Wearing a smartwatch on the wrist can detect arrhythmias such as bradycardia, tachycardia, and even atrial fibrillation. It can also simulate a single-lead ECG by connecting to a finger, enhancing diagnostic accuracy. Today, we will introduce how to use a smartwatch to simulate a multi-lead ECG for diagnosing more complex heart conditions like myocardial infarction and Brugada syndrome.
1. Simulating Leads I, II, III
Three-lead ECG from limbs
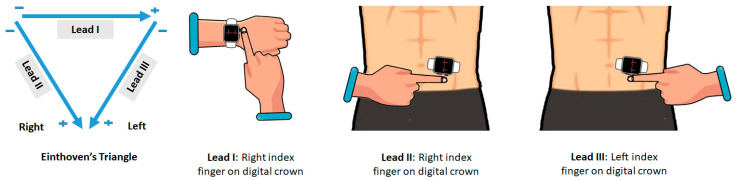
Figure 1. Diagram showing the placement of the smartwatch for simulation
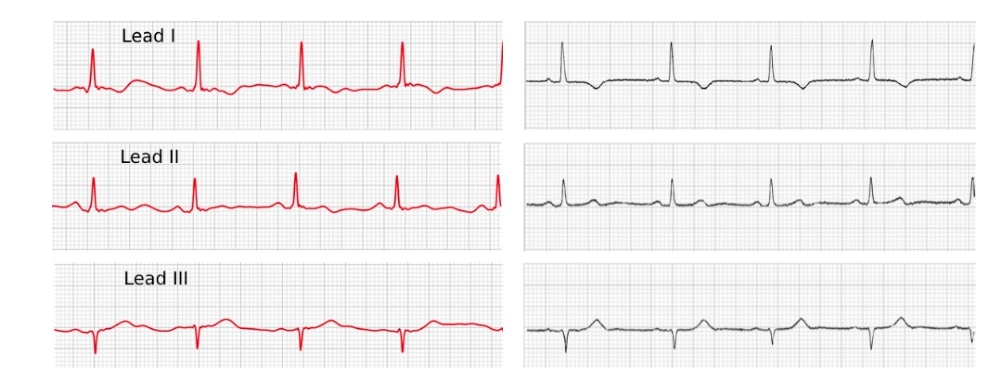
Figure 2. Comparison of standard ECG leads I, II, III with smartwatch simulated three-lead ECG
2. Simulating a Six-lead ECG
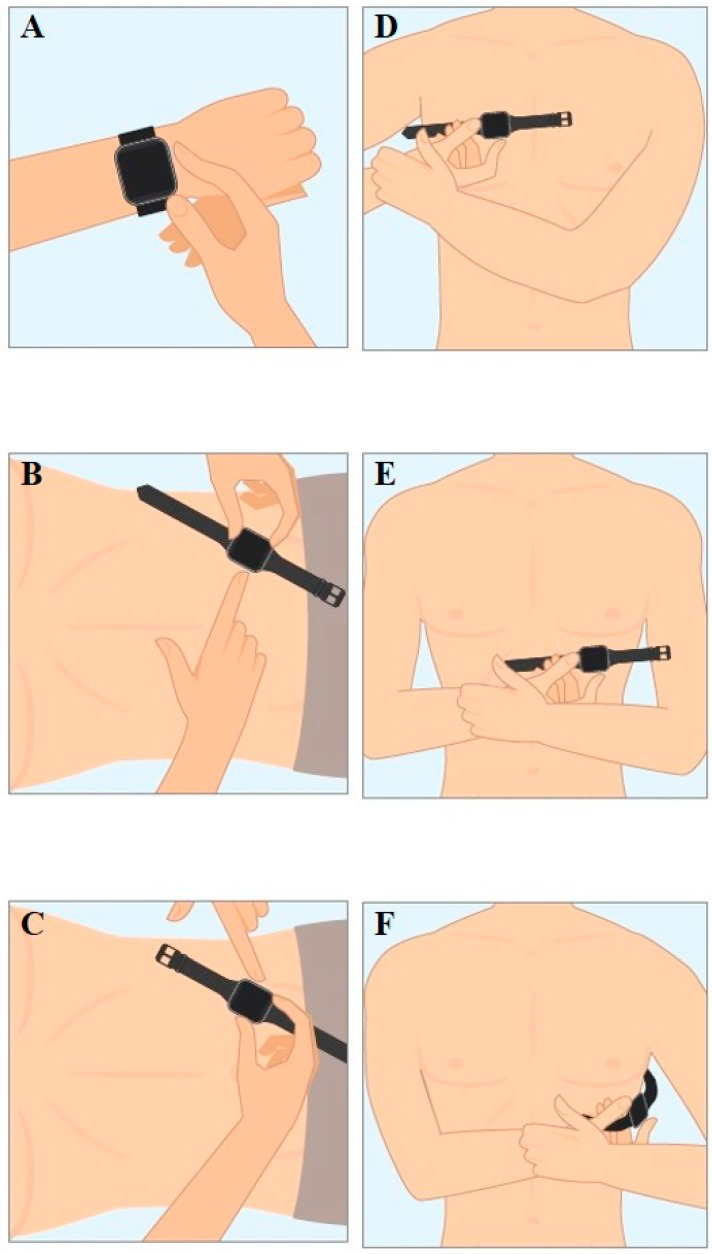
Figure 3. Diagram showing the placement of the smartwatch for six-lead simulation. The Einthoven (I, II, III) leads correspond to diagrams A, B, and C, while the Wilson pseudo-unipolar chest leads Wr (diagram D corresponding to V1), Wm (diagram E corresponding to V4), and Wl (diagram F corresponding to V6).

Figure 4. Comparison of standard ECG leads I, II, III, V1, V4, V6 with smartwatch simulated six-lead ECG
3. Simulating a Nine-lead ECG

Figure 5. The Apple Watch can obtain a nine-lead ECG as follows: the watch is worn on the left wrist, and the right index finger on the crown records lead I. To record other leads, the watch must be removed and placed correctly on appropriate abdominal and chest locations. The watch on the left lower abdomen and the right index finger on the crown records lead II, and the watch on the left lower abdomen and the left index finger on