
Single-mode imaging diagnostics can no longer meet the clinical needs for cardiovascular diseases. Hospitals need to utilize more advanced imaging equipment and adopt multiple imaging modalities to strive for precise and efficient provision of rich, high-definition medical imaging information. This is essential for accurate preoperative diagnosis, effective intraoperative treatment, and immediate postoperative assessment, which involves the application of multimodal imaging technology. With the continuous development of medical technology, multimodal digital operating rooms have become a project for many hospitals to build or renovate in recent years. Transforming an existing PET/CT room into a digital operating room that includes DSA and CT is a complex system engineering task. It encompasses structural engineering, purification engineering, electrical engineering, decoration engineering, and intelligent engineering, while also coordinating the requirements of various medical equipment manufacturers, the needs of clinical departments, site conditions, construction costs, and timelines.
Site Selection
The medical space at Fuwai Hospital of the Chinese Academy of Medical Sciences is relatively cramped. The PET/CT is located on the first floor of the inpatient building, in a brick-concrete structure that is relatively independent, with a high ceiling and multiple entrances and exits, situated in the core area of the hospital. These architectural features generally meet the requirements for constructing a multimodal digital operating room. Further investigation and research revealed that this area is closely connected to the inpatient building, with clear pedestrian pathways; it has convenient transportation links to the supply room, emergency room, and intensive care unit; it is adjacent to departments such as blood transfusion and pathology; and it has an independent material passageway. Transforming this area into an embedded multimodal digital operating room meets the needs of medical processes without disrupting the normal medical order of the hospital.
The embedded multimodal digital operating room is a new model that organically combines hybrid operating rooms, multimodal imaging technology, and inpatient areas. Major surgeries that would typically require staging in different operating rooms can be completed by a single team in one operating room, eliminating the need for patients to be transferred multiple times between the interventional catheterization room, CT examination room, and surgical operating room, thus avoiding risks such as hypoxia and instability of vital signs during transfers. This operating room emphasizes performing complex surgeries on the same patient at the same location and time, utilizing new composite surgical measures to achieve multidisciplinary collaboration, organically combining the advantages of medical and surgical treatments.
The embedded multimodal digital operating room is planned according to the conditions of the inpatient area, separating the surgical area from the inpatient area using clean and contaminated passageways that meet infection control requirements. The surgical area is equipped with necessary auxiliary rooms as needed, sharing a rest area with the inpatient area. During surgery, various imaging devices provide precise real-time positioning, and a digital information platform enables remote teaching and consultation functions, thereby improving surgical quality, accuracy, and safety, expanding the scope of surgery, and enhancing the utilization of imaging equipment. This independent yet unified design concept shortens the distance between the inpatient area and the surgical area, providing doctors with a more convenient, home-like working environment, which is conducive to improving medical work efficiency, while patients can enjoy “one-stop” services without leaving the inpatient area, fully reflecting the patient-centered service philosophy. Due to the unique location and equipment configuration of the operating room, it can also serve as a day surgery room, accommodating multiple usage modes flexibly.
For the multimodal digital operating room combining DSA and CT, it is essential to communicate fully with the departments involved during the initial design phase, prioritizing the needs of surgical operations. Through repeated discussions, functional requirements can be met while minimizing space usage. The multimodal digital operating room must incorporate mobile equipment into the floor plan, considering both the surgical operation space and allowing for extensive mobility of equipment to meet complex projection requirements. When DSA and CT are not in use, the equipment can be positioned as far away from the surgical bed as possible to provide a more spacious area for surgical operations. According to the requirements for DSA equipment, the net height of the operating room is typically between 2.9 and 3.0 m. Considering structural beams and the specialized requirements of clean operating rooms, the height of the multimodal digital operating room can be controlled between 4.5 and 4.8 m. The area where the hospital’s PET/CT is located just meets the architectural requirements, thus, after preliminary verification, this area was designated as a suitable location for the embedded multimodal digital operating room.
Design Basis
In addition to meeting the current standards of the construction industry, reference should also be made to the “Design Code for General Hospitals” (GB 51039-2014), “Technical Specifications for Clean Operating Rooms in Hospitals” (GB 50333-2013), and “Radiation Protection Requirements for Medical X-ray Diagnosis” (GBZ 130-2013).
