
Introduction
01
The Anatomy of the Orbitofrontal Gyrus and Its White Matter Connections
(Click the title to see the full text)
In 1909, Brodmann first described the orbitofrontal cortex (OFC), and our understanding of the prefrontal cortex has gradually expanded into the domains of behavior and cognition.Imaging studies and animal disease models show that the prefrontal cortex plays an important role in evaluating patient prognosis and assessing surgical risk.Although intraoperative localization of language and motor function areas has become standard for surgeries in this region, it is still difficult to accurately locate areas related to executive functions intraoperatively.Neurofunctional studies indicate that the OFC and its network of white matter fiber connections are involved in human executive functions, and understanding the precise location and anatomical connections of the OFC can significantly improve postoperative functional decline.From a functional perspective, the region of interest (ROIs) refers to the area of the frontal cortex involved in reward and decision-making.From a surgical operation perspective, the region of interest is based on anatomical structures, where the OFC refers to the most anterior part of the cerebral cortex, the inferior frontal gyrus posterior lateral part, the posterior part of the insula, and the medial part of the straight gyrus.The OFC is an important center in the central nervous system for processing visual, spatial, and emotional information.Based on fiber tract anatomy, we can understand the differences in executive functions that occur in patients after resection of frontal lobe tumors.
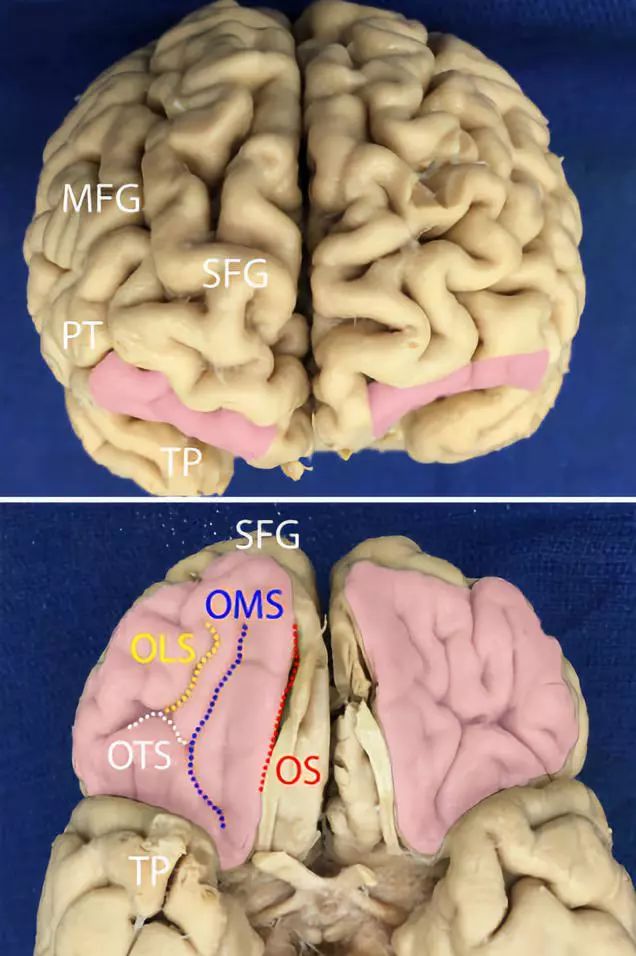
Figure 1. Above: Surface view of the OFC, located at the lower part of the superior frontal gyrus (SFG) and the medial frontal gyrus (MFG), and the triangular part of the inferior frontal gyrus (pars triangularis, PT). Below: Bottom view of the OFC, with the medial orbitofrontal gyrus located laterally to the olfactory sulcus (OS) and medially to the medial orbital sulcus (OMS, blue dashed line). The lateral orbitofrontal gyrus is located laterally to the lateral orbital sulcus (OLS, yellow dashed line) and anterior laterally to the transverse orbital sulcus (OTS, white dashed line). The anterior orbital gyrus is located between OLS and OMS. The pink area: OFC, TP: temporal pole.
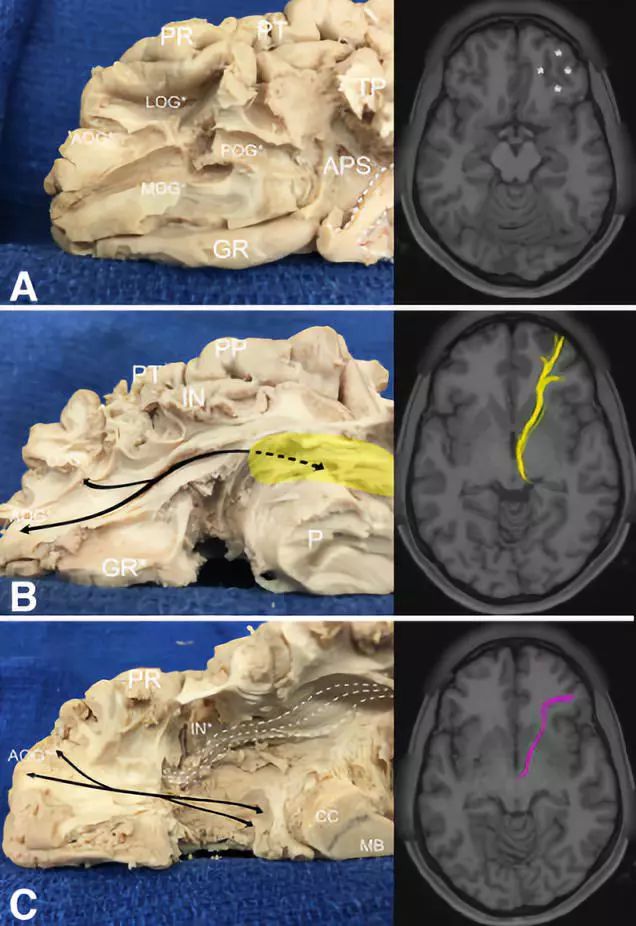
Figure 2. Connections of the orbitofrontal gyrus with the thalamus and anterior cingulate gyrus. A: Left image. The right hemisphere’s anterior blunt separation shows the connections between the orbitofrontal gyrus and surrounding structures; Right image. MRI-T1 axial image, with asterisks indicating the region of interest. B: Left image. The orbitofrontal gyrus fibers merge into the anterior medial part of the thalamic tract from the ventral precentral gyrus, with yellow indicating the connection between the orbitofrontal bundle and the thalamic tract; Right image. MRI-T1 axial image, with the yellow line representing the orbitofrontal gyrus fibers. C: Left image. The anatomy of the crossing fibers of the corpus callosum; Right image. MRI-T1 axial image, with the pink line indicating the crossing fibers of the corpus callosum.
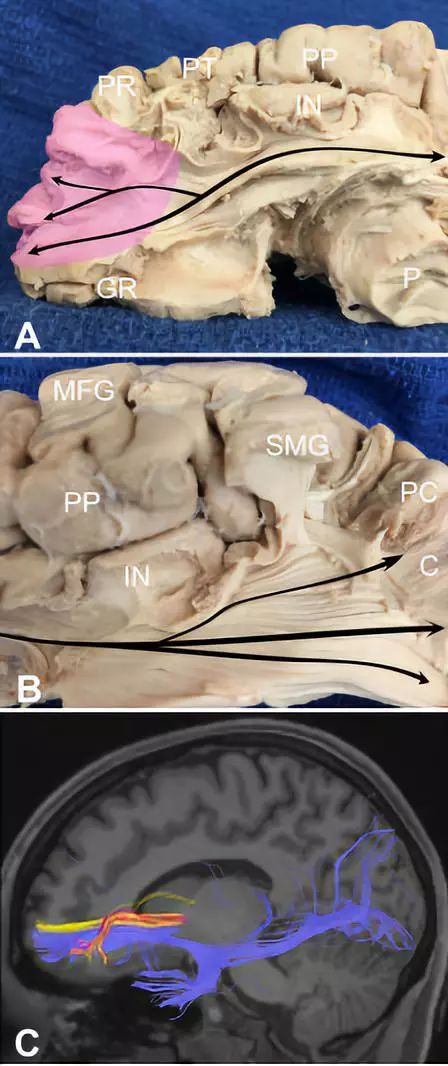
Figure 3. OFG fiber bundles projecting into the temporal, parietal, and occipital lobes. A: Sagittal fiber bundle anatomy of the right hemisphere, with pink indicating connections in OFG; B: Fiber bundles connect posterior medially with the occipital cortex; C: MRI-T1 sagittal imaging shows that the anterior frontal base fiber bundles project and distribute to the temporal, parietal, and occipital lobes.
