

Transcatheter Left Atrial Appendage Occlusion (LAAO) is an effective method for preventing stroke in patients with atrial fibrillation and has been widely used in clinical practice in recent years. However, there are still some challenges with LAAO, among which device-related thrombosis (DRT) after the procedure is an important concern. Previous studies have shown that the incidence of DRT after LAAO is 3.0-4.0%, which increases the risk of thromboembolic events.
Currently, the predictive factors for DRT are still limited to small sample sizes or single-center studies. Recently, the Journal of the American College of Cardiology (JACC) published results from an international multicenter clinical study on predictive factors for DRT, which is worth referencing.
The study included 237 patients with DRT from 37 centers (DRT group), with each patient matched with 2 patients from the same center who had the same type of occluder implanted and no DRT after the procedure (control group, n=474). The objectives of the study included: (1) DRT management strategies; (2) mid-term follow-up results, including major adverse cardiovascular events (MACE), bleeding events, and intracranial hemorrhage; (3) predictive factors for DRT. The DRT group had a higher proportion of hypertension, heart failure, previous stroke, history of venous thromboembolism, hypercoagulable state diseases, and non-paroxysmal atrial fibrillation compared to the control group (Table 1). There were no significant differences in the left atrial appendage morphology between the two groups, with approximately 80% of patients undergoing transesophageal echocardiography-guided procedures, and 74% of patients implanted with the Watchman occluder (Figure 1 and Table 2). The DRT group had a deeper occluder implantation position (12.0±8.4mm vs. 8.2±6.5mm, P<0.001) and a higher incidence of pericardial effusion during the perioperative period (3.4% vs. 0.6%, P=0.01) (Table 2).
Table 1: Baseline Characteristics of Patients
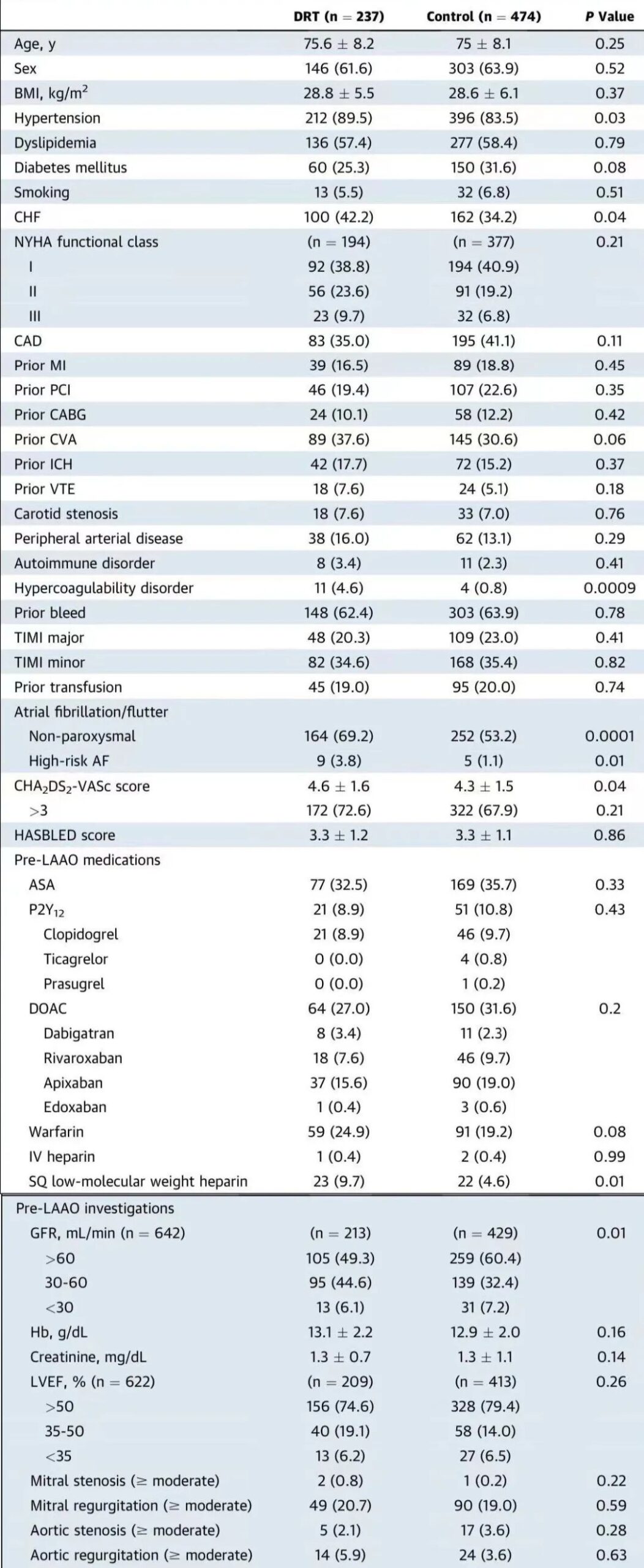
Table 2: Surgical Data of Patients
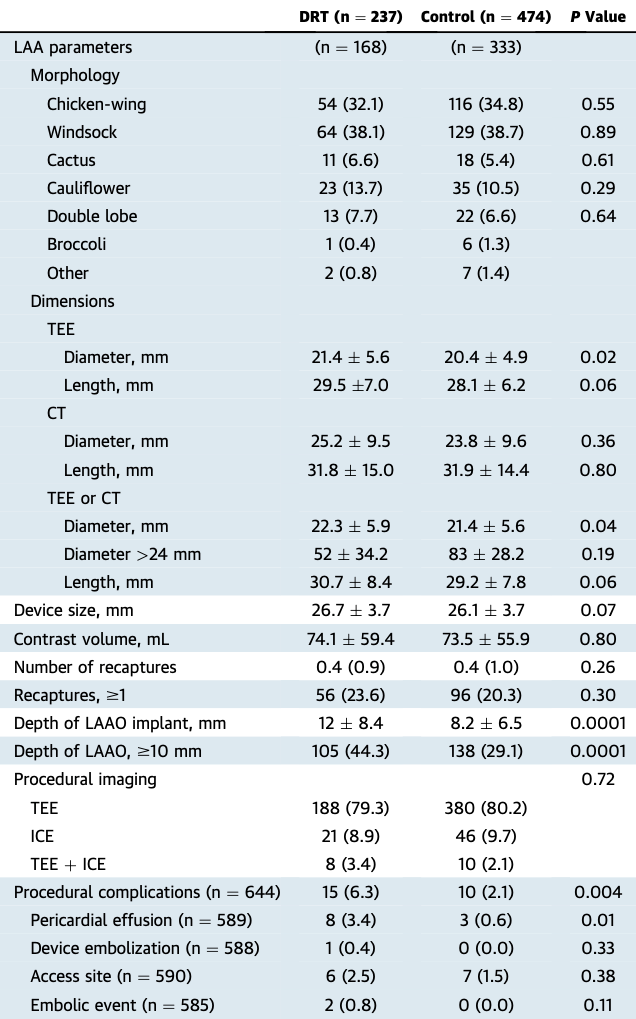
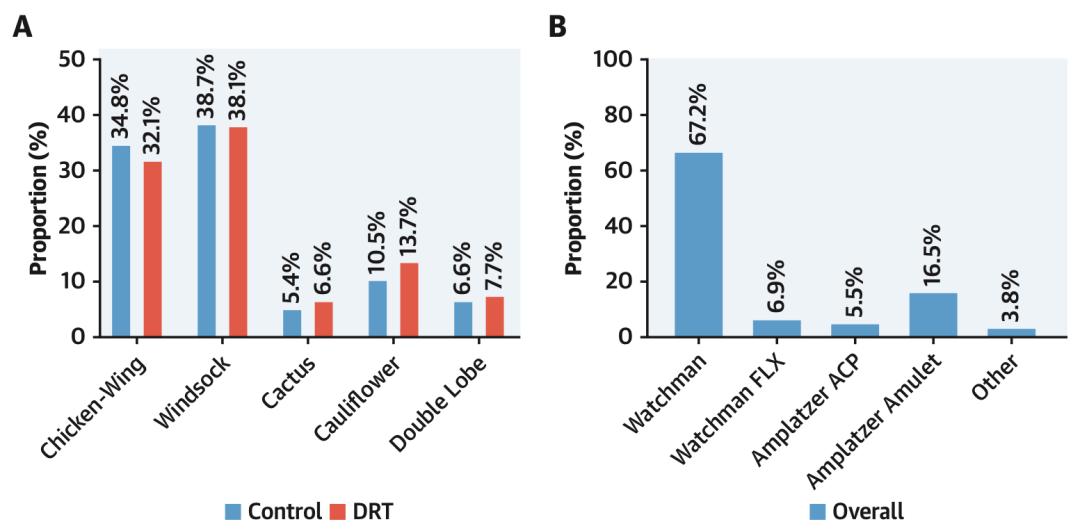
Figure 1: Morphology of the left atrial appendage in the two groups (A) and distribution of occluder types (B).
