
Overview
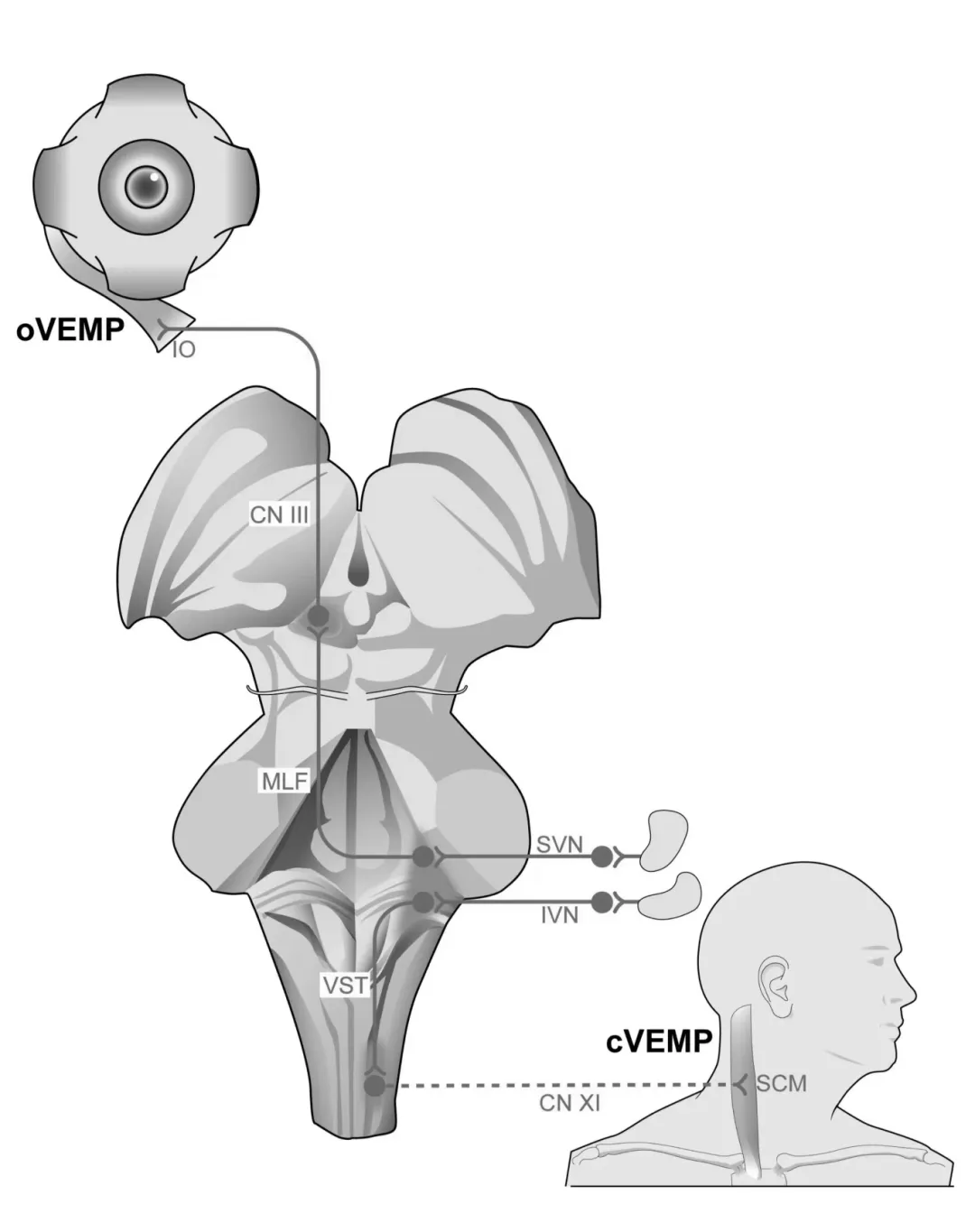
Figure1 Diagram of oVEMP and cVEMP conduction pathways
CN Ⅲ: cranial nerve Ⅲ, the third cranial nerve (oculomotor nerve); CN Ⅺ: cranial nerve Ⅺ, the eleventh cranial nerve (accessory nerve); IO: inferior oblique muscle, (eye) inferior oblique muscle; IVN: inferior vestibular nerve;MLF: medial longitudinal fasciculus, medial longitudinal fasciculus; SCM: sternocleidomastoid muscle, sternocleidomastoid muscle; SVN: superior vestibular nerve, superior vestibular nerve; VST: vestibulospinal tract, vestibulospinal tract;
As cVEMP and oVEMP technologies are promoted in China, it is necessary to standardize their detection methods, result evaluation, and clinical applications. The editorial board of the Chinese Journal of Otorhinolaryngology-Head and Neck Surgery and the Audiology Group of the Otorhinolaryngology-Head and Neck Surgery Branch of the Chinese Medical Association organized domestic experts to discuss multiple times, and based on the latest research results at home and abroad, this consensus was formulated to standardize and improve the detection and clinical application of cVEMP and oVEMP. Among the various stimulation methods inducing VEMP, air-conducted sound stimulation is currently the most convenient and widely used type in clinical practice, and this consensus only involves the detection of cVEMP and oVEMP induced by air-conducted sound stimulation.