02
The Ventral Precentral Fiber Intersection Area
Central Hub of Fiber Connections
(Click the title to see the full text)
The ventral precentral fiber intersection area (VPFIA) is an important white matter structure located in the ventral precentral gyrus, associated with language, motor, and higher cognitive functions. The white matter fiber bundles passing through the VPFIA include the anterior segment of the arcuate fasciculus (A-Arc), the long segment of the arcuate fasciculus (L-Arc), and the pyramidal pathway. By combining cadaveric dissections with diffusion tensor imaging (DTI) in healthy subjects and awake intraoperative electrical stimulation, the anatomical relationships of the VPFIA and its surrounding structures were studied. The results show that the VPFIA fiber bundles are arranged in an anterior-posterior manner: the pyramidal pathway originates ventrally in the anterior part of the precentral gyrus, the long segment of the arcuate fasciculus originates in the middle part, and the anterior segment of the arcuate fasciculus originates in the posterior part. The VPFIA is located between the dorsal language pathway and the motor cortex controlling speech-related muscles, such as the tongue, lips, and pharynx, making it an important language center in the perisylvian network. The study of the fiber bundle structure in this area is of great value for understanding the principles of language production and formulating surgical strategies for this area, and it can partly explain the phenomenon where resection of Broca’s area does not affect language function.
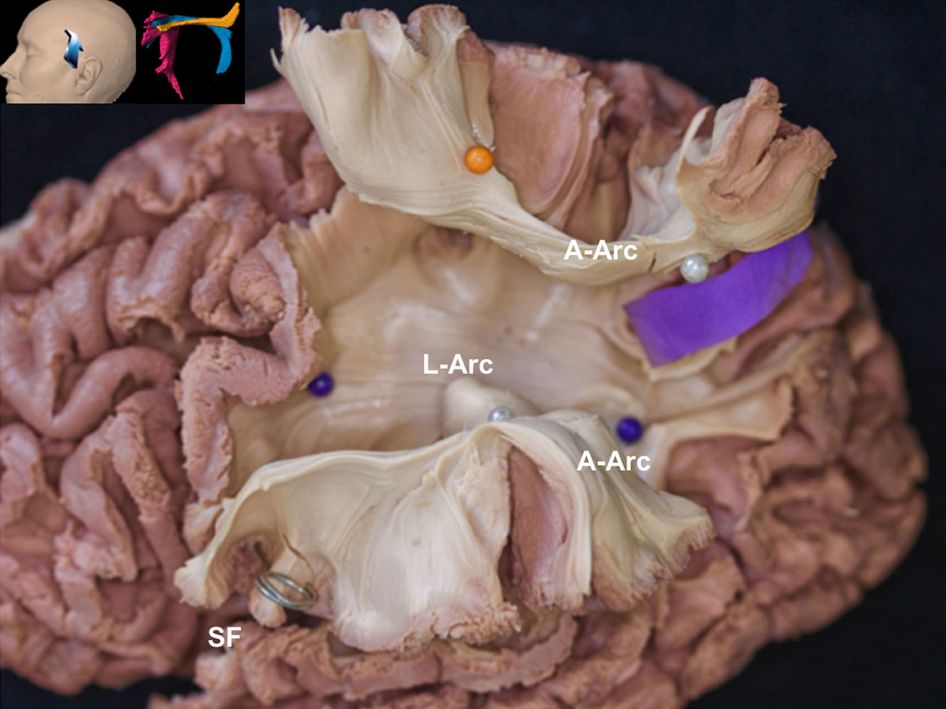
Figure 1. Anatomy of the left VPFIA white matter fiber bundles, with the upper arcuate fasciculus having been pulled up to show the deep long segment of the arcuate fasciculus. The VPFIA fiber bundles are arranged in an anterior-posterior manner. The anterior segment of the arcuate fasciculus originates from the posterior part of the ventral precentral gyrus. The long segment of the arcuate fasciculus heads towards the parietal lobe, reaching the anterior part of the precentral gyrus. A-Arc: anterior segment of the arcuate fasciculus; L-Arc: long segment of the arcuate fasciculus; SF: sylvian fissure.
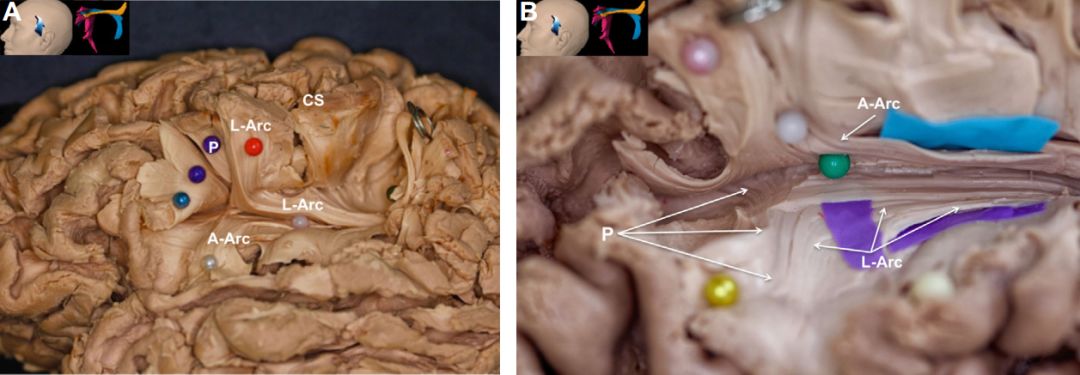
Figure 2. A. Anatomy of the VPFIA white matter fiber bundles in the left hemisphere. The ventral precentral gyrus has been opened to show the origins of various fiber bundles: the anterior segment of the arcuate fasciculus originates from the posterior part of the VPFIA; the long segment of the arcuate fasciculus originates from the middle part of the VPFIA; the pyramidal pathway is connected to the anterior part of the VPFIA. B. Another specimen of the left hemisphere, similar to figure A. CS: central sulcus; A-Arc: anterior segment of the arcuate fasciculus; L-Arc: long segment of the arcuate fasciculus; P: pyramidal pathway.
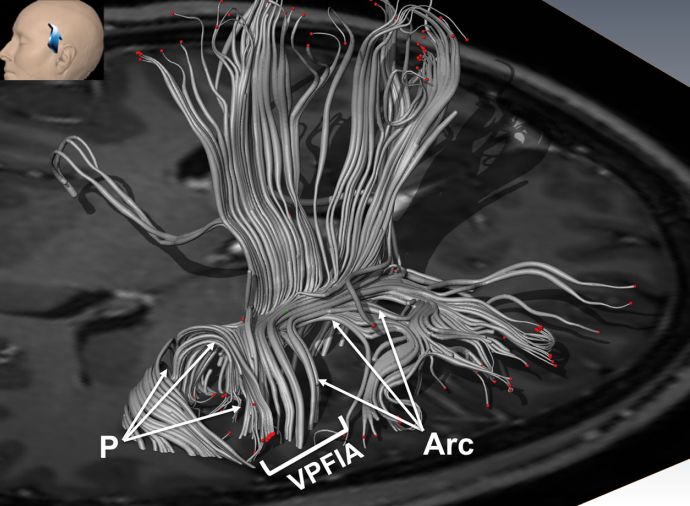
Figure 3. The VPFIA white matter fiber bundles shown in diffusion tensor imaging three-dimensional reconstruction. The pyramidal pathway is located anterior to the arcuate fasciculus. P: pyramidal pathway; Arc: arcuate fasciculus.