the crown records lead III. The leads correspond to V1 (right fourth intercostal space next to the sternum), V2 (left fourth intercostal space next to the sternum), V3 (between V2 and V4), V4 (left fifth intercostal space at the midclavicular line), V5 (left fifth intercostal space at the anterior axillary line), and V6 (left fifth intercostal space at the midaxillary line).
How accurate is this simulated multi-lead ECG? Let’s look at a controlled study published in JAMA Cardiology.
The study included 54 patients with ST-elevation myocardial infarction, 27 patients with non-ST-elevation myocardial infarction, and 19 healthy individuals. The watch was placed in different body positions to obtain nine bipolar ECGs (corresponding to Einthoven’s leads I, II, and III, and chest leads V1-V6), which were then compared with standard 12-lead ECG.
The Apple Watch and standard ECG were consistent in detecting normal ECG (Cohen’s kappa coefficient 0.90), ST segment elevation changes (Cohen’s kappa coefficient 0.88), and non-ST segment elevation changes (Cohen’s kappa coefficient 0.85). Bland-Altman analysis showed consistency between the Apple Watch and standard ECG in detecting the magnitude of ST segment changes (bias -0.003; SD, 0.18). The sensitivity of the Apple Watch in diagnosing normal ECG was 84%, specificity 100%; sensitivity for ST elevation was 93%, specificity 95%; sensitivity for NSTE was 94%, specificity 92%.
We can use the ECG recorded on the smartwatch to assist in the early diagnosis of acute coronary syndrome. Below is a simulated ECG detected by the smartwatch indicating a suspicious anterior myocardial infarction.
