In critically ill adult patients, adverse stress states negatively impact treatment outcomes; thus, effective sedation and analgesia are beneficial for patient prognosis. This article introduces the initiation, maintenance, and discontinuation of sedation and analgesia.
Identifying the Causes of Stress
●Anxiety – Anxiety is defined as a response to real or perceived threats, resulting in a state of fear and persistent autonomic arousal.
●Pain – Routine patient management, immobilization, surgery, endotracheal intubation, and other monitoring devices can cause pain..
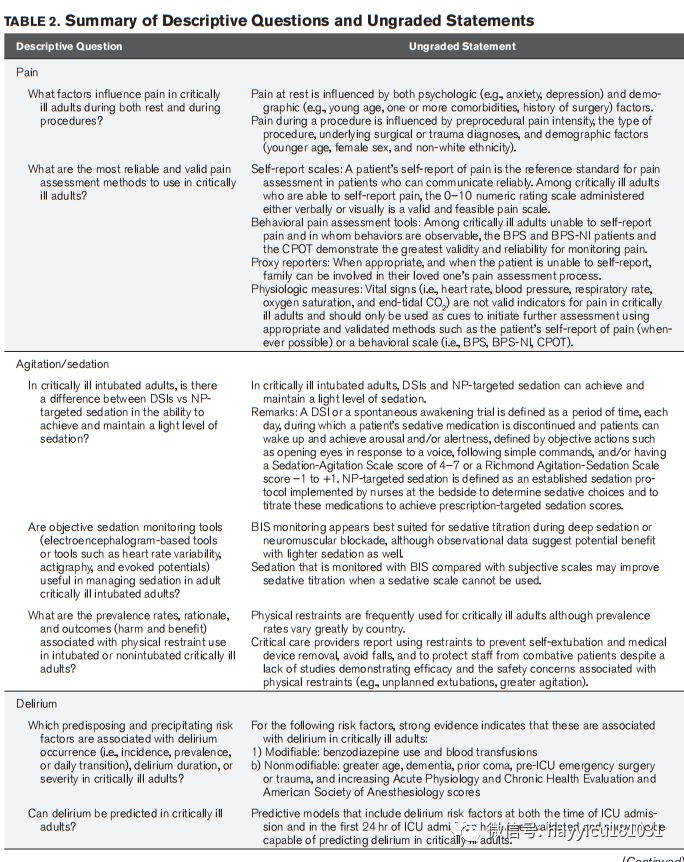
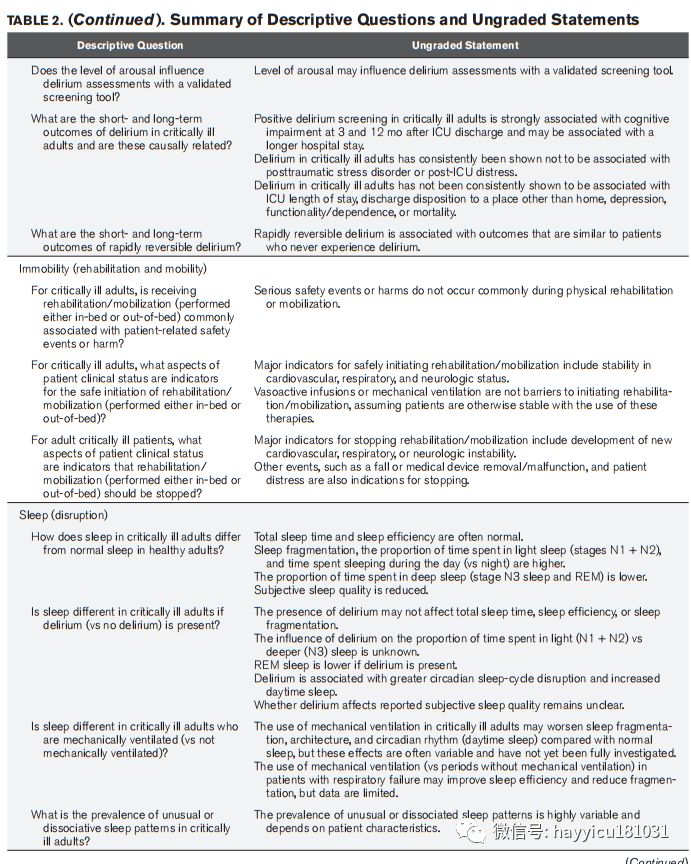
●Delirium – Delirium is an organic mental syndrome defined as an acute and potentially reversible impairment of consciousness and cognitive function, with an incidence in ICU patients as high as 80%, often unrecognized in older patients and those with hypoactive delirium.