03
The Fiber Bundle Anatomy of the Medial and Inferior Surfaces of the Cerebral Hemisphere
(Click the title to see the full text)
Understanding the distribution and function of white matter fiber bundles in the medial and inferior surfaces of the cerebral hemisphere is extremely important for reducing neurological dysfunction when choosing surgical approaches through the cerebral longitudinal fissure and the base of the brain. Most studies focus primarily on the damage to the neurovascular structures in this area due to surgery, with less emphasis on the protection of the nerve fiber bundles. By conducting anatomical studies on the white matter fiber bundles in the medial and inferior areas of the brain, we explore the potential damage to white matter fiber bundles that may occur during midline approach surgeries, indicating that understanding the neural fiber network in the medial and inferior surfaces of the cerebral hemisphere plays an important role in surgeries along the longitudinal fissure, falx cerebri, and base.
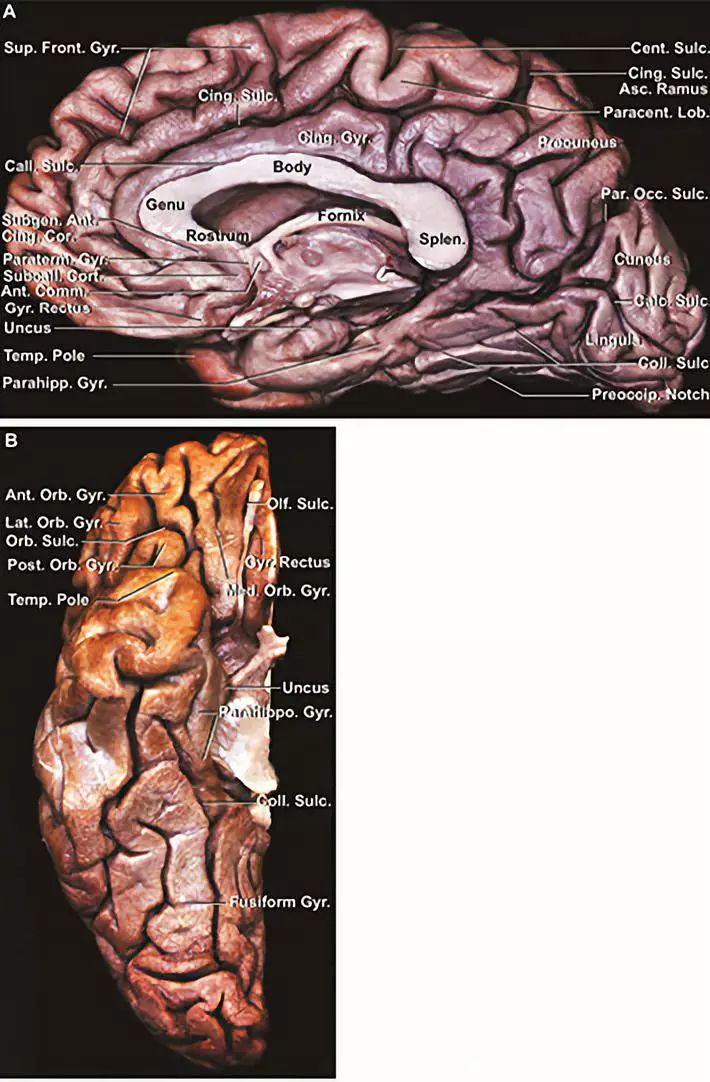
Figure 1. Anatomy of the medial and inferior surfaces of the brain. A: View of the right hemisphere from the medial side; B: View of the right hemisphere from the inferior side.
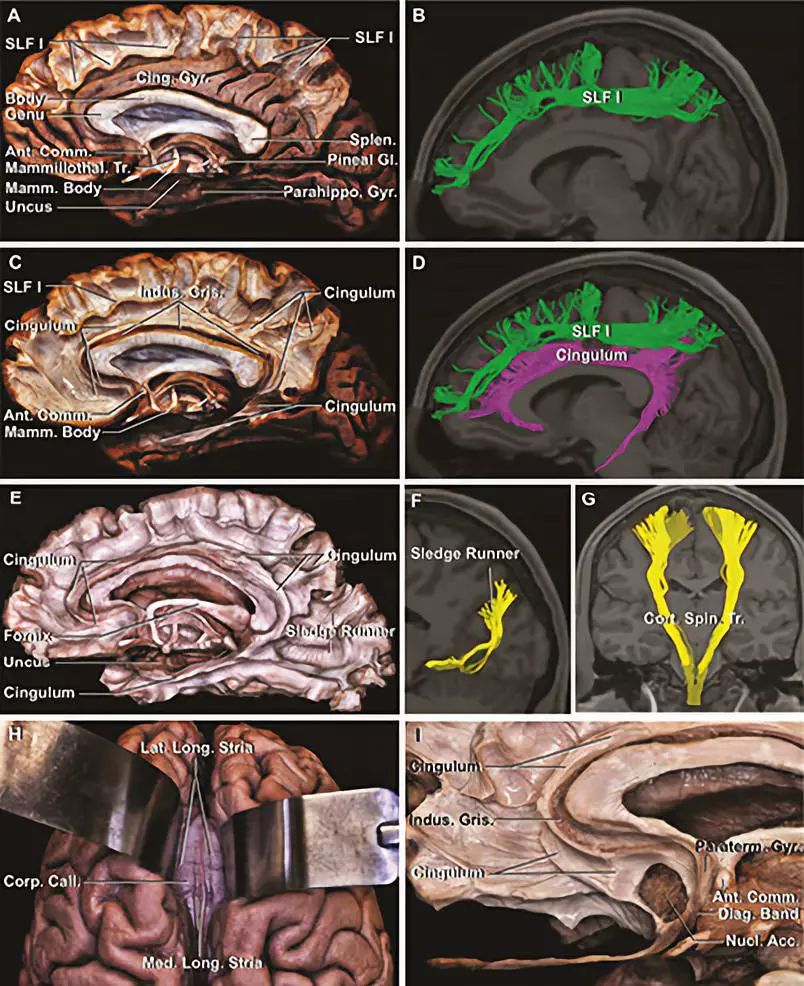
Figure 2. Anatomy of the fiber bundles on the medial surface of the right hemisphere.
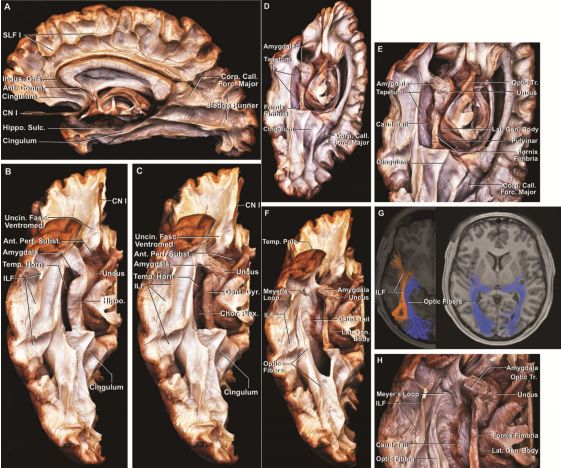
Figure 3. A. Right hemisphere medial view; B: Right hemisphere inferior view; C: Removing the hippocampal head and body exposes the dentate gyrus; D: Right hemisphere medial inferior view; E: Enlargement of figure D; F: Removal of the velum interpositum exposes the optic radiation; G: The inferior longitudinal fasciculus (orange) and the optic tract (blue); H: Enlargement of figure F.