During follow-up, the DRT group had higher rates of device displacement (2.7% vs. 0.0%, P=0.002) and residual shunting from the occluder (34.6% vs. 26.1%, P=0.005) (Table 3). The proportions of DRT found at postoperative <45d, 45-180d, 180-365d, and >365d were 24.9%, 38.8%, 16.0%, and 20.3%, respectively. The DRT group underwent imaging examinations more frequently and had a higher incidence of MACE (Figure 2). There were no statistical differences in the choice of antithrombotic drugs between the two groups after surgery, with most patients using single antiplatelet therapy (36.3%) or dual antiplatelet therapy (26.2%) when DRT was detected, followed by a significant increase in anticoagulation therapy, but 25.3% of patients still had DRT at the last follow-up (Figure 3). The median follow-up times for the DRT group and control group were 1.8 years and 1.6 years, respectively, with the DRT group having a higher incidence of MACE (29.5% vs. 3.6%, HR=3.49, P=0.01), where the incidence of ischemic stroke was also higher in the DRT group (16.9% vs. 3.6%, HR=3.49, P=0.01), while there were no significant differences in all-cause mortality and systemic embolism rates between the two groups (Figure 4). Additionally, the rates of bleeding events and intracranial hemorrhage were comparable between the two groups (Figure 5). For patients with both DRT and ischemic stroke, the study found that 59% of DRT cases were detected before the stroke occurred (Figure 6).