Risk factors for delirium include: electrolyte imbalances (hypocalcemia and hyponatremia), hyperamylasemia, hyperglycemia, azotemia, liver disease (hyperbilirubinemia and elevated liver enzymes), infections, drug withdrawal, alcohol withdrawal, malnutrition, cancer, cerebrovascular disease, cardiopulmonary disease, advanced age, and certain medications (benzodiazepines, corticosteroids, antihistamines, β blockers, antiarrhythmics, digoxin.
●Dyspnea – Dyspnea is a sensation of air hunger or suffocation.
●Neuromuscular paralysis – All patients receiving neuromuscular blockade require sedation, as the absence of sedation or adequate analgesia during neuromuscular paralysis is an extremely frightening and uncomfortable experience for patients.
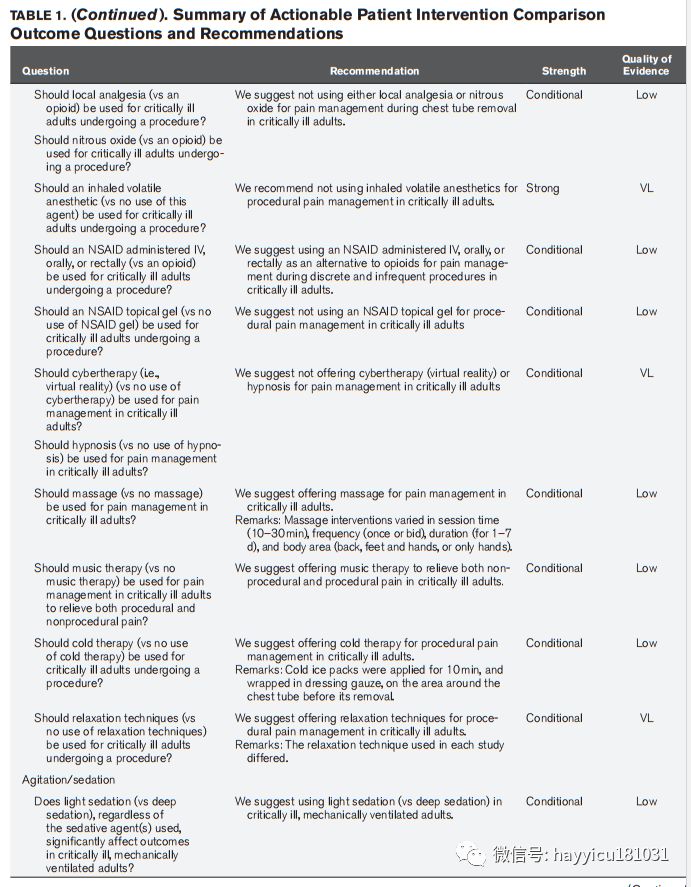
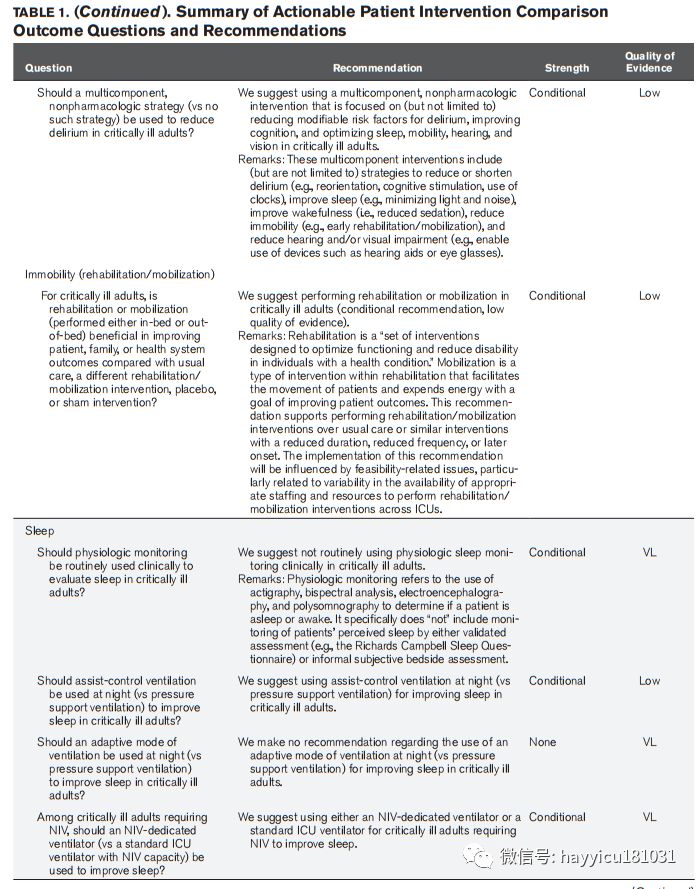
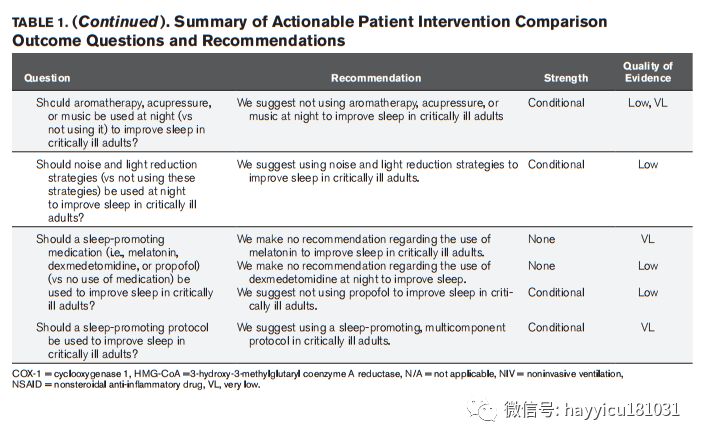
Non-Pharmacological Treatment Strategies — Pharmacological treatment strategies include: comforting patients, frequent communication with patients, regular family visits, establishing normal sleep cycles, and cognitive behavioral therapy. Examples of cognitive behavioral therapy include music therapy, guided imagery, and relaxation techniques.
●A multicenter randomized trial involving 373 mechanically ventilated patients reported that compared to usual care (UC) or noise-canceling headphones, patient-directed self-initiated music led to a decrease in anxiety visual analog scores throughout the study (up to 5.7 days) (52 points vs 33 points). Additionally, by day 5, the sedation intensity in the PDM group (sedation intensity score: 4.4 points vs 2.8 points) and frequency (the number of sedatives allowed in the study, 5 doses vs 3 doses) both decreased. A meta-analysis including 14 studies on the effects of music on mechanically ventilated patients confirmed these findings.