Medical Process Design
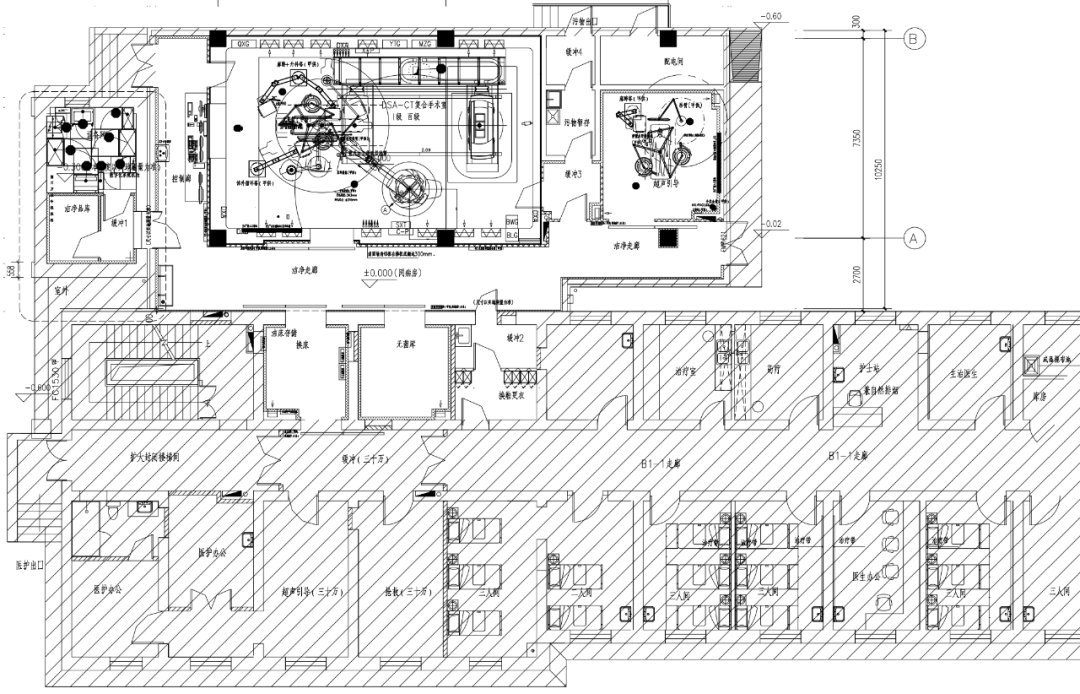
Since the embedded multimodal digital operating room is located at the end of the inpatient area, the design of entry and exit routes is based on the hospital’s infection control requirements. First, it is necessary to avoid cross-flow, ensuring compliance with infection control requirements while meeting the clinical workflow of departments. Medical staff, patients, and clean items enter the operating room through their respective channels; contaminated items are removed from the operating room over the shortest distance possible to avoid secondary contamination. The surgical area is divided into clean and non-clean zones, with a buffer zone set between the two, and the non-clean zone is connected to the inpatient area, allowing access to the clean area through a sanitary passage.
The surgical area is equipped with a sanitary passage, intelligent consumables storage, preoperative preparation area, sterile goods storage, control room, medical equipment room, air conditioning room, and power distribution room, sharing a living area with the inpatient area. During operation, the surgical area and inpatient area are two relatively independent zones.
The core of constructing a multimodal digital operating room is controlling and integrating the internal environment and equipment of the operating room. Given the limited space for this renovation project, builders must consider thoroughly how to arrange equipment such as shadowless lamps, electric knives, defibrillators, anesthesia machines, monitors, extracorporeal circulation machines, lead screens, suspension towers, high-pressure injectors, and digital displays based on usage methods and sequences, avoiding collisions between equipment, improving positioning accuracy, and shortening surgical time. Special attention must also be paid to the positioning of lead screens in relation to the air conditioning system’s air supply ducts, the positioning of suspension towers relative to the embedded components at the top of the DSA, and the relationship between the digital 4K screens and the return air vents on the north and south sides of the operating room, ensuring all facilities are used effectively and reasonably.
