Skip to content
Many people are confused about what the International Consensus Classification (ICC) of hematolymphoid tumors is. Today, we will briefly introduce it.
To introduce the origin of the ICC, it is inevitable to discuss the origin of the 5th edition of the World Health Organization (WHO) classification, and it is also necessary to review how past classifications of hematopoietic and lymphoid tumors were developed.
A Brief Review of the Changes in WHO Classification of Hematopoietic and Lymphoid Tumors (2022)
In previous communications, we mentioned that the WHO established the “Histological and Cytological Typing of Hematopoietic and Lymphoid Tumors” in 1976. This was the earliest version of the WHO classification (1st edition), but it was far less known than the French-American-British (FAB) classification and was hardly used.
Classification of Myeloid Tumors/Acute Leukemia: A Global Perspective and International Consensus Classification Approach
Since 2001, under the auspices of the WHO and its affiliated International Agency for Research on Cancer (IARC), the classification of hematopoietic and lymphoid tumors has been unified as part of the WHO classification series commonly referred to as the “WHO Blue Book”; this series also includes classifications for other tumors, such as those of the urinary and male reproductive systems, nervous system tumors, head and neck tumors, and thoracic tumors, among others.
For example, here is the Chinese translation of the 2001 WHO Classification of Nervous System Tumors (Blue Book):
 Before 2001, the classification of lymphomas, leukemias, and chronic myeloid diseases followed various different and often controversial paths. For lymphomas, pathologists initially adopted limited single-expert or regional classifications, such as those proposed by Rappaport, Lennert (Kiel), and Lukes and Collins; attempts were made to create a common language between classifications, termed a working classification, to establish their own classification. Although Rappaport included leukemias and chronic myeloid diseases in the 1966 Armed Forces Institute of Pathology volume, the recognized classifications of myeloid tumors and leukemias were primarily proposed by hematologists, including the FAB and polycythemia vera study group, among others. These classifications varied in standards and were based on different combinations of clinical features, cell morphology, and cytochemical tests; in some cases, limited immunophenotype analyses were included, with little assessment of prognostic significance. Despite these limitations, various classifications provided urgently needed standards for the diagnosis of various hematological tumors, which could be further studied and refined. However, these classifications did not represent an international consensus and did not widely incorporate the opinions of experts in hematology, oncology, genetics, and pathology.
In 1994, the International Lymphoma Study Group (ILSG), composed of international lymphoma pathologists, proposed the revised European-American Lymphoma (REAL) classification, attempting to define biological lymphoma entities based on clinical, morphological, immunophenotypic, and genetic criteria. After the publication of the REAL classification, Paul Kleihues and Les Sobin, co-editors of the WHO/IARC 3rd edition Blue Book series, contacted the co-authors of the REAL classification, including Elaine Jaffe, then president of the American Society of Hematopathology, to develop a similar classification for the WHO/IARC Blue Book series, which had not previously been widely used for hematological diseases classification.In fact, the 2nd edition of the WHO series did not include hematological tumors (from my understanding, the REAL classification could perhaps be seen as the 2nd edition WHO classification?).Jaffe and the executive committee of the American Society of Hematopathology suggested that the work for the 3rd edition of the WHO (now overseen by the IARC) be supervised by two major hematopathology societies, namely the American Society of Hematopathology (SH) and the European Association for Haematopathology (EAHP), convening an international advisory committee (CAC) of leading pathologists, oncologists, hematologists, and geneticists to provide input for the development of such classifications. They also suggested that the 3rd edition classification should not be limited to lymphomas but should also include myeloid tumors and acute leukemias.
The first CAC was held in 1997 at the Arlie House in Virginia, USA, and ultimately, with the efforts of 75 invited authors from around the world, the 3rd edition WHO classification of hematopoietic and lymphoid tumors was published in 2001.Similar CAC meetings were subsequently held in Chicago in 2007 and 2014, chaired by James Vardiman and Michelle Le Beau, and the 4th edition and revised 4th edition WHO/IARC publications were released in 2008 and 2017, respectively. The revised 4th edition had over 200 contributors from 24 countries. The records of the CAC meetings were published by the CAC leadership prior to the official WHO/IARC books.