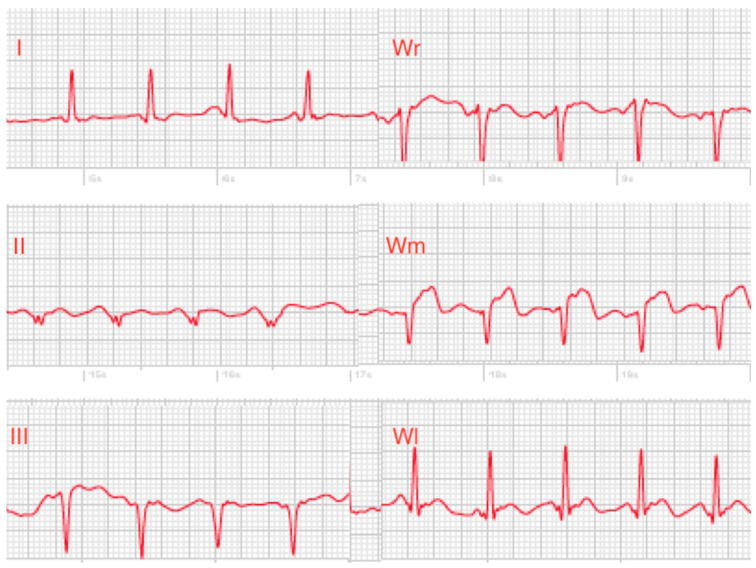
Figure 6. Simulated ECG Wm (V4) lead shows significant elevation, which can also screen for Brugada syndrome.
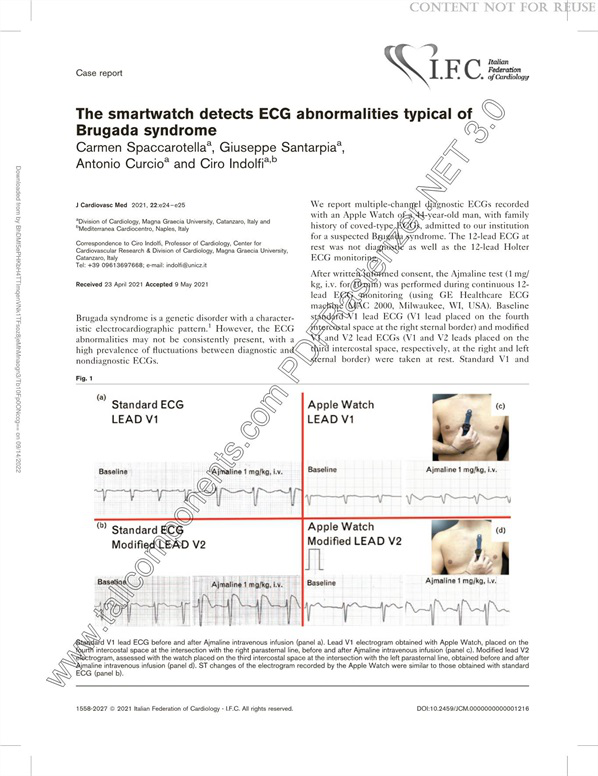
Figure 7. Simulated V1 and V2 leads indicate Brugada syndrome
Recently, someone developed a method using smartwatches to record lead I and modified lead V1 to detect whether heart resynchronization therapy (CRT) patients experience left ventricular (LV) non-capture path algorithms (Figure 8).