Table 3: Follow-up Data of Patients
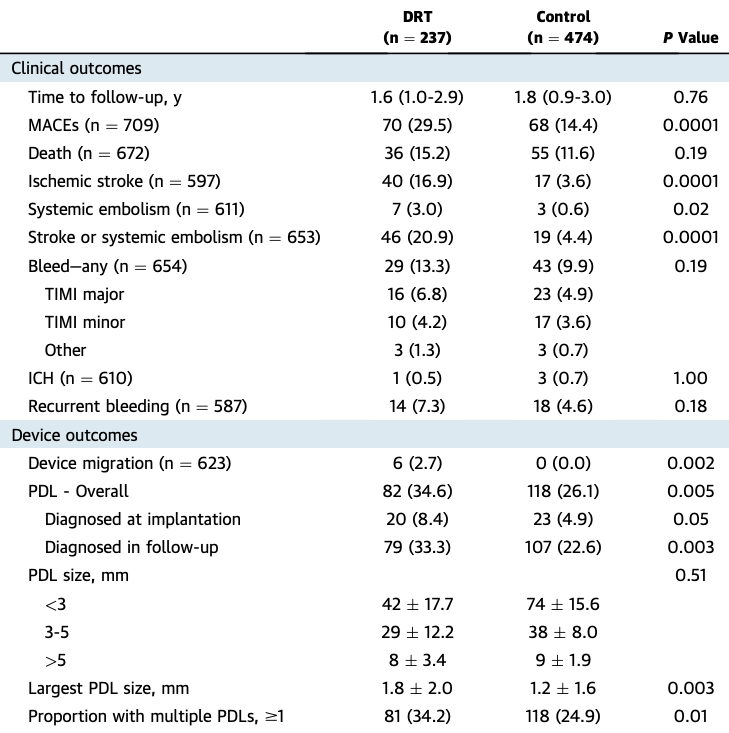
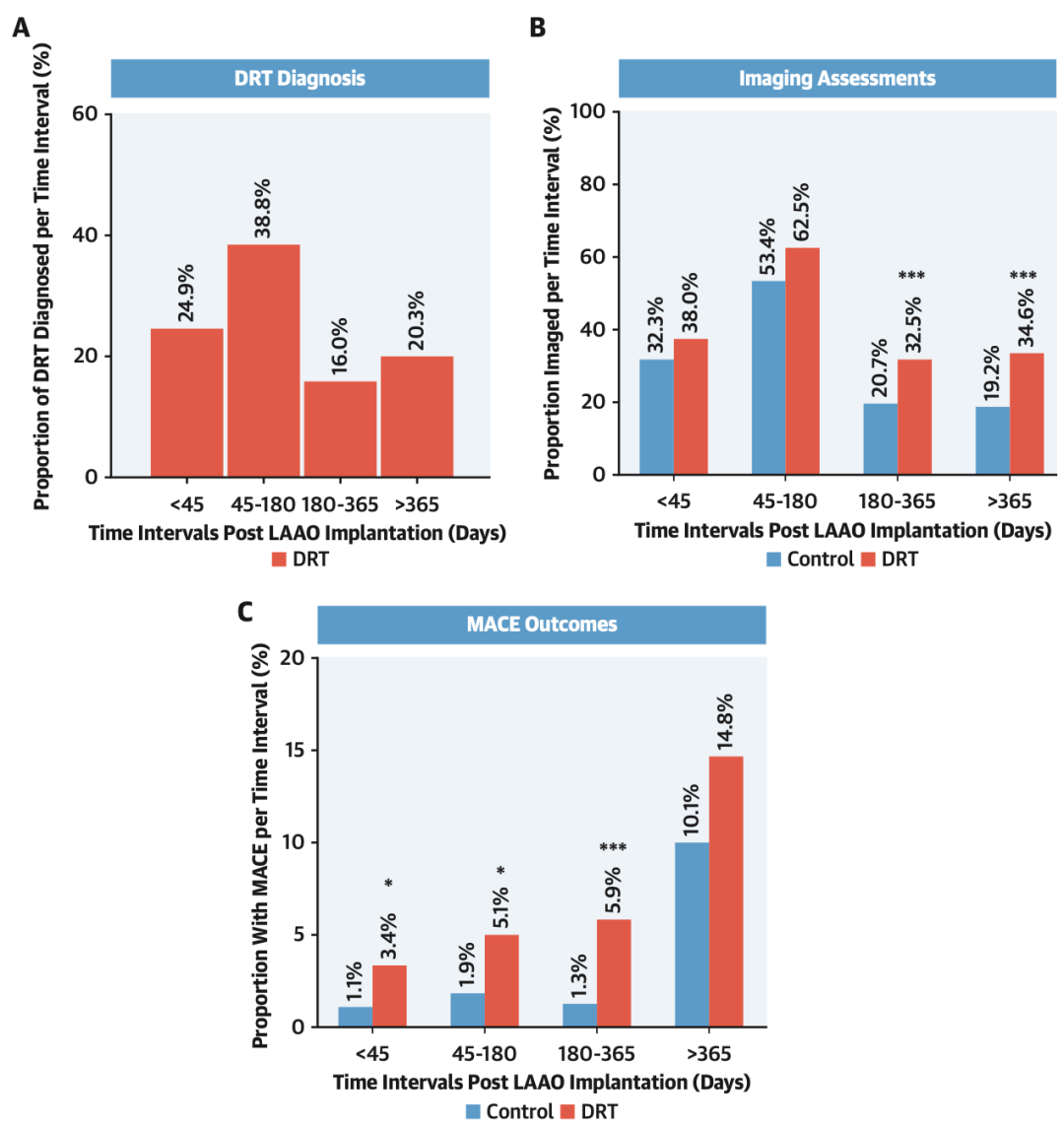
Figure 2: Time points for DRT diagnosis (A), imaging follow-up rates (B), and incidence of MACE events (C).
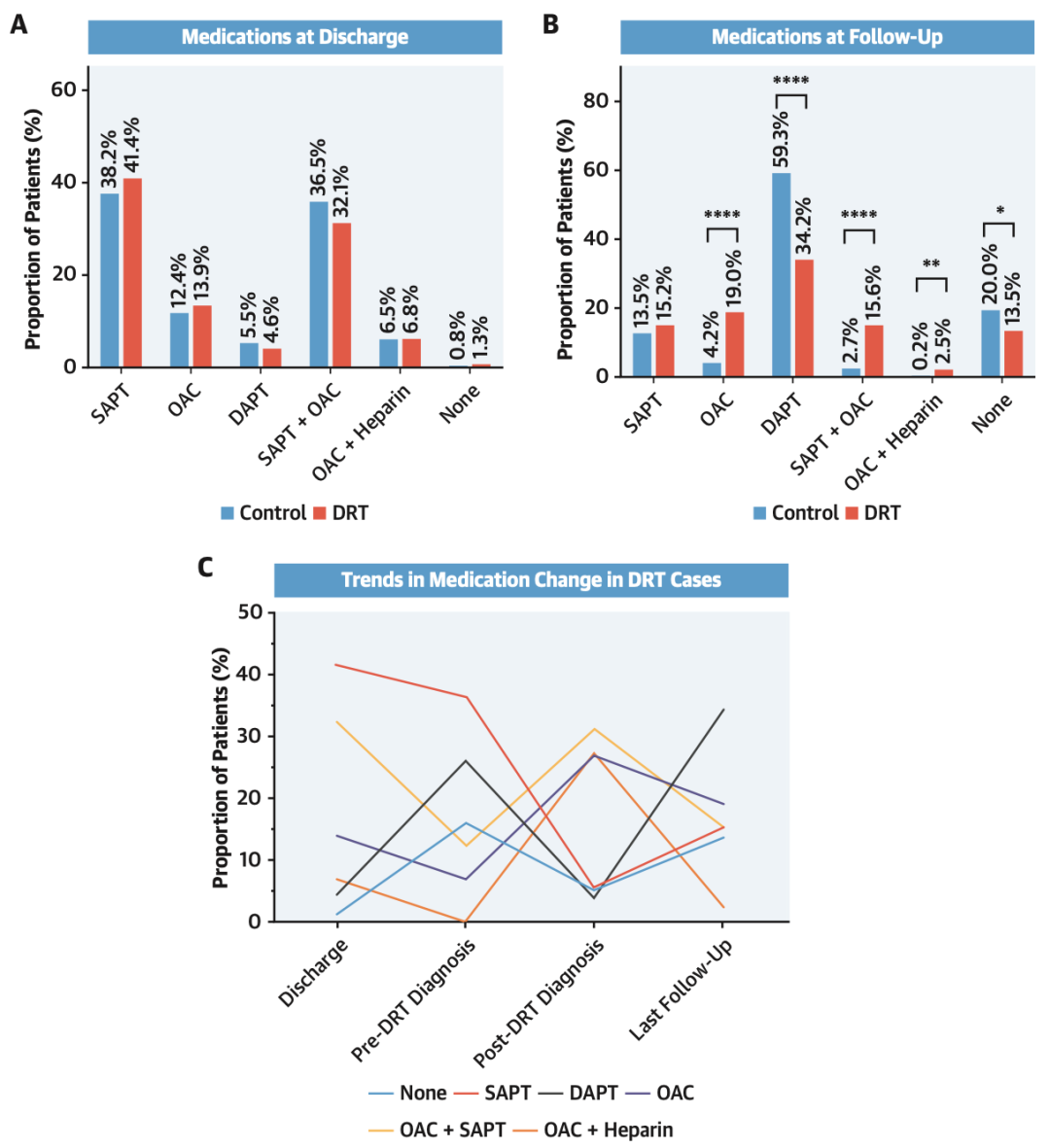
Figure 3: Antithrombotic drug usage at discharge after LAAO (A) and at the last follow-up (B), as well as the trend of antithrombotic drug changes in the DRT group (C).
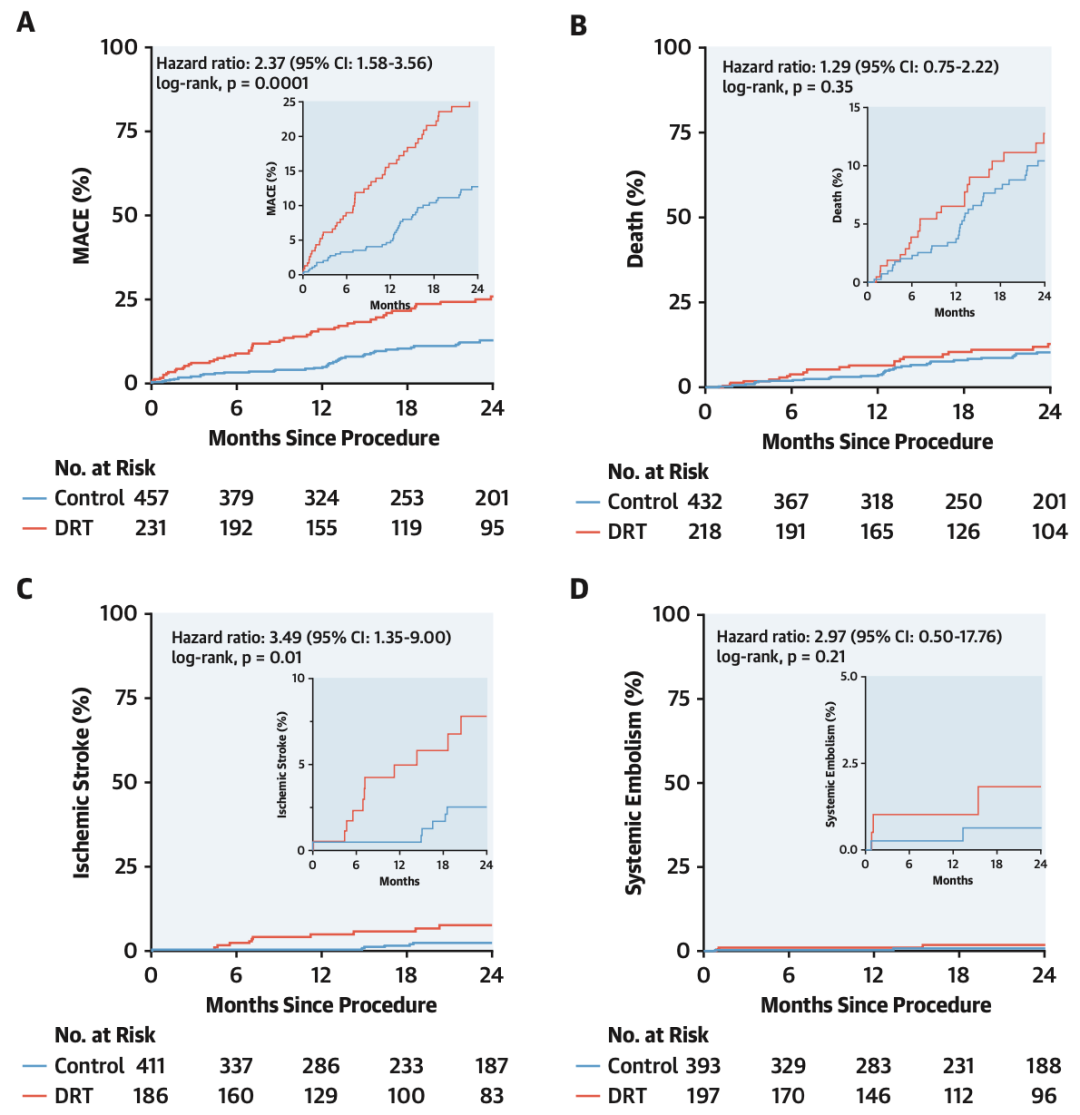
Figure 4: KM curves for MACE (A), death (B), ischemic stroke (C), and systemic embolism (D) incidence in the DRT group and control group after LAAO.