Let’s discuss specifically:
The records of the CAC meeting for the 3rd edition were milestone documents, proposing several major changes that are now well-known, including: the establishment of a large category to include diseases that are essentially proliferative but also have developmental abnormalities (i.e., MDS/MPD, the predecessor of MDS/MPN); a diagnosis of acute myeloid leukemia (AML) can be made with a blast cell ratio of ≥20%; AML with specific cytogenetic/molecular genetic features should be classified as distinct entities; there is no need to retain FAB nomenclature for precursor lymphoblastic tumors (the morphology of L1 and L2 cannot suggest immunophenotype, genetic abnormalities, or clinical manifestations, while L3 is usually the leukemic phase of Burkitt lymphoma); acute lymphoblastic leukemia and precursor lymphoblastic lymphoma are different manifestations of the same disease; and so on.
The records of the revised 4th edition CAC meeting were published in the journal BLOOD in 2016, hence this version is referred to as WHO 2016 and WHO 2017, which, in my view, are synonymous.
Attached is an introduction to the 3rd edition WHO classification (2001):
As well as an introduction to the 4th edition WHO classification (2008):
Now we can introduce the International Consensus Classification (ICC) and the 5th edition WHO classification origins.
Overview of the 5th edition WHO Classification
Summary of ICC and 5th edition WHO Classification Comparison Interpretation
The 5th edition WHO did not continue the formation process of the past three versions, but adopted an entirely new approach. Here, I quote the WeChat public account “Integrated Diagnosis of Hematological Diseases” PPT:
Thus, the editors of the 5th edition WHO classification and the editors of the revised 4th edition WHO classification are entirely different. However, the international expert group (many of whom participated in the revision of the 4th edition WHO classification) did not recognize the approach taken by WHO/IARC:
Before 2001, the classification of lymphomas, leukemias, and chronic myeloid diseases followed various different and often controversial paths. For lymphomas, pathologists initially adopted limited single-expert or regional classifications, such as those proposed by Rappaport, Lennert (Kiel), and Lukes and Collins; attempts were made to create a common language between classifications, termed a working classification, to establish their own classification. Although Rappaport included leukemias and chronic myeloid diseases in the 1966 Armed Forces Institute of Pathology volume, the recognized classifications of myeloid tumors and leukemias were primarily proposed by hematologists, including the FAB and polycythemia vera study group, among others. These classifications varied in standards and were based on different combinations of clinical features, cell morphology, and cytochemical tests; in some cases, limited immunophenotype analyses were included, with little assessment of prognostic significance. Despite these limitations, various classifications provided urgently needed standards for the diagnosis of various hematological tumors, which could be further studied and refined. However, these classifications did not represent an international consensus and did not widely incorporate the opinions of experts in hematology, oncology, genetics, and pathology.
In 1994, the International Lymphoma Study Group (ILSG), composed of international lymphoma pathologists, proposed the revised European-American Lymphoma (REAL) classification, attempting to define biological lymphoma entities based on clinical, morphological, immunophenotypic, and genetic criteria. After the publication of the REAL classification, Paul Kleihues and Les Sobin, co-editors of the WHO/IARC 3rd edition Blue Book series, contacted the co-authors of the REAL classification, including Elaine Jaffe, then president of the American Society of Hematopathology, to develop a similar classification for the WHO/IARC Blue Book series, which had not previously been widely used for hematological diseases classification.In fact, the 2nd edition of the WHO series did not include hematological tumors (from my understanding, the REAL classification could perhaps be seen as the 2nd edition WHO classification?).Jaffe and the executive committee of the American Society of Hematopathology suggested that the work for the 3rd edition of the WHO (now overseen by the IARC) be supervised by two major hematopathology societies, namely the American Society of Hematopathology (SH) and the European Association for Haematopathology (EAHP), convening an international advisory committee (CAC) of leading pathologists, oncologists, hematologists, and geneticists to provide input for the development of such classifications. They also suggested that the 3rd edition classification should not be limited to lymphomas but should also include myeloid tumors and acute leukemias.
The first CAC was held in 1997 at the Arlie House in Virginia, USA, and ultimately, with the efforts of 75 invited authors from around the world, the 3rd edition WHO classification of hematopoietic and lymphoid tumors was published in 2001.Similar CAC meetings were subsequently held in Chicago in 2007 and 2014, chaired by James Vardiman and Michelle Le Beau, and the 4th edition and revised 4th edition WHO/IARC publications were released in 2008 and 2017, respectively. The revised 4th edition had over 200 contributors from 24 countries. The records of the CAC meetings were published by the CAC leadership prior to the official WHO/IARC books.