▶Operating Room Area and Height
Typically, a dual-ball tube imaging machine requires at least 80 square meters of area, while a single-ball tube imaging machine requires at least 70 square meters. The operating room combining DSA and CT should be internally partitioned to facilitate use in both surgical and CT scanning states. Based on the positioning data provided by medical equipment manufacturers and the needs of surgical operations, the position of the surgical bed is first determined: the foot of the bed faces the observation window and is more than 2 m away from the wall of the control room to allow for the passage of instruments and vehicles during surgery. Then, through thorough communication with the surgical doctors, nurses, anesthetists, and extracorporeal circulation specialists, the positioning of equipment such as the extracorporeal circulation machine, lead screens, and suspension towers is determined based on their behavior trajectories and operational habits. Ultimately, the surgical bed is positioned 2.5 m from the DSA observation window and 2.9 m from both the north and south walls; the minimum sliding distance for the CT provided by the manufacturer is 4.6 m, thus determining the room dimensions to be 11.8 m in length and 7.9 m in width, with a net area of 89 square meters and a net height of 4.0 m.
▶Operating Area Decoration
Based on the maximum radiation dose of DSA, the control room is equipped with a lead glass observation window; the walls of the operating room are protected with 4 mm lead plates up to the floor slab; the floor is leveled and coated with 40 mm thick 4:1 barium sulfate cement slurry for radiation protection.
The floor of the operating room is covered with 2 mm rubber rolls, while other non-wet purified areas and clean auxiliary rooms have their floors treated with self-leveling before being covered with 2 mm thick PVC rolls. Wet areas are treated with 1.5 mm thick polymer cement-based waterproof coating before being tiled with 600 mm × 600 mm non-slip floor tiles. The walls of the purification room are constructed with 50 mm × 50 mm square steel keel, covered with 12 mm thick prefabricated electrolytic steel plates.
To ensure the observation effect of the control room personnel on the operating room, the lead glass in the control room has no splicing seams, and the extracorporeal circulation tower is moved away to avoid obstructing the observation window. The ceiling is made of 600 mm × 600 mm × 0.8 mm aluminum ceiling panels, with a ceiling height of over 2.6 m. Sufficient power and network interfaces are reserved according to equipment requirements, avoiding the use of power strips to prevent clutter and maintain a clean environment. The furniture in the control room is custom-made according to on-site measurements to enhance visual coordination.
▶Operating Area Purification
The purification level of the operating room is Level I, while the purification levels of the clean corridor, clean room, and auxiliary rooms are Level IV. Due to the relatively independent location of the operating room, the inpatient area only has a fan coil system, and the chilled water supply temperature is relatively high, thus a separate cooling source is considered. Calculations show that the maximum cooling load for the operating room area is 144 kW, and the maximum heating load is 70 kW. Therefore, two air-cooled condensing units are set on the east side of the building to handle outdoor fresh air dehumidification in summer, and four air-cooled condensing units are set to handle cooling and dehumidification within the circulation unit and for rapid cooling. A VRV independent air conditioning system is set in the medical equipment room and UPS room to meet year-round cooling needs. A fresh air unit is set to provide fresh air for both the operating room circulation unit and the auxiliary room circulation unit, with a fresh air volume of 3000 cubic meters/hour, including fresh air section, fan section, dehumidification device, and coarse and medium efficiency filters. The operating room circulation unit operates year-round with a four-pipe system, including mixing section, fan section, medium efficiency filter section, evaporation section, dehumidification section, and rapid heating section. The clean corridor, clean room, and auxiliary rooms are equipped with circulation units, including mixing section, fan section, medium efficiency filter section, evaporation section, and dehumidification section.
According to regulatory requirements, when the ophthalmic operating room exceeds 30 square meters and other operating rooms exceed 50 square meters and require an increase in air supply area, the proportion of increased air supply area should not exceed the proportion of increased net area of the operating room. This project determines the air supply area to be 3.2 m × 2.5 m = 8 square meters. Based on the control wind speed and fresh air requirements for the operating area, the air supply volume for the 89 m2 operating room is calculated to be 12,500 cubic meters/hour. Given that the multimodal digital operating room is long and narrow and divided into two areas, to ensure the cleanliness level of the operating room, four high-efficiency air supply outlets are set in the CT area on the east side, with an air supply volume of 2500 cubic meters/hour, resulting in a total air supply volume for the operating room of 15,000 cubic meters/hour. The final air handling unit selection for the operating room is based on an air volume of 16,800 cubic meters/hour.