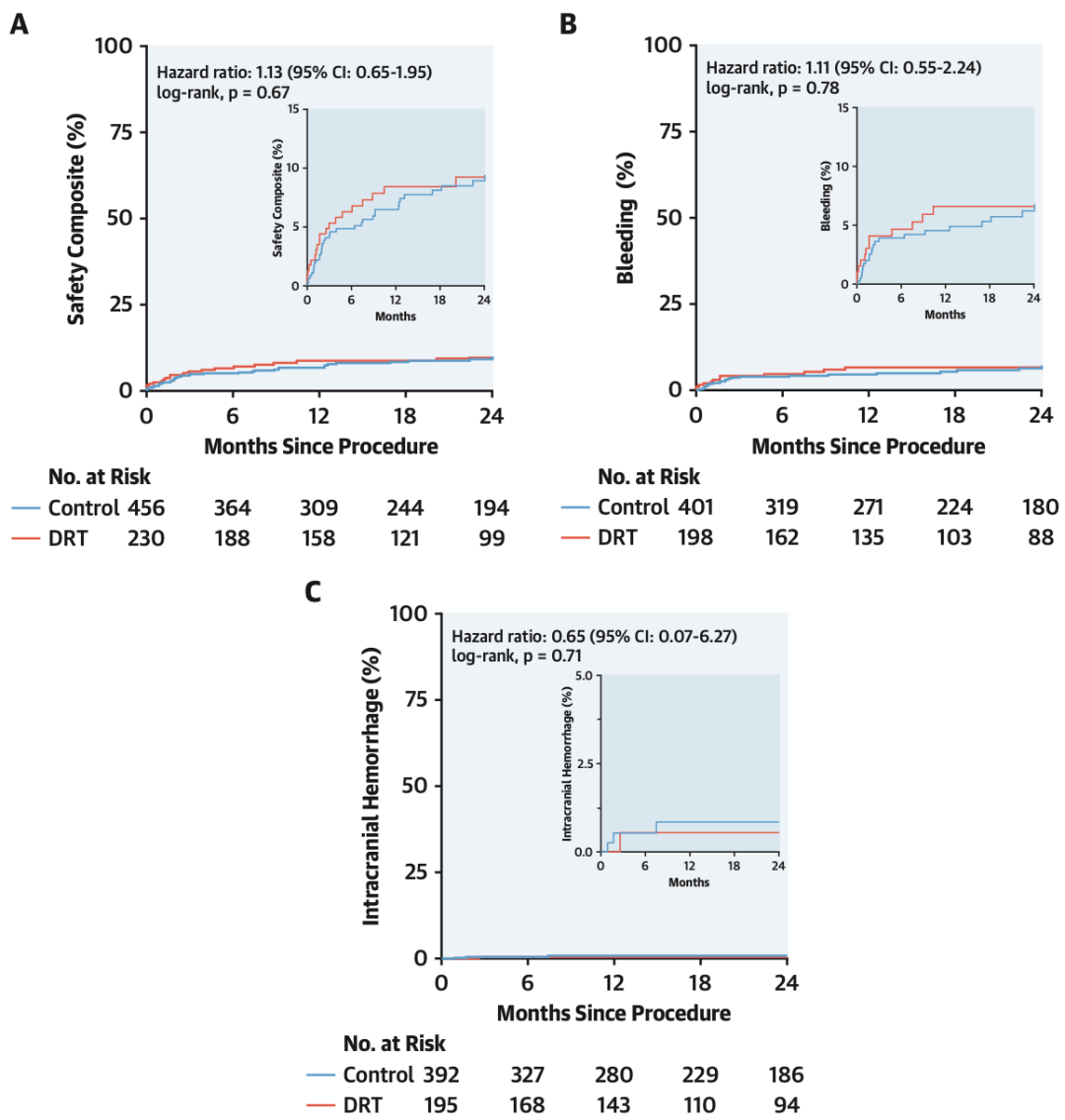
Figure 5: KM curves for safety endpoint events (A), bleeding events (B), and intracranial hemorrhage (C) incidence in the DRT group and control group after LAAO.