Let’s discuss specifically:
The records of the CAC meeting for the 3rd edition were milestone documents, proposing several major changes that are now well-known, including: the establishment of a large category to include diseases that are essentially proliferative but also have developmental abnormalities (i.e., MDS/MPD, the predecessor of MDS/MPN); a diagnosis of acute myeloid leukemia (AML) can be made with a blast cell ratio of ≥20%; AML with specific cytogenetic/molecular genetic features should be classified as distinct entities; there is no need to retain FAB nomenclature for precursor lymphoblastic tumors (the morphology of L1 and L2 cannot suggest immunophenotype, genetic abnormalities, or clinical manifestations, while L3 is usually the leukemic phase of Burkitt lymphoma); acute lymphoblastic leukemia and precursor lymphoblastic lymphoma are different manifestations of the same disease; and so on.
The records of the revised 4th edition CAC meeting were published in the journal BLOOD in 2016, hence this version is referred to as WHO 2016 and WHO 2017, which, in my view, are synonymous.
Attached is an introduction to the 3rd edition WHO classification (2001):
As well as an introduction to the 4th edition WHO classification (2008):
Now we can introduce the International Consensus Classification (ICC) and the 5th edition WHO classification origins.
Overview of the 5th edition WHO Classification
Summary of ICC and 5th edition WHO Classification Comparison Interpretation
The 5th edition WHO did not continue the formation process of the past three versions, but adopted an entirely new approach. Here, I quote the WeChat public account “Integrated Diagnosis of Hematological Diseases” PPT:
Thus, the editors of the 5th edition WHO classification and the editors of the revised 4th edition WHO classification are entirely different. However, the international expert group (many of whom participated in the revision of the 4th edition WHO classification) did not recognize the approach taken by WHO/IARC:
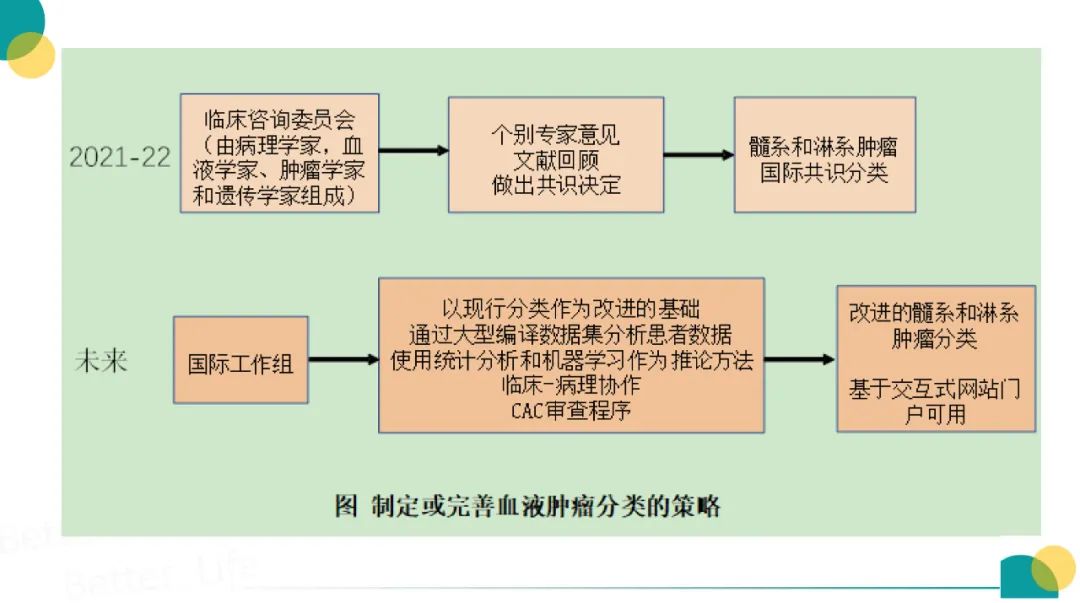 Despite multiple communications between the leaders of SH and EAHP and Ian Cree, the editor of the WHO/IARC 5th edition Blue Book series, including a formal request from 33 leaders in pathology, hematology, oncology, and genetics in February 2020, consensus was not reached on the necessity of convening a Clinical Advisory Committee (CAC) before initiating the 5th edition classification. Therefore, even though they knew that their conclusions might not inform the forthcoming WHO classification, SH and EAHP decided to advance the CAC, based on the opinions of former WHO editors and senior advisors, as well as leaders from SH and EAHP and top clinicians from around the world. To organize the International Consensus Meeting on Myeloid and Lymphoid Tumor Classification (ICC), clinical and pathology co-chairs for lymphoid and myeloid/acute leukemia were selected. The co-chairs for myeloid/acute leukemia pathology, Daniel Arber, Robert Hasserjian, and Attilio Orazi, along with clinical co-chairs Mario Cazzola, Hartmut Döhner, and Ayalew Tefferi, aimed to include diverse and geographically broad leaders in various disease categories. Once participants were identified, extensive preparatory work was needed to prepare for a two-day productive CAC meeting. Invited participants were assigned to groups, each of which pre-reviewed existing classifications and proposed potential changes and key issues to be addressed at the CAC. Each group held a series of virtual meetings and shared key issues across disease groups, such as potential changes in blast cell counts or exclusion criteria.