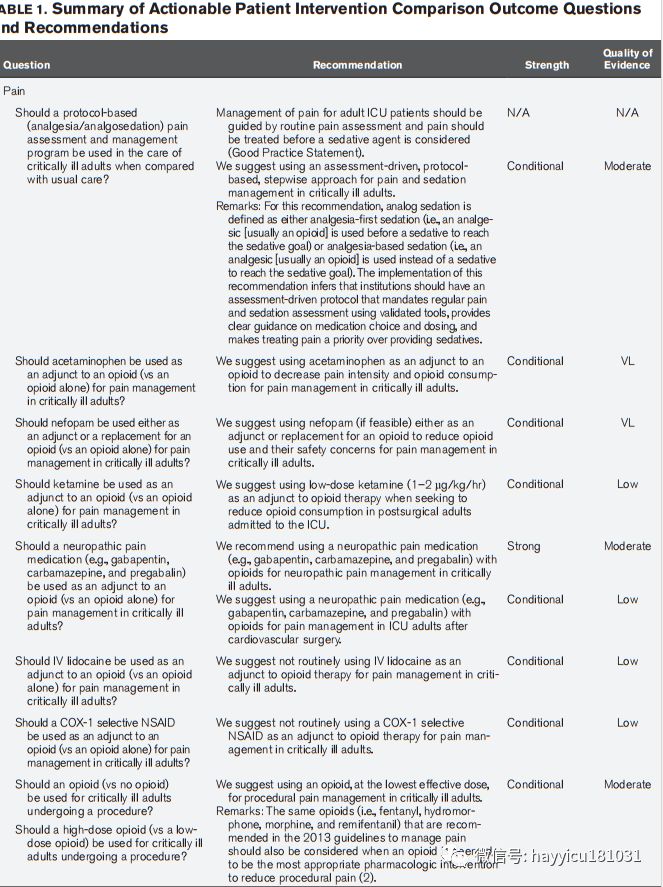
Initiation — The Society of Critical Care Medicine (SCCM) has published guidelines on the selection and initiation of sedation–analgesia medications for critically ill patients.
Available Medications — Commonly used sedation–analgesia medications in the ICU include: benzodiazepines (e.g., diazepam, lorazepam, and midazolam), opioids (e.g., fentanyl, hydromorphone, morphine, and remifentanil), propofol, dexmedetomidine, ketamine, and antipsychotics (e.g., haloperidol, quetiapine, and ziprasidone). Other medications such as acetaminophen, non-steroidal anti-inflammatory drugs (e.g., ketorolac), and anticonvulsants may be used as adjunctive therapy when needed.
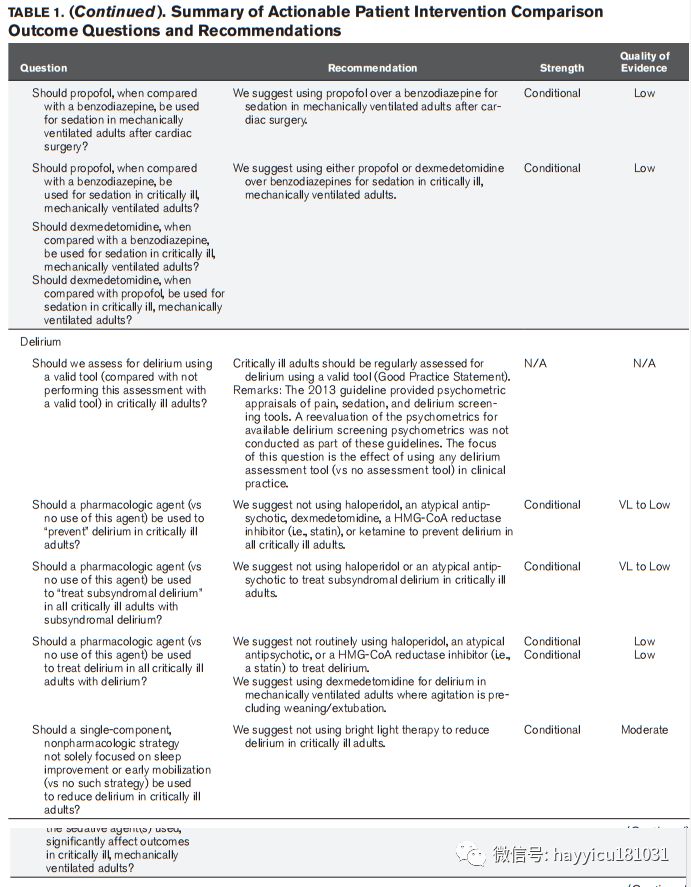
Medication Selection — The SCCM guidelines favor non-benzodiazepine medications, as evidence suggests they shorten the duration of mechanical ventilation, but the best medication for short-term or long-term treatment remains unclear.