04
The Relationship Between Brain White Matter Fiber Bundles and Lateral Ventricular Surgery
(Click the title to see the full text)
Surgery on the lateral ventricles requires cutting through several fiber bundles to reach the surgical target area. Because the lesions are located within the lateral ventricle or on any position of the ventricular wall, their deep location, combined with the variable shape and size of the lateral ventricle, and the distribution of numerous fiber bundles outside the ventricular wall adjacent to important neural structures such as the thalamus, basal ganglia, hypothalamus, and pineal gland, makes lateral ventricular surgery highly challenging. Using the anatomy of brain white matter fiber bundles and MRI fiber tract imaging technology, we explore the relationship between the neural fiber bundles and the lateral ventricle, as well as the damage caused to the lateral ventricle by surgical approaches.
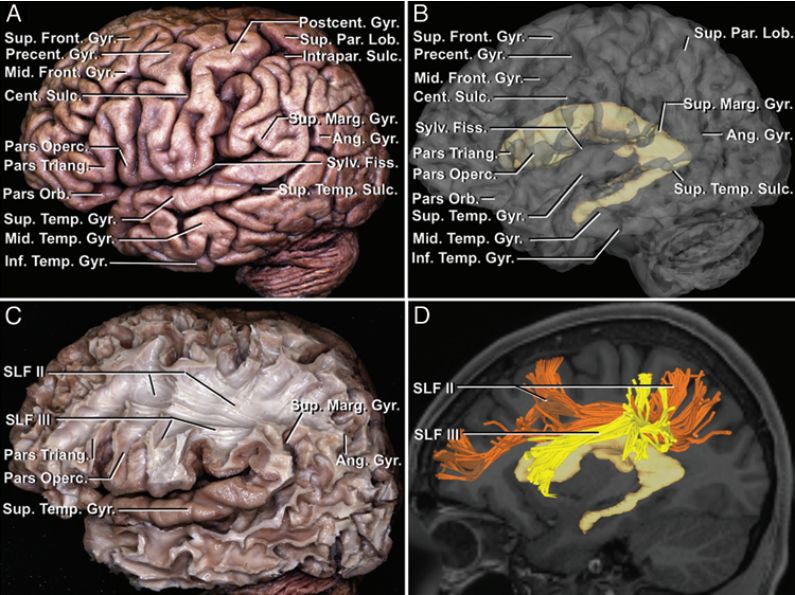
Figure 1. Anatomy of fiber bundles from outside to inside, and lateral MR fiber bundle imaging. A: Left hemisphere lateral surface of the brain with gyri and sulci; B: MRI 3D reconstruction showing the relationship between the lateral ventricle and the cortex; C: Removal of the outer cortex and short association fibers including superior longitudinal fasciculus II and III; D: MR fiber bundle imaging showing superior longitudinal fasciculus II (orange) and III (yellow), with superior longitudinal fasciculus II located on the upper lateral side of the lateral ventricle’s frontal horn, body, and atrium, and superior longitudinal fasciculus III located on the upper two-thirds of the lateral aspect of the frontal horn and body, as well as on the upper margin of the atrium.
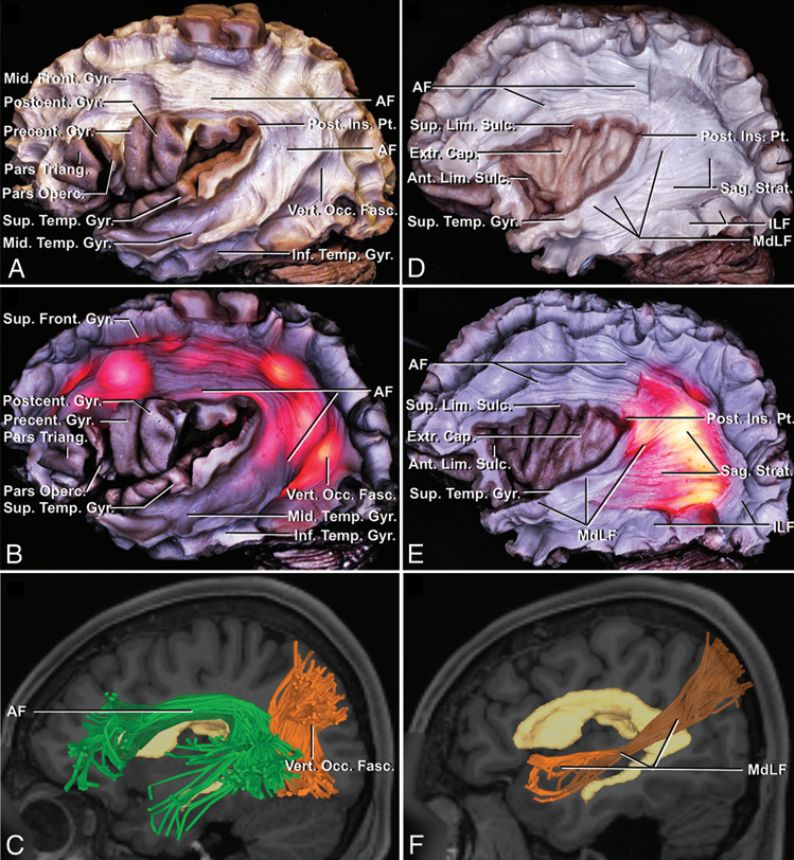
Figure 2. A: Processed specimen of the superior temporal gyrus, removing the superior longitudinal fasciculus II and III, U-shaped fibers, and exposing AF and VOF; B: Fluoroscopy placing the endoscope light source into the lateral ventricle shows the relationship between the white matter fiber bundles and the lateral ventricle; C: MR fiber bundle imaging shows the relationship between AF (green) and VOF (orange) with the lateral ventricle; D: The processed specimens of the anterior, posterior, and inferior parts of the insula show the edge of the insula. After removing the posterior part of AF, MdLF and ILF are exposed, and after removing the insular cortex, the outer capsule is exposed; E: Fluoroscopy shows the relationship between MdLF and ILF with the lateral ventricle; F: MR fiber bundle imaging shows the relationship of MdLF (orange) with the lateral ventricle.
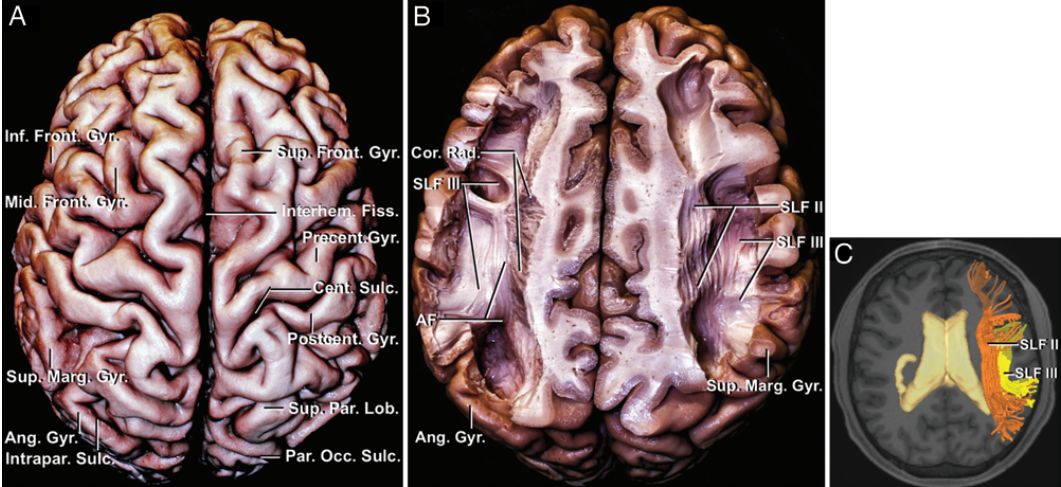
Figure 3. A: The brain’s upper surface with gyri and sulci; B: Superior longitudinal fasciculus II and III (superior view); C: MR fiber bundle imaging shows the relationship of superior longitudinal fasciculus II (orange) and III (yellow) with the lateral ventricle.