Testing Environment
The testing environment should be kept quiet, and it is recommended to conduct the tests in a soundproof/electromagnetic shielded room. The examination room should be equipped with a testing bed or chair, maintaining a comfortable temperature and humidity. It should have an otoscope, disposable or disinfectable electrode patches, 75% alcohol cotton balls, abrasive paste, conductive gel, tape, gauze, and earplugs or headphones of various specifications.
Pre-Test Preparation
1 Subject education: Inform the subject or guardian about the testing time and process, and notify the potential discomfort and precautions during the test. For minor subjects, it is necessary to patiently calm their emotions and obtain good cooperation. For younger children, sometimes parental assistance or collaboration from 2-3 testing personnel may be required.
2 Recording site preparation: Check the subject’s eye and neck muscle activity state, assess cooperation level.
3 External ear canal examination: The tester should carefully examine the subject’s external ear canal and tympanic membrane to rule out cerumen or otitis media that could affect test results, and select appropriate earplugs or headphones based on the size of the external ear canal.
4 Skin preparation: Clean the skin surface where the electrodes will be placed with alcohol cotton balls to remove grease, and if necessary, use abrasive paste to remove dead skin cells to reduce the impact of electrode impedance on test results, ensuring secure attachment of electrodes.
Use an evoked potential device for testing, ensuring the equipment has a reliable grounding wire and is calibrated regularly. It is recommended to calibrate the short-duration sound signal to peak equivalent sound pressure level (dB peak-equivalent sound pressure level, dB peSPL) to measure sound intensity. Considering the practical difficulties in calibrating equipment at various institutions, if it is temporarily not possible to calibrate to dB peSPL, dB SPL or dB nHL can also be used for testing.
Testing Parameters
The high cut-off frequency for cVEMP testing is set between 5-30Hz, and the low cut-off frequency is set between 1000-3000Hz; oVEMP has a high cut-off frequency set between 1-20Hz and a low cut-off frequency between 1000-2000Hz.
The amplifier gain for cVEMP is set between 2500-5000; oVEMP amplifier gain is between 20000-50000.
The usable stimulation rate is 2-10 times/second, and it is recommended to use 4.9-5.1 times/second.
The recording window width is set to -20-80ms, or -20-60ms.
The number of averages is set to 100-200 times.
During the test, electromyography should be used to monitor the muscle contraction intensity. The cVEMP amplitude is positively correlated with muscle contraction intensity; the greater the muscle strength, the larger the amplitude. Therefore, during the test, it is recommended to keep the contraction amplitude of the sternocleidomastoid muscle within a relatively stable range, typically set at 50-200µV.
Testing Procedure
Electrode position: The recording electrode is placed at the midpoint or upper 1/3 junction of the sternocleidomastoid muscle, the reference electrode is placed on the surface of the sternocleidomastoid joint, and the ground electrode is placed on the forehead or chin (Figure 2a), with inter-electrode resistance ≤5kΩ.
Testing method: ① Supine head lift method: The subject lies supine and keeps the head elevated about 30º, maintaining tension in both sternocleidomastoid muscles; ② Sitting neck rotation method: The subject sits, turns the head to the opposite side, and maintains tension in the sternocleidomastoid muscle; sound stimulation is applied while recording the potentials generated by the activity of the same-side sternocleidomastoid muscle. After the initial sound intensity elicits a stable VEMP waveform, repeat recording every 10dB decrease until the waveform disappears, then increase by 5dB for retesting to determine the threshold.