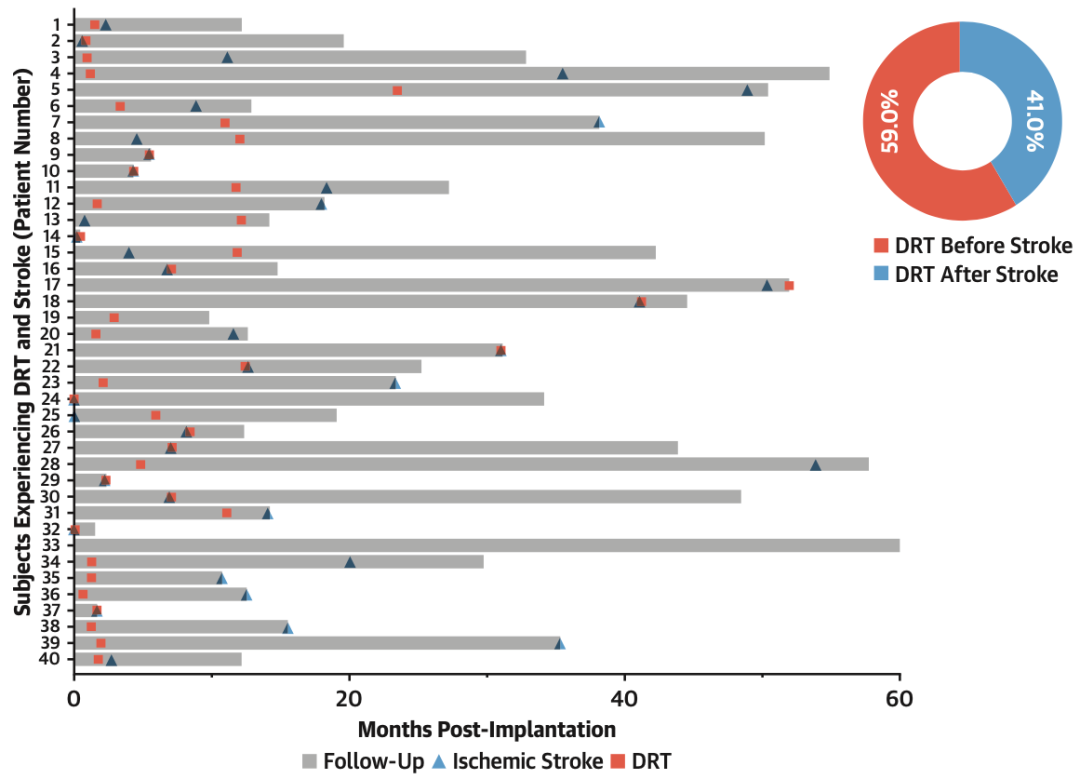
Figure 6: Distribution of DRT detection time and ischemic stroke occurrence time.
Multivariate analysis found that predictive factors for DRT included hypercoagulable state diseases (OR=17.50), pericardial effusion (OR=13.45), renal insufficiency (OR=4.02), occluder implantation distance greater than 10mm from the pulmonary veins (OR=2.41), and non-paroxysmal atrial fibrillation (OR=1.90) (Figure 7). After scoring these predictive factors, a DRT risk scoring system was established, where hypercoagulable state diseases and pericardial effusion each scored 4 points, renal insufficiency, occluder implantation distance greater than 10mm, and non-paroxysmal atrial fibrillation each scored 1 point, with total scores of 0-1 points indicating low risk for DRT and ≥2 points indicating high risk for DRT (Figure 8).