●Addressing the Causes of Stress
•If the stress response is due to dyspnea or pain, opioids are the first choice.
•If the stress is due to delirium, antipsychotics (e.g., haloperidol, quetiapine) should not be routinely used but may be used for significant stress caused by delirium. Dexmedetomidine may be used for patients delayed in extubation due to delirium.
• The SCCM recommends using propofol instead of benzodiazepines for cardiac surgery patients, and using dexmedetomidine instead of benzodiazepines for other surgical and medical patients. For patients with unexplained stress who are intubated and mechanically ventilated, analgesia should be prioritized.
●Whenever selecting sedation–analgesia medications, the pharmacokinetic variables affecting drug metabolism (e.g., age, weight, and liver and kidney function) and the desired depth of sedation should also be considered.
Initial Dosing The initial dose of sedation–analgesia medications should be determined by the following factors: the expected level of sedation; the ability to tolerate the selected medication, including hemodynamic and respiratory status; and factors that may affect drug metabolism, such as patient age, weight, liver and kidney function, drug interactions, history of alcohol use, and substance abuse.
Administration — Evidence suggests that continuous infusion of sedation–analgesia medications may prolong the duration of mechanical ventilation. Intermittent intravenous boluses, daily awakenings, or minimal continuous infusion adjusted gradually to achieve a lighter sedation level with a RASS score of -2 to 0 should be considered. Initial intermittent intravenous boluses should be given, along with initial continuous infusion and daily awakenings or minimal doses adjusted gradually to achieve light sedation (RASS score -2 to 0).
Sedation Goals — The ideal sedation goal is for the patient to be awake, comfortable, and experiencing no or only mild stress (RASS scale 0).
Monitoring
●Pain scales – Existing unidimensional scoring methods (i.e., verbal numeric rating scale, visual analog scale, and numeric rating scale) and multidimensional scales (i.e., McGill Pain Questionnaire and Wisconsin Brief Pain Questionnaire) are used to assess the patient’s pain level.
●Sedation scales – Current guidelines support the use of RASS and the Richmond Agitation-Sedation Scale (SAS). Other scoring systems include: the Muscle Activity Assessment Scale (MAAS), the Minnesota Sedation Assessment Tool (MSAT), and the Ramsay Sedation Scale. The COMFORT scale is an effective and reliable scoring system for children.
●Delirium scales – i.e., the ICU Confusion Assessment Method (CAM-ICU). The Intensive Care Delirium Screening Checklist (ICDSC) is also a simple and effective tool for bedside assessment of delirium.
The Bispectral Index (BIS) — BIS monitoring analyzes electroencephalogram data using Fourier transform to estimate the depth of sedation. BIS monitoring is suitable for ICU patients receiving deep sedation or neuromuscular paralysis to assess sedation depth;
Avoiding Over-Sedation :
Intermittent Infusion — An observational study of 242 patients compared the duration of mechanical ventilation between two groups: one group received continuous infusion of sedation–analgesia medications, while the other group received intermittent infusion of sedation–analgesia medications based on a nursing protocol or no sedation–analgesia medications. The duration of mechanical ventilation in the intermittent infusion or no medication group was shorter than in the continuous infusion group (median time: 56 hours vs 185 hours).