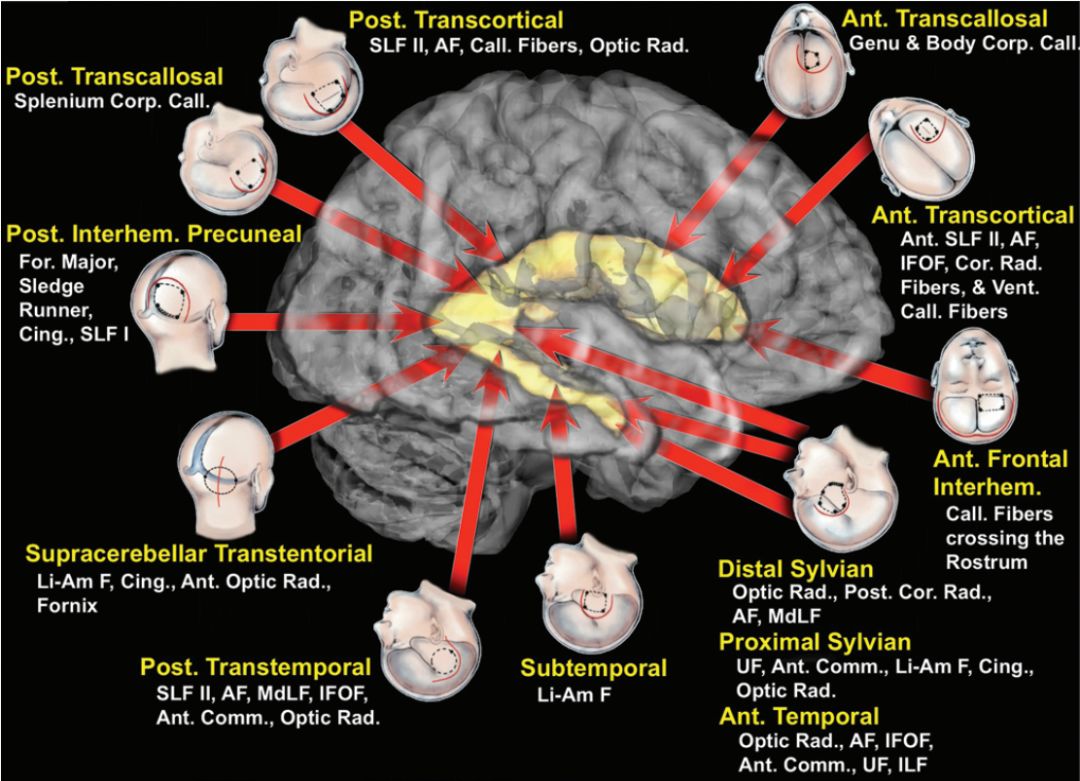
Figure 4. A: The superior longitudinal fasciculus I extends from the precuneus to the anterior part of the superior frontal gyrus and the middle part of the corpus callosum, while the cingulum runs above the corpus callosum and below the superior longitudinal fasciculus I, terminating near the pressure and knee of the corpus callosum; B: Fluoroscopy shows the cingulum and the superior longitudinal fasciculus I running along the lateral ventricle’s atrium, body, and frontal horn; C: MR fiber bundle imaging shows the relationship of the arcuate fasciculus (green) with the lateral ventricle.

Figure 5. Various surgical approaches for lesions within the lateral ventricle. The main surgical approaches include the anterior approach, posterior approach, posterior longitudinal fissure approach via the corpus callosum, posterior longitudinal fissure approach via the precuneus, the upper cerebellum approach via the lateral recess of the cerebellum, the paramedian upper cerebellum approach via the cerebellar tentorium, and the lateral approach.
The study clarifies the adjacency relationships between the lateral ventricle and the superior longitudinal fasciculus I, II, III, arcuate fasciculus, vertical fasciculus, middle longitudinal fasciculus, inferior longitudinal fasciculus, uncinate fasciculus, cingulum, corpus callosum, fornix, caudate nucleus, thalamus, and stria terminalis, which are related to the lateral ventricle. Understanding the relationship between brain white matter fiber bundles and the lateral ventricle helps to more accurately handle lesions within the lateral ventricle surgically.
05
Research on Identifying White Matter Fiber Conduction Pathways
(Click the title to see the full text)
Gliomas are characterized by diffusion and infiltration, making complete tumor resection challenging. The goal of brain tumor resection is to maximize tumor removal while preserving language, motor functions, and vision. Therefore, locating functional brain areas and identifying white matter conduction pathways are crucial for reducing patient morbidity. By utilizing diffusion tensor imaging (DTI) and fiber tract imaging technology with MRI, it is significant for clarifying the orientation of white matter fiber bundles and guiding the extent of glioma resection, providing an automated fiber bundle recognition model for patients with imaging bias caused by tumor edema and infiltration, thus enhancing the safety of tumor removal. The automated fiber bundle recognition model used to guide glioma surgery can improve the safe removal of tumors.
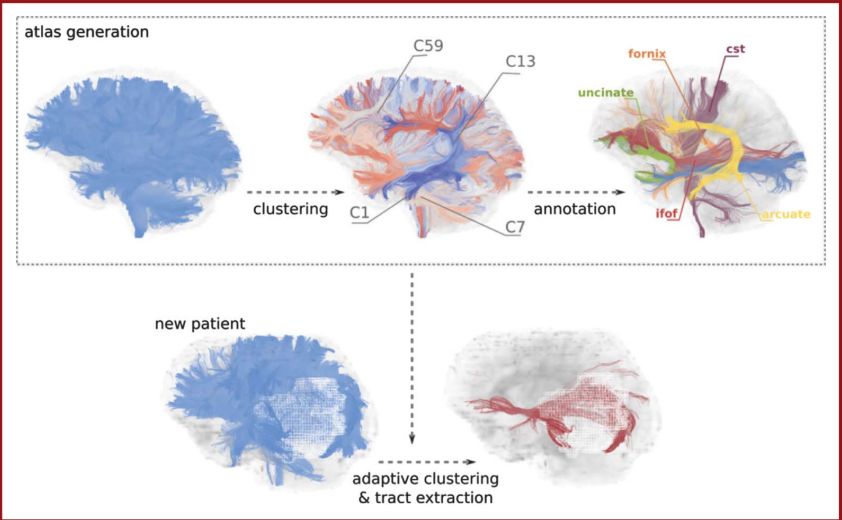
Figure 1. Steps for automated recognition of fiber bundles. The white matter fiber bundle map is formed from the fiber bundle clustering model of healthy participants. The same fiber bundle clustering model map is used for automated matching of fiber bundles in different tumor patients.
Postoperative white matter fiber bundles are severely deformed, but the white matter fiber bundles within the internal capsule can still be clearly identified (Figure 2).

Figure 2. From left to right, the first image: Schematic diagram of white matter fiber bundles within the internal capsule; the second image: White matter fiber bundles of healthy participants; the third image: White matter fiber bundle map of patients with surgical history.