On September 20-21, groups gathered at the Rubinstain Forum on the University of Chicago campus to present their statements to the entire CAC. The combined CAC for lymphoid and myeloid/acute leukemia included 138 participants from 23 countries across 5 continents (42 onsite, 98 remote). Participants discussed and debated potential classification changes and identified new and unresolved issues. After the meeting, the groups reconvened to address key issues and propose the final classifications for myeloid tumors and acute leukemias. For several contentious issues, a survey was conducted among all CAC myeloid/acute leukemia participants to gather further opinions and ensure consensus on significant changes. The results became the International Consensus Classification for Myeloid and Lymphoid Neoplasms (ICC-MLN), which will be reported in a peer-reviewed manuscript, with a publication target of mid-2022 (ultimately published in September of that year in the journal BLOOD, while the introductory literature for the 5th edition WHO classification was published earlier in May in the journal Leukemia). The new name ICC-MLN was proposed by the pathology co-chairs, reflecting broad international input from authoritative pathologists and clinicians, as well as updated genetic integration. ICC-MLN will reflect the consensus among all parties involved in the diagnosis and treatment of hematological tumor patients regarding disease entities, terminology, and diagnostic criteria.
The fundamental principle of the new ICC classification is to rely on input from pathology experts and clinical insights to develop a classification that is reasonable in terms of genetic integration and clinical pathology.
Thus, in terms of lineage, the ICC is the legitimate continuation of the revised 4th edition WHO classification (continuing the formation process of the past three versions of the WHO classification), while the 5th edition WHO classification is a new endeavor (borrowing from ICC’s perspective: there is almost no continuity). However, which of the two is better, I clearly cannot say.
It is worth mentioning that the ICC classification has been adopted in the adult acute myeloid leukemia (AML) treatment recommendations of the European Leukemia Network, and these recommendations were published months before the ICC CAC meeting records were published in BLOOD.
However, nearly two years later (from May 2022 to now), the 5th edition WHO Blue Book has still not been published. The information I have received is that WHO/IARC and SH/EAHP are still at odds on many issues, trying to reach a consensus. This somewhat surprises me; I thought WHO/IARC would be confident in establishing a new classification on their own, but it seems that things are not so smooth, and they are likely under significant pressure from various sides; otherwise, it should have been published long ago. It is said that ICC will also have its own publication (similar to the existence of the WHO Blue Book), and for now, we can only continue to wait.
As for how to deal with the existence of two classification systems, please refer to the following hyperlinks:
Summary of ICC and 5th edition WHO Classification Comparison Interpretation
How will China move forward in the era of dual international classifications?
It must be emphasized that neither the ICC nor the 5th edition WHO classification, nor past versions, seem to have had experts from mainland China involved in their writing (there are some from Hong Kong SAR and Taiwan). However, the population of mainland China exceeds the combined population of Western countries; coupled with various influencing factors such as ethnicity, living environment, and lifestyle, the situation of many diseases in China differs from the discussions in the revised 4th edition WHO classification Blue Book. Therefore, I believe that regardless of which new classification is adopted, we should cautiously regard the discussions in their publications.
