During the upregulation and activation stage, ROS and DAMP activate key transcription factors (such as NF-kB), and DAMP activates transcription factors through interactions with pattern recognition receptors (such as TLR-4). Consequently, genes are activated and expressed, leading to the production of pro-inflammatory cytokines and signaling molecules. Simultaneously, after lipid peroxidation of the cell membrane, the ceramide pathway is activated. Damaging enzymes (matrix metalloproteinases) affect connective tissue. Thus, natural defense mechanisms (such as antioxidant enzymes controlling oxidative stress) are suppressed.
Amplification:
In the signal amplification stage, as the process intensifies, the number of signaling molecules (including cytokines) increases, providing positive feedback amplification effects. For instance, released TNF-α can sustain NF-κB activity while initiating MAPK signaling activation. The breakdown of tight junctions leads to increased epithelial permeability, providing a pathway for bacterial cell wall products (PAMPs), further exacerbating the biological response.
Ulceration:
The accumulation of the above biological events leads to progressive tissue damage and loss of epithelial continuity, clinically manifesting as ulceration and atrophic changes. Oral bacteria colonizing the ulcers stimulate infiltrating macrophages, neutrophils, and lymphocytes to secrete additional pro-inflammatory cytokines, exacerbating mucosal damage and deepening its severity. This harmful process continues to evolve, leading to a storm of ROS, PAMPs, DAMPs, and pro-inflammatory cytokines.
Healing:
Finally, at the end of radiotherapy or chemotherapy, ulcers heal on their own. Once the triggering mechanisms of this process are controlled, redox balance begins to restore, and the process gradually approaches completion. Under the stimulation of extracellular matrix signaling molecules, the epithelium undergoes migration, proliferation, and differentiation, and the local microbiome is reconstructed. This final stage enables mucosal regeneration and restoration of continuity. However, the genetics of the new epithelium may differ from the original epithelium, which could lower the threshold for subsequent cycles of radiotherapy or chemotherapy.
Content Edited by: Xiao Ju
Scan to add CA Academic Assistant
Get more benefits in the Chinese version
(Such as valuable Chinese version PDFs~)
👇
1. Elad S, Yarom N, Zadik Y, Kuten-Shorrer M, Sonis ST. The broadening scope of oral mucositis and oral ulcerative mucosal toxicities of anticancer therapies. CA Cancer J Clin. 2022;72(1):57-77. doi:10.3322/caac.21704
Copyright Notice
This article is published by Focus CA, edited/typeset by Xiao Ju; images in the text are sourced from CA and Focus CA design. This material is intended solely for academic conferences or events, aimed at facilitating communication and exchange of medical information, and is for reference by healthcare professionals only. Please retain the complete source above, and the copyright of the article belongs to the original author. For copyright issues or to discuss other collaborations, please contact via email: [email protected].