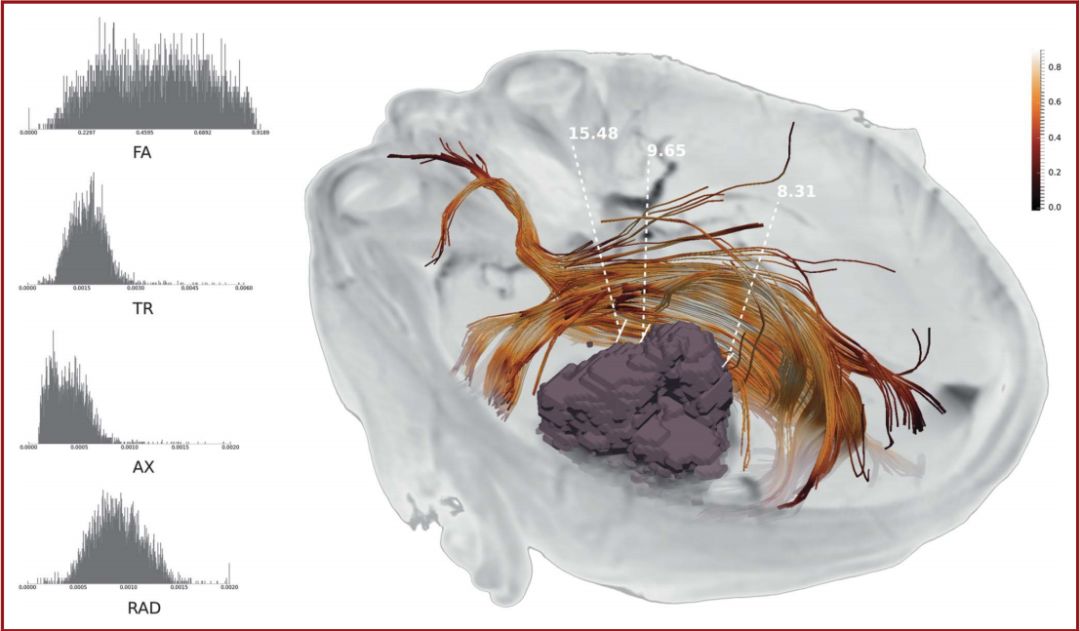
Figure 3. Schematic diagram of the tumor and surrounding white matter fiber bundles (IFOF).
06
High-Resolution Fiber Tract Imaging Shows Clear 12 Pairs of Cranial Nerves
(Click the title to see the full text)
High-resolution fiber tract imaging technology (HDFT), utilizing diffusion spectrum imaging (DSI) to acquire images, can accurately reproduce multiple crossing fiber bundles in 3D, significantly improving imaging resolution and providing detailed spatial tracing images of cranial nerve (CN) pathways. By applying HDFT in healthy individuals and patients with intracranial tumors, we can precisely reconstruct the neural fiber bundles of the CNs, showing the spatial tracing images of the 12 pairs of cranial nerve fiber bundles. Preoperative reconstruction of cranial nerve fiber bundles using HDFT technology helps to understand the complex fiber bundle orientations and crossing conditions, providing a basis for predicting CN displacements caused by skull base tumors and formulating surgical resection plans.
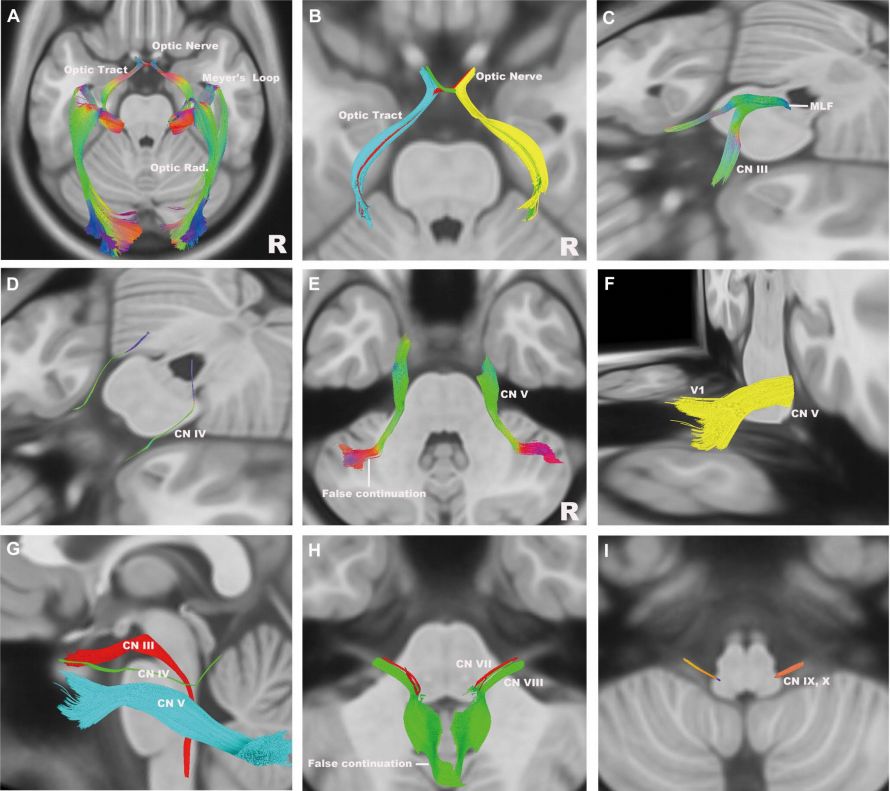
Figure 1. Using HDFT technology to display 12 pairs of cranial nerves on the MRI diffusion imaging structural template within the human neural connectivity project database. A. Visual pathway (axial view); B. Close-up of the optic chiasm (axial view), with blue and yellow representing the temporal visual tract, green and red representing the nasal visual tract; C. Oculomotor nerve (oblique view); D. Trochlear nerve (oblique view); E. Trigeminal nerve (axial view), with the medial fiber bundle in the brainstem not fully reconstructed; F. Trigeminal nerve (oblique view), with incomplete reconstruction of trigeminal nerve branches; G. Oculomotor nerve, trochlear nerve, and trigeminal nerve (close-up and axial view); H. Facial nerve and vestibulocochlear nerve (axial view); I. Glossopharyngeal nerve and vagus nerve. MLF: medial longitudinal fasciculus.
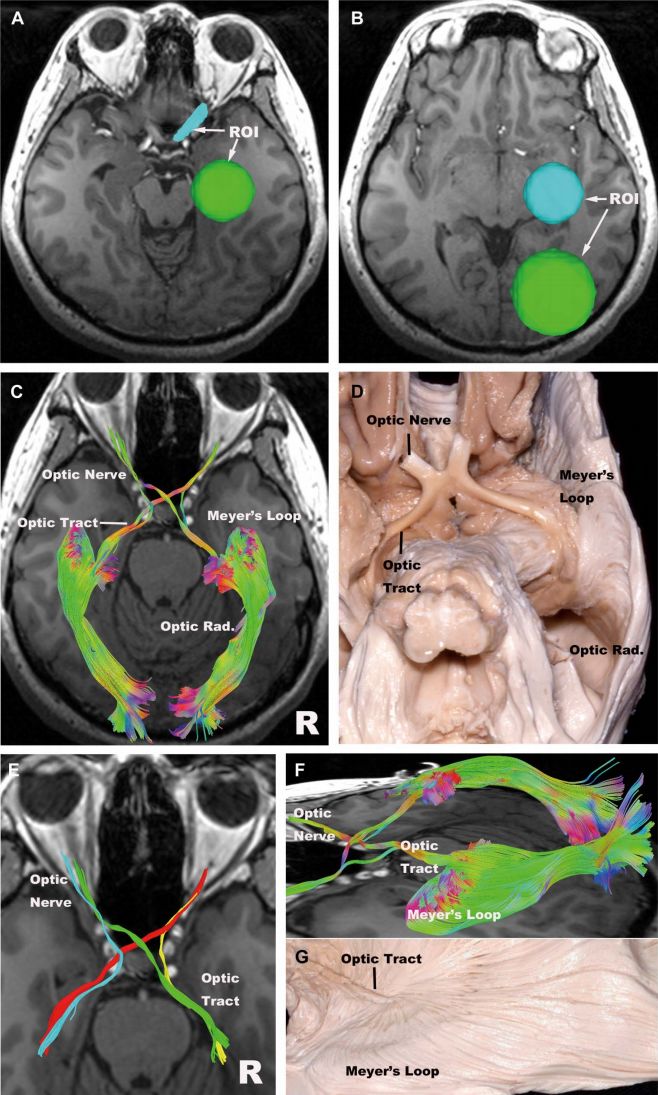
Figure 2. The optic nerve. A. ROIs are placed on the optic nerve and lateral geniculate nucleus; B. ROIs are placed on the lateral geniculate nucleus and occipital lobe; C. Visual pathway, reconstructing the nasal visual nerve, temporal visual nerve, optic chiasm, optic tract, and complete visual radiation, including Meyer’s loop, the intermediate bundle, and the dorsal bundle; D. Corresponding anatomical diagram (view from below in C); E. Optic chiasm, with blue and yellow representing the temporal visual tract, green and red representing the nasal visual tract; F. Visual radiation; G. Corresponding anatomical diagram (side view in F).