Electrode position: The recording electrode is placed about 1cm below the midline of the pupil at the lower edge of both eye sockets, the reference electrode is placed about 1-2cm below the recording electrode, and the ground electrode is placed on the forehead or chin, with inter-electrode resistance ≤5kΩ. (Figure 2b).
Testing method: The subject adopts a supine or sitting position, gazing as much as possible at a point approximately 30º above the top of the head, recording the potential generated by the activity of the contralateral inferior oblique muscle, requiring the subject to avoid blinking and unnecessary eye movements. After the initial sound intensity elicits a stable VEMP waveform, repeat recording every 10dB decrease until the waveform disappears, then increase by 5dB for retesting to determine the threshold.
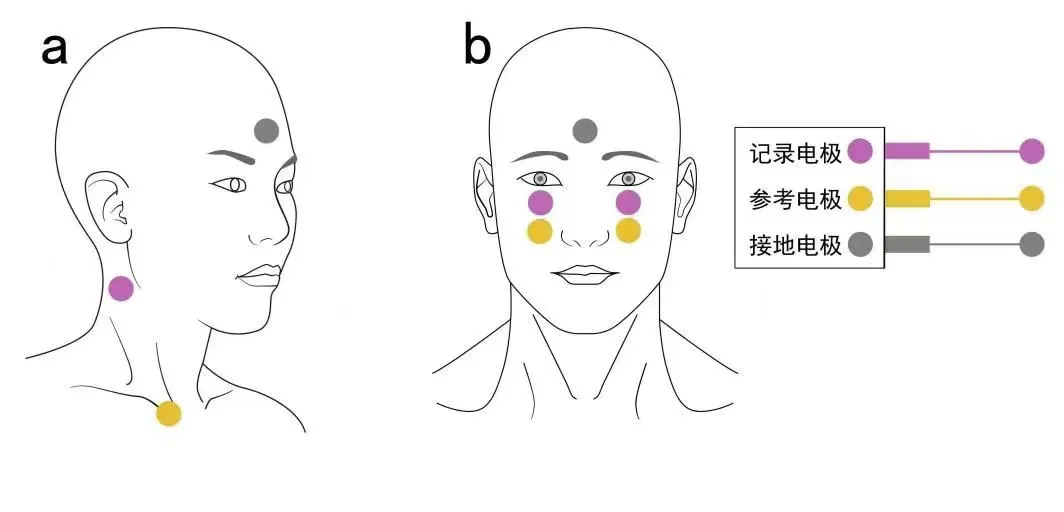
Figure2 cVEMP(a)andoVEMP(b)electrode position diagram
Result Interpretation
cVEMP waveform determination: The typical cVEMP waveform appears after the stimulus begins, showing a downward positive wave peak at approximately 13ms latency (marked as p13), followed by an upward negative wave peak at approximately 23ms latency (marked as n23) (Figure 3a).
oVEMP waveform determination: The typical oVEMP waveform appears after the stimulus begins, showing an upward negative wave peak at approximately 10ms latency (marked as n10), followed by a downward positive wave peak at approximately 15ms latency (marked as p15) (Figure 3b).
Latency is significant for waveform identification. A typical waveform is considered to exist at a specific latency under a specific stimulus intensity; if the waveform is difficult to identify or has poor repeatability after three repeated recordings at a specific stimulus intensity, it is determined that VEMP has not been evoked. Lowercase letters p and n indicate the polarity and non-neural origin of the VEMP waveform, while the Arabic numerals 13, 23, and 10, 15 represent the latencies of the waves.
Including whether the waveform is evoked, threshold (dB peSPL), p-wave latency (ms), n-wave latency (ms), inter-wave interval (ms), amplitude (µV), and interaural asymmetry ratio (IAR), etc. The minimum stimulus intensity that can evoke the VEMP waveform is defined as the threshold, the time difference from stimulus onset to the p/n wave is defined as latency, the time difference between the two waves is the inter-wave interval, and the vertical distance between the peaks of the two waves is the amplitude.
The formula for calculating IAR is: IAR=∣right ear parameter-left ear parameter∣/(right ear parameter + left ear parameter)×100%. Among the IAR values of various indicators, the amplitude IAR value is the most commonly used. IAR values range from 0 to 100%. A smaller value indicates better symmetry between the two ears, while a larger value indicates worse symmetry.