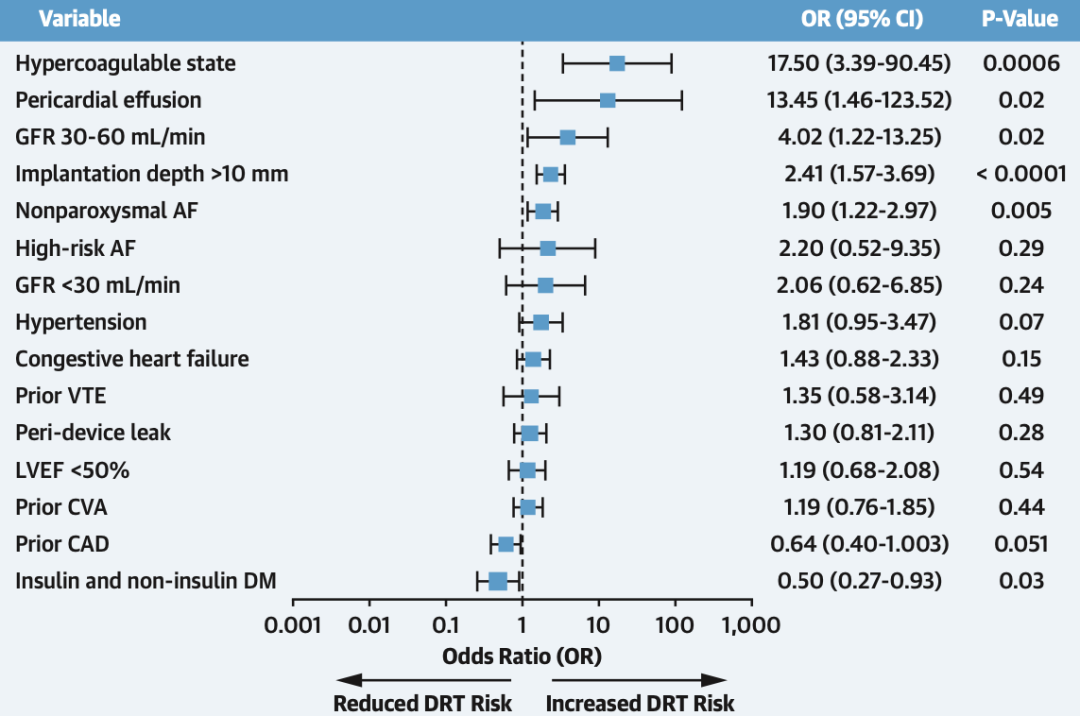
Figure 7: Predictive factors for DRT after LAAO.
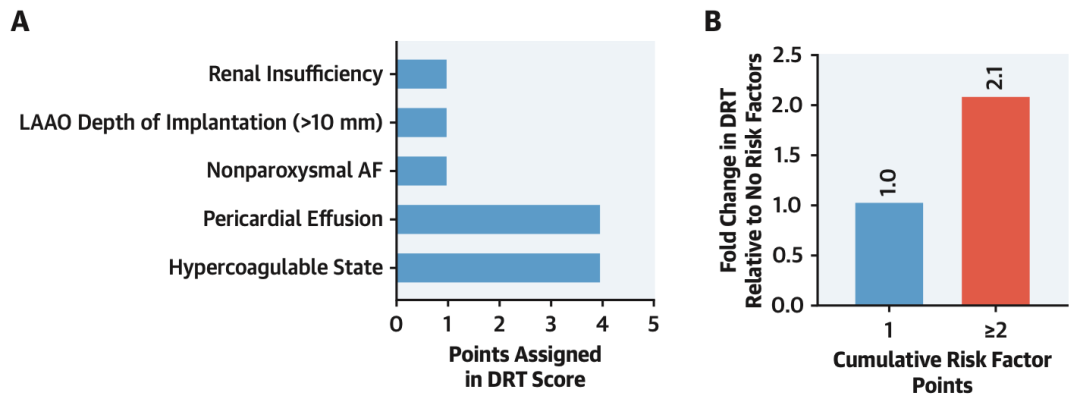
Figure 8: DRT risk scoring model.
Conclusion
This study shows that DRT after LAAO increases the risk of ischemic stroke. Some factors can predict DRT, and stratifying DRT risk based on these factors can facilitate perioperative and postoperative management.

References
PMID: 34294267
Editors | Reviewers: Du Xianfeng
Translation: Wang Binhao
Editor: Fang Renyuan
Previous Recommendations
High-risk patients with atrial fibrillation for stroke: The competition between LAAC and NOACs
What to do when LAAO encounters clopidogrel resistance?
Is it feasible to re-occlude residual leaks from the occluder?
Does the type of atrial fibrillation affect the results of left atrial appendage occlusion?
Does pulsed electric field ablation affect the histological characteristics and function of atrial tissue?
Are you willing to use 50W for isolating the superior vena cava?
What kind of “low-risk” atrial fibrillation patients are more likely to have a stroke?
What impact does thrombocytopenia have on left atrial appendage occlusion?
Relationship between the thickness of the epicardial fat pad of the left atrial posterior wall and recurrence after atrial fibrillation ablation
[EP Good Case] Right-sided accessory pathway seen by ICE
Can bivalirudin be used instead of heparin during left atrial appendage occlusion?
Is T-wave inversion in COVID-19 patients significant?
What impact does left atrial appendage occlusion have on AF progression? The FLAAC registry study