Daily Awakening Sedation Strategy and Protocolized Sedation Strategy — The daily awakening sedation strategy (DSI) refers to stopping the continuous infusion of sedation–analgesia medications until the patient is awake and can follow commands, or until the patient exhibits a stress state and is deemed to require resuming sedation. Randomized trials and meta-analyses have reported that DSI is beneficial in reducing the duration of mechanical ventilation and length of hospital stay.
●A similar trial randomized 336 patients to receive daily spontaneous breathing trials and daily spontaneous awakening trials, or to receive daily spontaneous breathing trials and routine sedation. Patients in the daily spontaneous awakening trial group had a lower 1-year mortality rate (though the 28-day mortality rate was not reduced), increased days off the ventilator, and shorter ICU and hospital stays. This group of patients also had less cognitive impairment at 3 months (the absolute risk reduction rate was 20%), but the difference was not statistically significant at 12 months.
Discontinuation — When sedation–analgesia medications are no longer needed, the order and speed of discontinuation must be determined:
●For patients receiving more than one sedation–analgesia medication (e.g., one benzodiazepine plus one opioid), the gradual tapering of opioids to discontinuation should be arranged last, so that the patient does not experience pain upon awakening.
●The rate of tapering should be individualized. Generally, if sedation–analgesia medications have been used for a short duration (≤7 days), abrupt discontinuation is acceptable. Additionally, for patients sedated for more than 7 days with prolonged drug accumulation leading to deep sedation, abrupt discontinuation is also appropriate. However, if patients have been using sedation–analgesia medications for >7 days and there is evidence of rapid tolerance (i.e., requiring increased doses over time to achieve the same level of sedation), gradual tapering is necessary (10%-25% reduction daily).
During the tapering of sedation–analgesia medications, close monitoring for withdrawal symptoms is essential. In such cases, acute withdrawal symptoms appear to be quite common. An observational study involving 28 mechanically ventilated patients hospitalized in the ICU for more than 1 week found that during the tapering of sedation–analgesia medications, 9 patients (32%) experienced acute withdrawal symptoms. The higher the doses of benzodiazepines and opioids, the greater the risk of withdrawal symptoms. Several strategies have been proposed to prevent opioid withdrawal symptoms, including gradual dose reduction, switching to longer-acting oral equivalent medications, switching to long-acting barbiturates (e.g., phenobarbital), and adding α-2 agonists (e.g., clonidine and dexmedetomidine).
Summary and Recommendations
●Before initiating sedation–analgesia medications for stress-induced agitation, the causes of stress should be identified and addressed. Non-pharmacological treatment strategies should also be implemented.
●When non-pharmacological interventions and treatment of the causes of stress are insufficient to control agitation, pharmacological sedation is required.
●The selection of sedation–analgesia medications and their initial doses is based on several factors: the cause of stress, expected duration of treatment, potential drug interactions, desired depth of sedation, and pharmacokinetic variables affecting drug metabolism.
●Continuous infusion of sedation–analgesia medications should not be administered to critically ill patients. Intermittent infusion, continuous infusion guided by sedation protocols, or daily interruptions of continuous infusion are preferable.
●All patients should undergo frequent reassessment to determine whether their agitation and underlying stress have been adequately treated. Sedation–analgesia medications should then be adjusted accordingly, either by gradually adjusting the dose or tapering to discontinuation.
●Once a comfortable state is initially achieved, patients should be frequently reassessed, and the target depth of sedation adjusted. As respiratory failure or other critical illnesses are treated, the need for sedation should decrease. Therefore, attempts to reduce sedation levels should be made daily, but the rate of tapering must be individualized. For patients receiving more than one sedation–analgesia medication, tapering opioids to discontinuation should be done last, so that the patient does not experience pain upon awakening. During the tapering process, close monitoring for withdrawal symptoms is essential.
Crit Care Med. 2018 Sep;46(9):1464-1470.
doi: 10.1097/CCM.0000000000003307.