07
Microanatomy of the Central Core Region of the Brain
(Click the title to see the full text)
The central core is located deep within each cerebral hemisphere, serving as the dividing line between the brainstem and the cerebral lobes, primarily composed of the surface of the insula, basal ganglia, and thalamus. It also contains parts of the anterior commissure, amygdala fibers, and the insular cortex. The central core connects to other structures above the tentorium through the cerebral isthmus, which consists of the internal capsule, external capsule, and outer capsule fibers. The central core is responsible for the integration of information in the brain and plays an important role in motor, sensory, emotional, and cognitive functions; thus, understanding the concept of the central core is greatly beneficial for better understanding surgeries in this region. The central core is divided into quadrants, detailing its cortical and subcortical anatomical structures, determining its boundaries, especially the morphology and adjacency of the thalamus, basal ganglia, associated fiber bundles, and blood vessels. Different surgical approaches are employed for lesions in different quadrants, which has significant guiding value for surgeries.
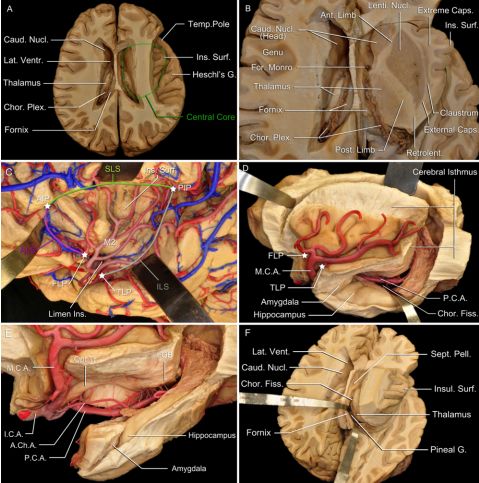
Figure 1. The brain’s central core. A: Horizontal axial section of the medial frontal gyrus, removing the surface of the insula, exposing the central core, with the caudate nucleus and thalamus on the medial side and the surface of the insula on the lateral side; B: Through the axial section of the central core, it is seen to consist of the basal ganglia and fiber bundles, which gather from within the central core, forming the outer capsule, external capsule, and internal capsule based on their positional relationships with the basal ganglia; C: Separating the sylvian fissure, retracting the insular cover exposes the insula, which is triangular in shape, bounded by the anterior, superior, and inferior circular sulci, with its anterior inferior vertex being the insular threshold. The convergence points of these sulci are the anterior insular point (intersection of the anterior and superior circular sulci), the posterior insular point (intersection of the superior and inferior circular sulci), the frontal threshold point (intersection of the insular threshold and anterior circular sulcus), and the temporal threshold point (intersection of the insular threshold and inferior circular sulcus); D: Making a deep incision around the insular sulcus exposes the lateral ventricle, separating the central core from other structures in the cerebral hemisphere; E: The choroidal fissure is a natural fissure between the fornix and thalamus, also separating most of the medial structures of the temporal lobe from the central core.
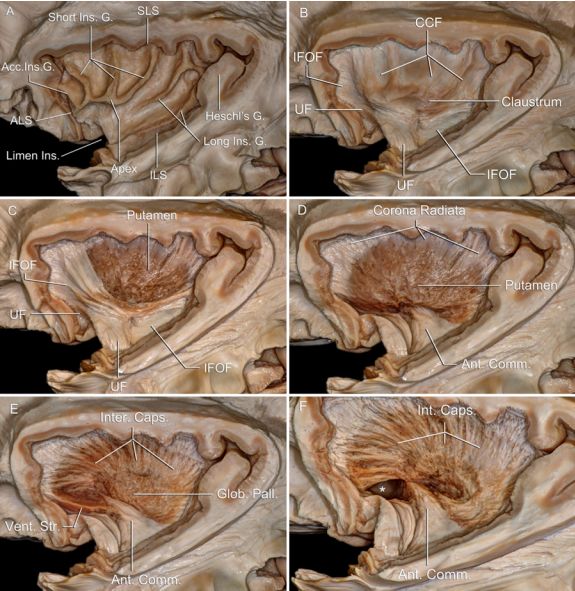
Figure 2. Anatomy of the lateral fiber bundles of the central core. A: Lateral view after removing the insular cover; exposing the outer capsule, with attention to the short insular gyrus and the accessory insular gyrus located at the anterior part of the insula, which converge at the apex of the insula, while the long insular gyrus does not converge; B: Dissecting deeper, removing the insular gyrus and outer capsule. Exposing the claustrum and distinguishing important fiber bundles: the uncinate fasciculus and inferior occipital fasciculus arising from the ventral claustrum; C: The claustrum-cortical fibers arise from the dorsal claustrum, removing to expose the putamen below. Note that the uncinate fasciculus and inferior occipital fasciculus converge below the apex of the insula, which serves as a cortical landmark for these two fiber bundles; D: Removing the uncinate fasciculus and inferior occipital fasciculus exposes the external lateral of the anterior commissure; E: Removing the putamen exposes the pallidum below it. The anterior commissure crosses the longitudinal fissure, extending outward, forming a fiber bundle that crosses the midline to connect the two cerebral hemispheres; F: Removing the pallidum exposes the entire internal capsule. The fiber bundles that leave the central core become part of the corona radiata.

Figure 3. The anatomy of the medial fiber bundles of the central core. A: Medial view of the brain, where the central core cannot be directly presented, but some boundary structures of the central core can be seen. The septal area, fornix, third ventricle, and the head and body of the lateral ventricle are located medially to the central core. The corpus callosum and anterior commissure surround the central core, forming a joint fiber bundle that crosses the midline connecting the two cerebral hemispheres; B: Removing the thalamus reveals the fiber bundles within the central core.
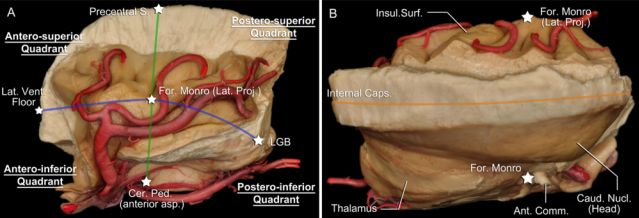
Figure 4. Blood supply to the central core. A: Lateral view, removing all lobes of the brain, revealing the central core above the brainstem. The middle cerebral artery arises from the internal carotid artery, first passing below the central core (M1 segment), then bending to the surface of the insula (M2 segment). Branches from the M2 segment of the middle cerebral artery supply the outer structures of the central core, namely the surface of the insula, outer capsule, claustrum, and external capsule; B: Removing the left central core reveals the relevant arteries. The lenticulostriate artery arises from the M1 segment of the middle cerebral artery, and the thalamoperforating artery arises from the tip of the basilar artery and the proximal segment of the posterior cerebral artery; C: The posterior choroidal arteries arise from the proximal segment of the posterior cerebral artery, entering the lateral ventricle, while the anterior choroidal arteries surround the posterior and superior parts of the central core, supplying blood to this area; D: Lateral view of the central core, removing the surface of the insula, outer capsule, claustrum, and external capsule. The lenticulostriate artery passes towards the lentiform nucleus; E: The lenticulostriate artery forms anterior and posterior arterial pedicles, with the anterior pedicle continuing towards the putamen and the posterior pedicle entering the globus pallidus; F: The view of the central core from above, removing the caudate nucleus.