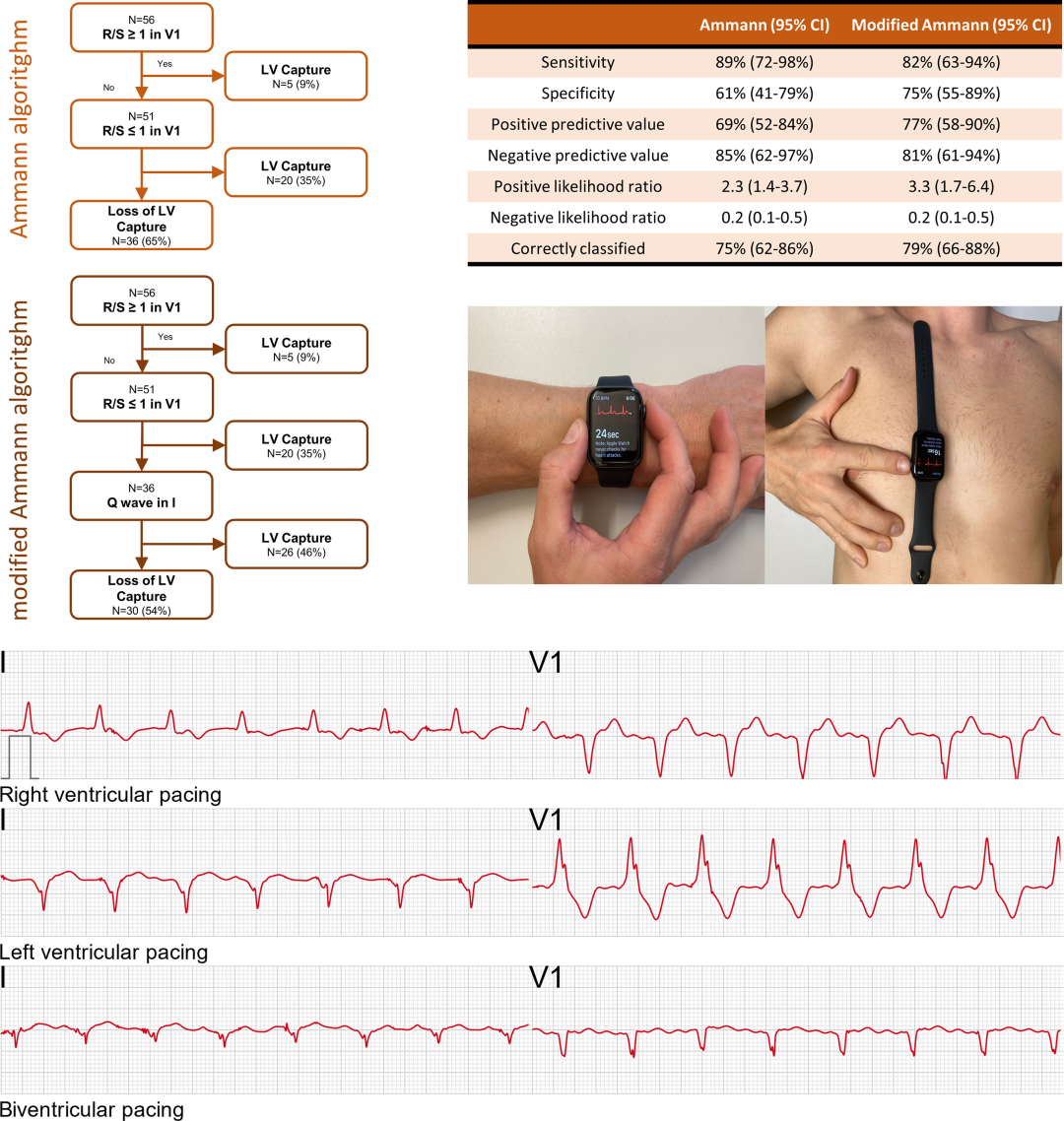
Figure 8. Flowchart for detecting CRT left ventricular non-capture using a smartwatch
If you have a smartwatch capable of recording ECG (the study used the Apple Watch), utilizing these simulation functions is equivalent to carrying a simple ECG machine.
References
1. https://www.heartrhythmjournal.com/article/S1547-5271(22)02382-7/fulltext
2. https://pubmed.ncbi.nlm.nih.gov/31658713
3. DOI: 10.1001/jamacardio.2020.3994
4. DOI: 10.2459/JCM.0000000000001216
5. https://pubmed.ncbi.nlm.nih.gov/32906661