Cardiovascular specialty hospitals have specific requirements for operating room temperature, necessitating an “emergency rise and fall mode”: during thoracotomy, the indoor temperature must be reduced to 17 °C within 7 minutes to meet the needs of extracorporeal circulation and resuscitation; during closure, the indoor temperature must be raised to 23 °C within 7 minutes. Therefore, the circulation unit in the operating room must be equipped with direct expansion units to meet the rapid heating and cooling needs. By changing the room temperature, it can help reduce the patient’s basal metabolic rate, decrease the perfusion demand of vital organs, thereby alleviating the burden on the heart. Lower temperatures can also provide more effective time for surgical operations and reduce the risk of surgical infections.
It is important to note that the cardiac operating room must pay special attention to humidity control. In the configuration of conventional operating rooms, a dehumidification section is set in the fresh air unit to handle the summer outdoor heat and humidity load. However, in a Class 100 cardiac operating room, a deep dehumidification section must be set to ensure that the humidity in the room reaches 30% to 60% to avoid intraoperative infections.
During the initial design phase, it is essential to fully consider the northern weather, the direction of the fresh air inlet, the frost protection of the units, and the installation of insect-proof nets. Heating coils or heaters should be set at the front end of the fresh air unit, with a minimum flow rate established. This project adopts electric heating for humidification, considering the water quality in the north and the requirements of the humidifier for water quality, using softened water or pure water to ensure the efficiency and safety of the humidifier and coils.
Due to the special nature of the renovation project, the units are located above the operating room. After fully considering vibration and noise issues, beltless turbine fans are selected, with the equipment foundation using shock absorbers, and the machine room employing sound-absorbing panels and other noise reduction measures to minimize the impact of equipment on the operating room below.
▶Electrical Design
The surgical area adopts a TN-S power distribution method, with partial use of an IT system; electrical equipment and lighting related to life safety in the operating room are classified as special important loads within the first-level load, and an uninterruptible power supply and isolation transformer are set for them. A radiating power supply method is used, with two cables drawn from the same transformer in the building’s power distribution room to supply the main distribution box in the surgical area, and then two routes are drawn to supply the DSA/CT distribution box, all using low-smoke halogen-free cables. An automatic transfer switch (ATSE) with dual power supply end-to-end mutual switching is selected to meet the required switching time and comply with relevant standards. It is noteworthy that the UPS should preferably be equipped with online monitoring capabilities and maintenance bypass to meet future operational and maintenance needs.
Equipment manufacturers typically require independent distribution boxes for their equipment, which should be set up according to the manufacturer’s power distribution requirements, and plastic shell air switches should be installed, with input and output lines connected using copper lugs to ensure the stability of power supply voltage. All socket circuits should use residual current protective circuit breakers (electromagnetic type) with an action current of 30 mA and an action time of 0.1 s.
▶Medical Gas Design
The walls of conventional operating rooms are equipped with a comprehensive medical equipment belt, typically designed with one active and one backup: two oxygen terminals, two positive pressure terminals, and two negative pressure terminals. High-power sockets are also considered, with anesthesia waste gas pipelines set at the top. According to regulations, the pressure of oxygen terminals and positive pressure air terminals must not be less than 0.4 MPa, and the pressure of vacuum suction terminals must not be less than -0.06 MPa.
In this design, except for anesthesia waste gas using PVC pipes, all other medical gas pipelines use copper pipes. It is important to note that medical gas interfaces will also be set on the extracorporeal circulation tower and anesthesia tower, with one active and one backup, and high-power power supply sockets must be set. All socket panels should be inclined to avoid virtual insertion due to gravity. Since the manufacturers of the suspension towers and the construction units of the operating room are often not the same, special attention must be paid to the airtightness of the medical gas pipeline connections with the suspension towers, ensuring thorough communication regarding the working interface and valve characteristics to avoid gas leakage during pressure testing and maintenance. The gas terminal alarm box is set at the nurse station, equipped with sound and light alarm functions. The negative pressure suction, oxygen, and compressed air introduced into the operating room must use separate pipelines and cannot be shared with the inpatient area.
▶Information System Design
The central integrated system of the digital operating room comprehensively utilizes various technologies such as network communication, image processing, information integration, communication security, and intelligent terminals, enabling central integration and information control of digital devices within the operating room. This allows the operating room to no longer exist as an isolated entity, enabling the transmission of imaging information within the operating room without the need for fiber optics, and providing one-click 3D reconstruction, one-click image fusion, and other functions required for clinical use.