To reduce the influence of background electromyogram (EMG) on IAR, the concept of corrected amplitude has been introduced in cVEMP clinical tests: that is, the original amplitude recorded divided by the background EMG activity. Currently, there is no unified calculation method for background EMG activity; it is recommended to use the original amplitude divided by the root mean square value of the background EMG activity for 20ms before stimulation to obtain it. Usually, the root mean square value of background EMG activity can be automatically obtained by the testing instrument. If the detection system does not include this feature, it is necessary to maintain the relative balance of muscle tension on both sides of the subject during the recording process.
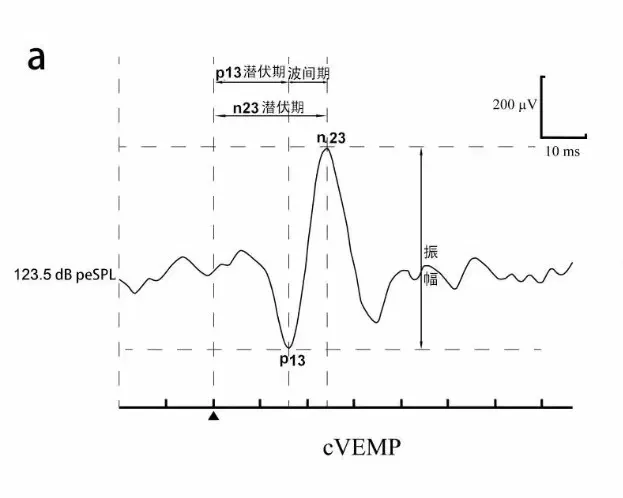
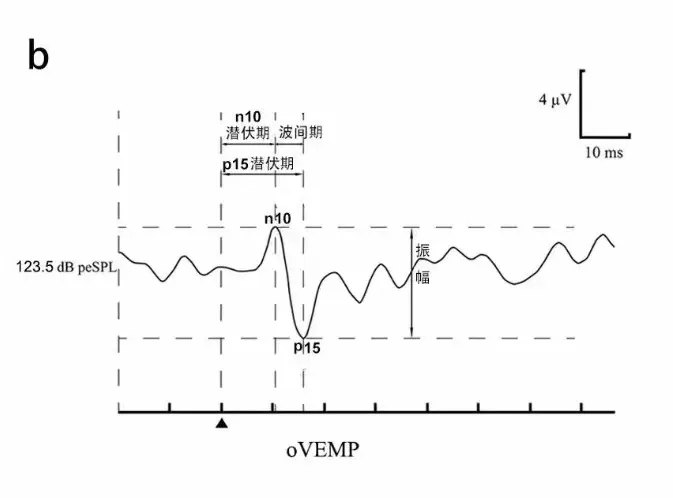
Figure3 cVEMP(a)andoVEMP(b)waveform and parameter diagram
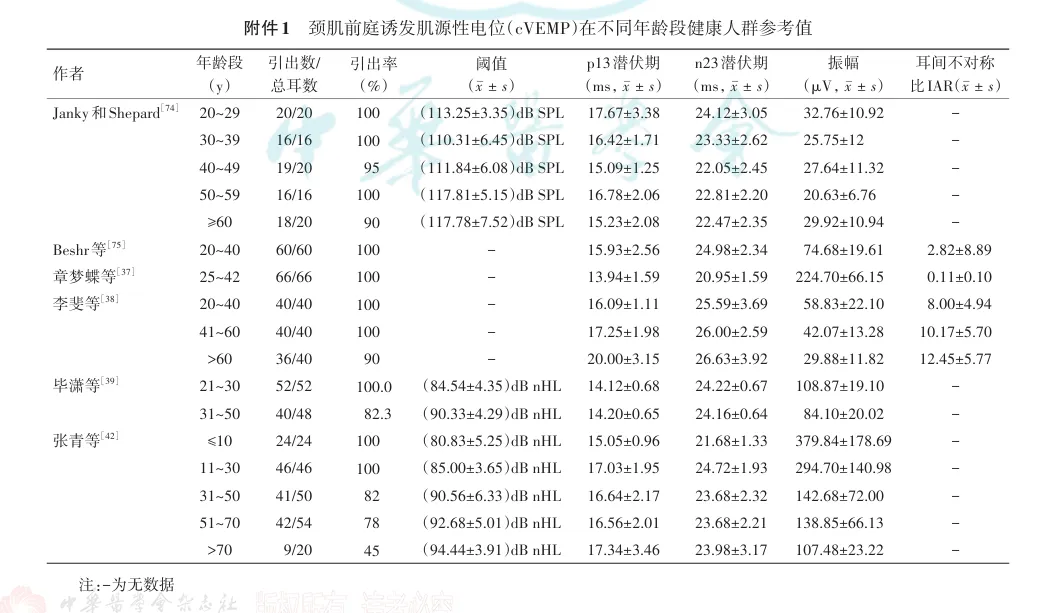
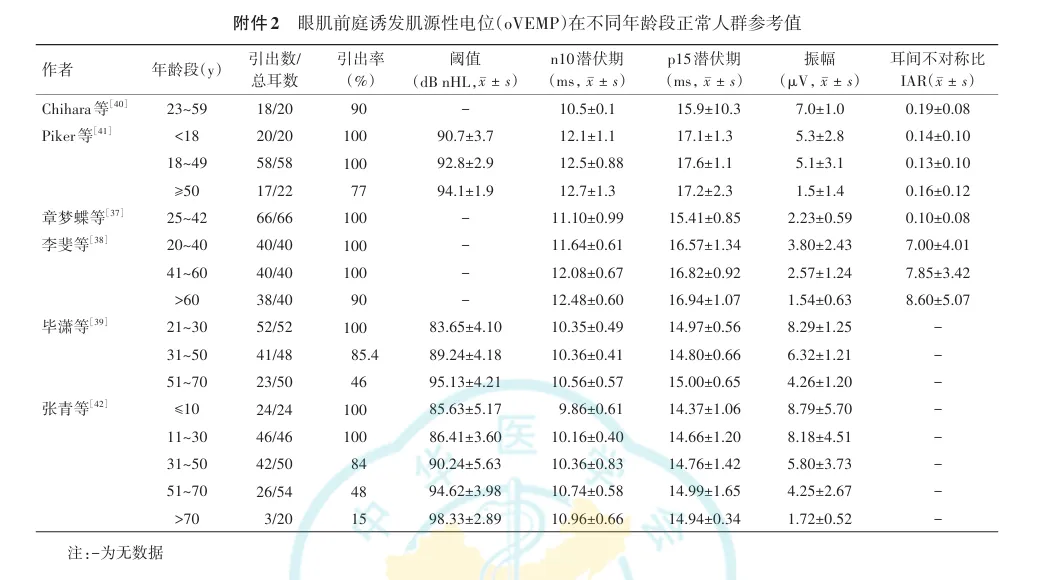
It is recommended that each institution establish its own normal reference values. Normal reference values may be affected by factors such as age, sex, race, recording equipment, and parameter settings, and these factors should be considered when establishing normal reference values. Reference values for normal populations of different age groups or genders can be described separately. Additionally, the evocation rate of VEMP significantly decreases in populations over 60 years old, which should be noted during interpretation. Previous literature on normal reference values of VEMP in populations can be found in Appendix 1.