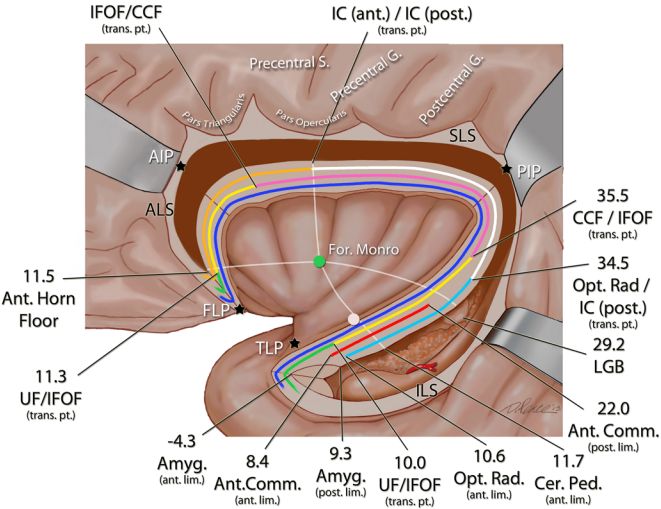
Figure 5. The subdivision of the central core. A: Lateral view, dissecting the central core. According to the vertical line (green) and horizontal line (blue) in the figure, the central core is subdivided into four quadrants, with the intersection of the two lines representing the lateral projection point of the interventricular foramen. The vertical line is the connection between the most anterior part of the precentral gyrus and the brainstem, indicating the anterior edge of the pyramidal tract, suggesting to the surgeon that there are pyramidal tract fibers of the internal capsule running in the deep posterior quadrant. The horizontal line is the connection from the bottom of the anterior horn of the lateral ventricle to the lateral geniculate nucleus, suggesting that when dealing with lesions in the anterior horn and body of the lateral ventricle, the surgical approach should be above this level; the lateral approach to the third ventricle should be chosen in the lower posterior quadrant, while the approach to the anterior perforated substance should be selected in the lower anterior quadrant; B: View of the central core from above. The orange line represents the connection along the caudate nucleus (above) and the lenticulostriate artery (deep), which represents the sagittal sinus plane, which should not be crossed or damaged during surgery. If the lesion is located laterally to this plane, the approach should be from the lateral side of the insula; if the lesion is located medially, the approach should be from the medial side of the insula.
08
The Microanatomy and Surgical Approaches of the Cerebral Central Core Region
(Click the title to see the full text)
The cerebral central core region (CCC) has different subdivisions, including important deep brain structures and adjacent brain pools and ventricles, which are significant in neurosurgical procedures. Through cadaveric studies, the cortical and subcortical structures of the cerebral central core region are microscopically dissected, providing detailed descriptions of the boundaries, cortical, and subcortical microanatomical structures of the cerebral central core region. The paths of blood vessels and nerve fiber bundles are observed, and various neurosurgical approaches are proposed. Through percutaneous insular ultrasound for locating the interventricular foramen, data on tumors in the central core region can be obtained, helping to reduce the incidence of postoperative complications.
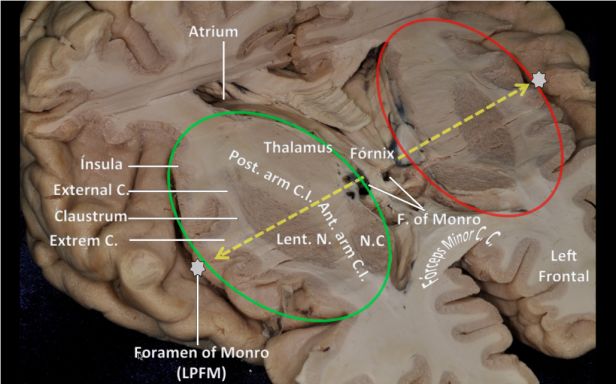
Figure 1. The anterior surface of the CCC is an imaginary plane extending from the anterior circular sulcus, crossing the anterior edge of the caudate nucleus, with the upper limit at the anterior horn of the lateral ventricle and the lower limit at the anterior edge of the septal area.
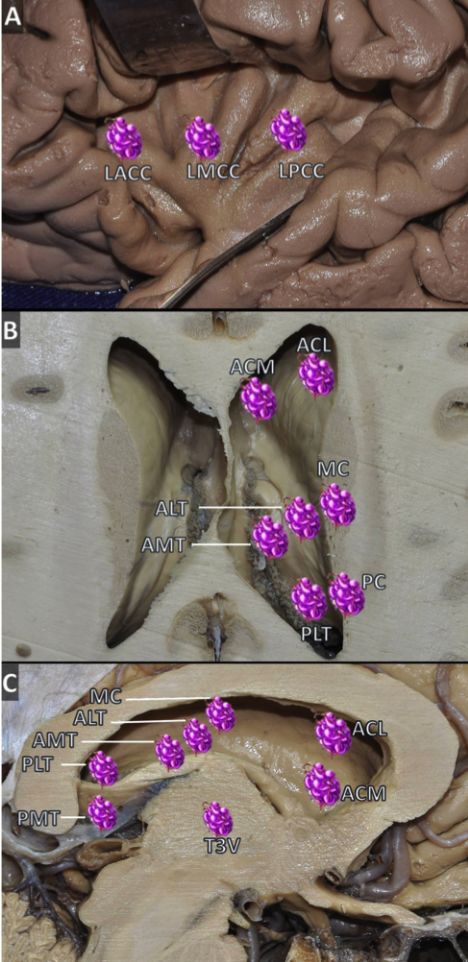
Figure 2. Schematic diagram of fine subdivisions of the cerebral central core region. A: Opening the lateral fissure reveals the surface of the insula, showing the anterior lateral core area, middle lateral core area, and posterior lateral core area; B: Axial brain slice above the lateral ventricle, showing the dorsal surface in the middle of the CCC; C: Sagittal brain slice showing the middle part of the CCC.
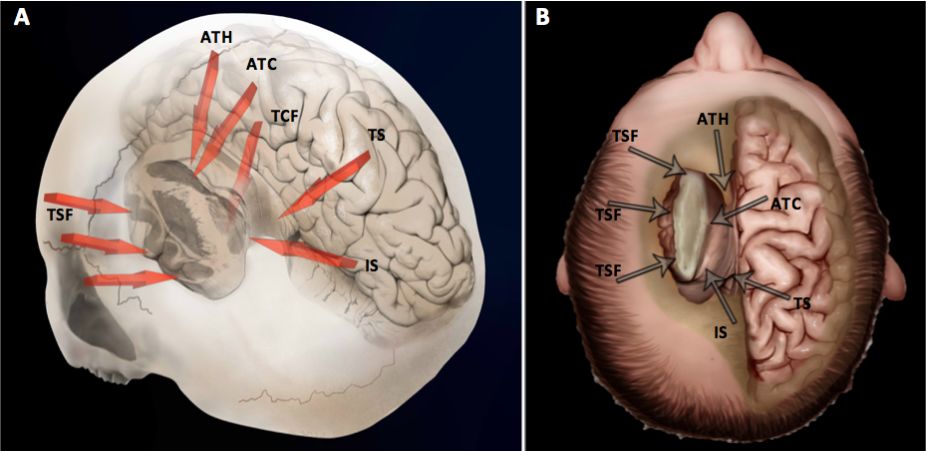
Figure 3. Schematic diagram of surgical approaches to the left cerebral central core region. Based on the anatomical analysis of the CCC, six surgical approaches are proposed: ipsilateral approach through the corpus callosum, contralateral approach through the corpus callosum, approach through the choroidal fissure, approach through the cingulum, approach through the medial sulcus, and approach through the lateral fissure.

-
Special Topic on Neurosurgery (I) | Literature Review of Intracranial Tumors
