C-Reactive Protein
CRP has both pro-inflammatory and anti-inflammatory properties. It plays a role in recognizing and clearing foreign pathogens and damaged cells by binding to phosphocholine, phospholipids, histones, chromatin, and fibrinogen. It can activate the classical complement pathway and also activate phagocytes through Fc receptors, accelerating the clearance of cell debris and damaged or apoptotic cells and foreign pathogens.
High-sensitivity C-reactive protein (hs-CRP) is the same protein as ordinary CRP, but it is named due to the use of more sensitive detection methods such as latex immunoassay. The detection of hs-CRP allows for more accurate measurement of CRP in the range of 0.5-10mg/L, thus generating more clinical value.
Clinical Significance
-
In bacterial infections, serum CRP can be moderately to significantly elevated, with 80% of bacterial infection patients having CRP > 100 mg/L. -
Gram-negative infections can lead to the highest levels of CRP, sometimes reaching 500mg/L; -
Gram-positive bacterial infections and parasitic infections usually cause moderate reactions, typically around 100mg/L. -
CRP does not significantly increase in viral infections (except for some severe invasive viruses that cause tissue damage, such as adenovirus and herpes virus), usually not exceeding 50mg/L and rarely exceeding 100mg/L. -
During anti-infection treatment, dynamic monitoring of CRP levels can assist in assessing treatment efficacy. A decline in CRP to normal can be one of the indicators for discontinuing medication. -
The guidelines established by the British Thoracic Society recommend monitoring CRP levels as a useful indicator for evaluating the success of treatment for community-acquired pneumonia (CAP). A CRP ≤ 100mg/L has a similar negative predictive effect as the CURB-65 and Pneumonia Severity Index (PSI) classifications, suggesting that invasive respiratory support and/or vasopressor use are unnecessary. For suspected pneumonia, CRP is considered the first-line screening method, with a CRP greater than approximately 60mg/L indicating bacterial pneumonia.
-
Numerous studies indicate that inflammation plays a key role in the development of atherosclerosis and related cardiovascular events. As a sensitive indicator of inflammation, elevated hs-CRP levels are directly associated with the occurrence of atherosclerosis and the risk of plaque rupture. -
Individuals with elevated hs-CRP levels are twice as likely to experience acute strokes and three times more likely to suffer myocardial infarction compared to healthy individuals. Regular hs-CRP tests can help detect potential cardiovascular disease risks early. -
Most patients with acute myocardial infarction show significantly elevated CRP levels, and among all acute phase proteins, this increase appears the earliest.
-
When treating bacterial infections with antibiotics, dynamic monitoring of CRP is necessary, as it provides earlier warnings of complications and treatment efficacy than clinical signs, and is more clinically significant in cases of neutropenia or suppressed immune status. -
Serial plasma CRP measurements can be used for treatment monitoring in various infections, determining the effective use of antibiotic therapy; adjusting anti-inflammatory medication dosages based on changes in CRP levels; discontinuing antibiotic treatment when CRP returns to normal; and providing guidance for antibiotic treatment in high-risk populations lacking microbiological diagnoses.
-
-
CRP can be used to monitor the activity level and treatment efficacy of inflammatory diseases. In inflammatory joint diseases such as rheumatoid arthritis and ankylosing spondylitis, CRP levels can reflect disease activity.
-
CRP is used to assess the severity of acute pancreatitis. When CRP exceeds 250mg/L, it suggests extensive necrotizing pancreatitis.
-
Combined detection of CRP and white blood cells (WBC) has a synergistic diagnostic effect for bacterial infections. CRP is more sensitive than WBC, rising earlier and returning to normal more quickly, thus demonstrating extremely high sensitivity.
-
Elevated levels of CRP may be associated with an increased risk of postoperative complications, and CRP can serve as one of the predictive indicators for postoperative complications. -
If CRP increases within 6 hours post-surgery, it should decrease to normal within two to three days if there are no complications. If CRP remains elevated for 5 to 7 days post-surgery, it may indicate potential complications such as infection or thromboembolism. -
Measuring CRP also helps in estimating prognosis for burn patients and determining the timing for debridement and skin grafting.
6. Assessment of Disease Activity and Efficacy Monitoring
-
CRP levels of 10-50mg/L indicate mild inflammation; -
CRP rising to 100mg/L indicates a more severe disease, and intravenous administration may be necessary; -
CRP >100mg/L indicates severe disease processes and often indicates the presence of bacterial infection.
-
Within 3 days post-organ transplant, CRP levels rise and then begin to decrease; if the concentration does not decrease, it suggests early rejection reactions. -
In patients post-organ transplant, CRP also significantly rises during rejection, making it a useful indicator to assist in the clinical diagnosis of rejection reactions.
-
CRP may be elevated in patients with malignant tumors, thus it is also used as one of the monitoring indicators for tumors. CRP is a protein produced in response to inflammation and tissue damage in the human body. -
Elevated or rising CRP levels indicate poor prognosis and often suggest metastasis.
-
In systemic lupus erythematosus, polymyositis, and systemic sclerosis, CRP does not show significant changes, hence it can be used for the differentiation of rheumatic diseases. -
Patients with SLE are prone to secondary infections. Clinical manifestations are similar to those during active phases, and serum CRP does not show significant changes during active phases, but it rises significantly during secondary infections, making it important for differential diagnosis.
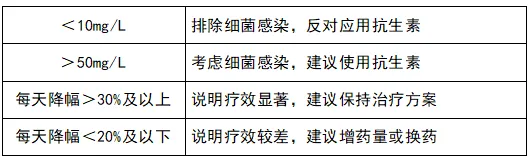
C-Reactive Protein Reference Values
Compiled/Formatted by: Joann
Edited by: Ye Jing