Despite multiple communications between the leaders of SH and EAHP and Ian Cree, the editor of the WHO/IARC 5th edition Blue Book series, including a formal request from 33 leaders in pathology, hematology, oncology, and genetics in February 2020, consensus was not reached on the necessity of convening a Clinical Advisory Committee (CAC) before initiating the 5th edition classification. Therefore, even though they knew that their conclusions might not inform the forthcoming WHO classification, SH and EAHP decided to advance the CAC, based on the opinions of former WHO editors and senior advisors, as well as leaders from SH and EAHP and top clinicians from around the world. To organize the International Consensus Meeting on Myeloid and Lymphoid Tumor Classification (ICC), clinical and pathology co-chairs for lymphoid and myeloid/acute leukemia were selected. The co-chairs for myeloid/acute leukemia pathology, Daniel Arber, Robert Hasserjian, and Attilio Orazi, along with clinical co-chairs Mario Cazzola, Hartmut Döhner, and Ayalew Tefferi, aimed to include diverse and geographically broad leaders in various disease categories. Once participants were identified, extensive preparatory work was needed to prepare for a two-day productive CAC meeting. Invited participants were assigned to groups, each of which pre-reviewed existing classifications and proposed potential changes and key issues to be addressed at the CAC. Each group held a series of virtual meetings and shared key issues across disease groups, such as potential changes in blast cell counts or exclusion criteria.
On September 20-21, groups gathered at the Rubinstain Forum on the University of Chicago campus to present their statements to the entire CAC. The combined CAC for lymphoid and myeloid/acute leukemia included 138 participants from 23 countries across 5 continents (42 onsite, 98 remote). Participants discussed and debated potential classification changes and identified new and unresolved issues. After the meeting, the groups reconvened to address key issues and propose the final classifications for myeloid tumors and acute leukemias. For several contentious issues, a survey was conducted among all CAC myeloid/acute leukemia participants to gather further opinions and ensure consensus on significant changes. The results became the International Consensus Classification for Myeloid and Lymphoid Neoplasms (ICC-MLN), which will be reported in a peer-reviewed manuscript, with a publication target of mid-2022 (ultimately published in September of that year in the journal BLOOD, while the introductory literature for the 5th edition WHO classification was published earlier in May in the journal Leukemia). The new name ICC-MLN was proposed by the pathology co-chairs, reflecting broad international input from authoritative pathologists and clinicians, as well as updated genetic integration. ICC-MLN will reflect the consensus among all parties involved in the diagnosis and treatment of hematological tumor patients regarding disease entities, terminology, and diagnostic criteria.
The fundamental principle of the new ICC classification is to rely on input from pathology experts and clinical insights to develop a classification that is reasonable in terms of genetic integration and clinical pathology.
Thus, in terms of lineage, the ICC is the legitimate continuation of the revised 4th edition WHO classification (continuing the formation process of the past three versions of the WHO classification), while the 5th edition WHO classification is a new endeavor (borrowing from ICC’s perspective: there is almost no continuity). However, which of the two is better, I clearly cannot say.
It is worth mentioning that the ICC classification has been adopted in the adult acute myeloid leukemia (AML) treatment recommendations of the European Leukemia Network, and these recommendations were published months before the ICC CAC meeting records were published in BLOOD.
However, nearly two years later (from May 2022 to now), the 5th edition WHO Blue Book has still not been published. The information I have received is that WHO/IARC and SH/EAHP are still at odds on many issues, trying to reach a consensus. This somewhat surprises me; I thought WHO/IARC would be confident in establishing a new classification on their own, but it seems that things are not so smooth, and they are likely under significant pressure from various sides; otherwise, it should have been published long ago. It is said that ICC will also have its own publication (similar to the existence of the WHO Blue Book), and for now, we can only continue to wait.
As for how to deal with the existence of two classification systems, please refer to the following hyperlinks:
Summary of ICC and 5th edition WHO Classification Comparison Interpretation
How will China move forward in the era of dual international classifications?
It must be emphasized that neither the ICC nor the 5th edition WHO classification, nor past versions, seem to have had experts from mainland China involved in their writing (there are some from Hong Kong SAR and Taiwan). However, the population of mainland China exceeds the combined population of Western countries; coupled with various influencing factors such as ethnicity, living environment, and lifestyle, the situation of many diseases in China differs from the discussions in the revised 4th edition WHO classification Blue Book. Therefore, I believe that regardless of which new classification is adopted, we should cautiously regard the discussions in their publications.