The digital operating room connects with the hospital’s PACS, HIS, and LIS, integrating imaging information, test information, and intraoperative information of surgical patients, allowing doctors to retrieve information as needed during surgery.
With the help of shadowless lamp cameras, side cameras, and DSA large screen cameras, each step of the surgical operation can be clearly displayed on various screens in the operating room and control room, assisting surgical doctors, anesthetists, extracorporeal circulation specialists, surgical nurses, and other relevant professionals in obtaining comprehensive surgical information, enabling precise surgical navigation. In particular, the export of anesthesia information can reduce the radiation exposure to anesthetists.
Additionally, the main unit can perform multi-screen synthesis, with functions for broadcasting, recording, teaching, remote consultation, monitoring, playback, and editing of imaging data. The control center can connect to the lecture hall and teaching room.
These functions require the advance reservation of various lines, information points, network ports, etc., while also paying attention to the concealment of equipment lines to ensure both aesthetics and compliance with infection control requirements.
In this design, equipment that ensures the normal operation of the operating room, such as air-cooled condensing units, air conditioning units, VRV air conditioning, power distribution cabinets, and UPS monitoring systems, will be connected to the hospital’s intelligent mechanical and electrical management platform for real-time analysis of energy supply conditions, predicting faults, and achieving energy-saving operations.
The multimodal digital operating room is a composite of CT and DSA operating rooms, and its design must meet the needs for close collaboration among surgical doctors, radiologists, engineers, anesthetists, and nurses. It should facilitate the participation of radiologists in surgical planning and intraoperative image processing, providing surgeons with the best surgical path and dynamic changes in intraoperative images, while also considering the operations of surgical procedures and the movement of personnel.
Given the complexity of constructing a multimodal digital operating room, which involves multiple fields, it can be considered as a whole from both engineering design and medical equipment procurement perspectives. During the design phase, thorough communication with equipment manufacturers is essential to comprehensively reflect the needs of medical equipment in the drawings. At the same time, the planning and design should be forward-looking.Original Authors:Cheng Fangdian, Chen Yuhui, Hu Daotao (Fuwai Hospital, Chinese Academy of Medical Sciences)Source: “Chinese Hospital Architecture and Equipment” magazine, Issue 9, 2022Previous HighlightsAbout the second round of notification for the 2022 China Hospital Architecture and Equipment Innovation Development Conference (HCDE)|2021 Annual China Hospital Architecture and Equipment – Craftsman Figures (Hospital Category) Announcement|2021 Annual China Hospital Architecture and Equipment – Craftsman Figures (Architecture Category) Announcement|2021 Annual China Hospital Architecture and Equipment – Craftsman Figures (Mechanical and Electrical Category) Announcement|2021 Annual China Hospital Architecture and Equipment – Craftsman Enterprises 2021 Annual Hospital Architecture and Equipment – Craftsman Cases (Architectural Design Category) Results Announcement 2021 Annual Hospital Architecture and Equipment – Craftsman Cases (Decoration Design Category) Results Announcement 2021 Annual Hospital Architecture and Equipment – Craftsman Cases (Management Category) Results Announcement All done! A comparison of three versions of the “General Hospital Construction Standards”~ Understanding the 2021 version of the “Traditional Chinese Medicine Hospital Construction Standards”~ Interpretation of the “Medical Waste Classification Directory (2021 version)” Practical Post | What standards and specifications should be referenced when writing academic papers? Are isolation wards, negative pressure wards, and negative pressure isolation wards the same thing? No more quarreling! There are rules for dividing construction interfaces in hospital construction projects. A new model for the construction of endoscope reprocessing centers in hospitals
During the pandemic, the disinfection scope, methods, and measures of medical institutions (authoritative version)
This is a garden-style, one-stop service tertiary hospital
Medical construction projects adopt the EPC model, and these risks must be noted
The application of a special supervision model in the closing phase of hospital construction projects – taking Sichuan University West China Tianfu Hospital as an example
Six issues in the radioactive wastewater treatment project of the nuclear medicine department
Key points for constructing positive and negative pressure conversion operating rooms under the “normal epidemic” (including cases)
What to do when large hospitals encounter temporary voltage drops from external power sources?
Key points, difficulties, and countermeasures for the construction of DSA machine rooms in large hospitalsIt’s really different! This is a smart disinfection supply center