Failure to evoke VEMP waveforms and abnormal parameters can be considered abnormal test results. Generally, in adult populations, if the amplitude IAR of cVEMP exceeds 33% or that of oVEMP exceeds 40%, it is deemed abnormal.
Clinical Applications
cVEMP and oVEMP can objectively, locationally, and quantitatively detect lesions in the “saccule-vestibular nerve-ipsilateral sternocleidomastoid muscle” and “utricle-superior vestibular nerve-contralateral inferior oblique muscle” conduction pathways, and can also dynamically monitor changes in the functional status of the vestibular otolith organ conduction pathways during the diagnosis and treatment of diseases.
Outlook
Editorial Board of the Chinese Journal of Otorhinolaryngology-Head and Neck Surgery, Audiology Group of the Otorhinolaryngology-Head and Neck Surgery Branch of the Chinese Medical Association. Clinical Practice Consensus on Vestibular Evoked Myogenic Potentials in China (2024). Chinese Journal of Otorhinolaryngology-Head and Neck Surgery [J], 2024, 59(4): 306-314.
Original link: Clinical Practice Consensus on Vestibular Evoked Myogenic Potentials in China (2024)

Welookforwardtoyourattention!
This public account willcontinue to introduce the clinical work of the Department of Otorhinolaryngology-Head and Neck Surgery of Shanghai Jiao Tong University School of Medicine and disseminate knowledge related to otorhinolaryngology-Head and Neck Surgery and promote popular science information and publish the latest developments in clinical and research progress in this field, sending the latest information and dynamics of academic conferences at home and abroad.More content, please stay tuned!
