Today, we will review a condition often manifested by macrodactyly, known as Proteus Syndrome. This article is primarily based on the following references:
1. Jamis-Dow CA, Turner J, Biesecker LG, et al. Radiologic manifestations of Proteus syndrome. Radiographics. 2004; 24(4): 1051-68. doi: 10.1148/rg.244035726
2. He Jingnan, Chen Tao. A case of Proteus syndrome. Chinese Journal of Plastic Surgery, 2021, 37(9): 1003-1006. DOI: 10.3760/cma.j.cn114453-20200430-00257.
Proteus Syndrome is named after the Greek god Proteus, an early sea god whose appearance was unpredictable, making him elusive. Therefore, the medical community named this rare disease, with an incidence of only one in a million, after Proteus. This disease causes excessive tissue growth and can affect any tissue produced by the germ layer. It is usually not apparent at birth but progresses rapidly during childhood. Common manifestations include macrodactyly, vertebral deformities, asymmetrical limb growth and length differences, bone hypertrophy, abnormal and asymmetrical fat distribution, asymmetrical muscle development, connective tissue nevi, and vascular malformations.
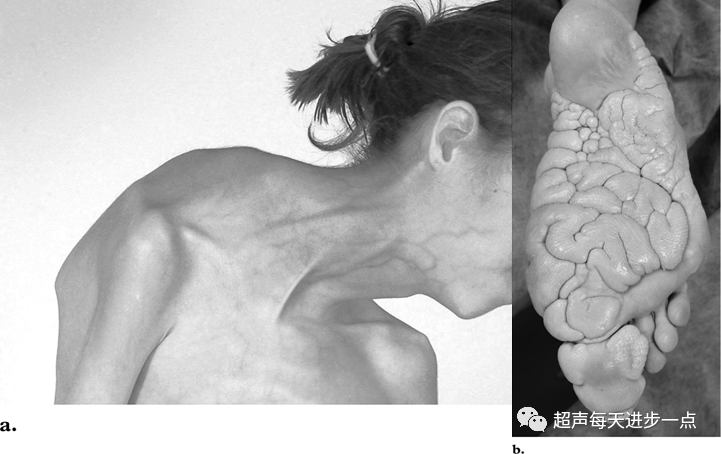 Cervical vertebral deformities and plantar brain-like connective tissue nevi, with the fifth toe removed due to macrodactyly.
Cervical vertebral deformities and plantar brain-like connective tissue nevi, with the fifth toe removed due to macrodactyly.
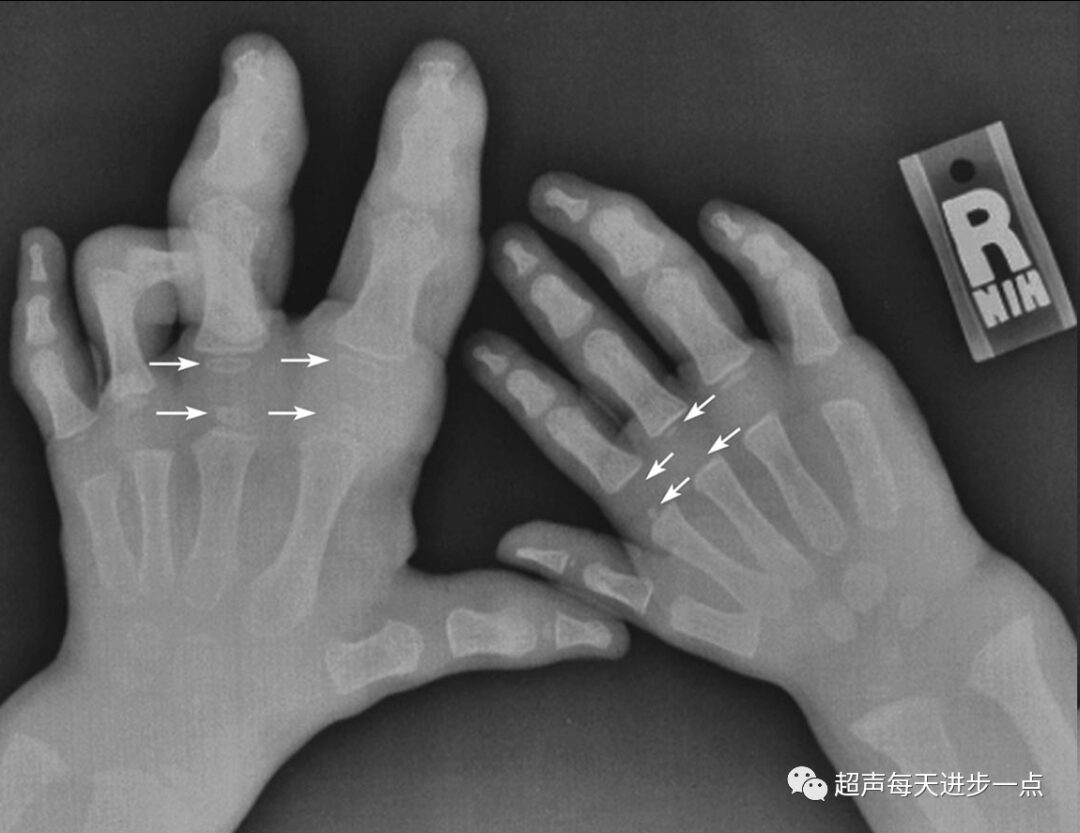 Asymmetrical macrodactyly.
Asymmetrical macrodactyly.
 Unequal lower limb lengths, with femur and fibula deformities.
Unequal lower limb lengths, with femur and fibula deformities.

Bone hypertrophy: In the left image, the patella and tibia; in the right image, the femur and tibia.
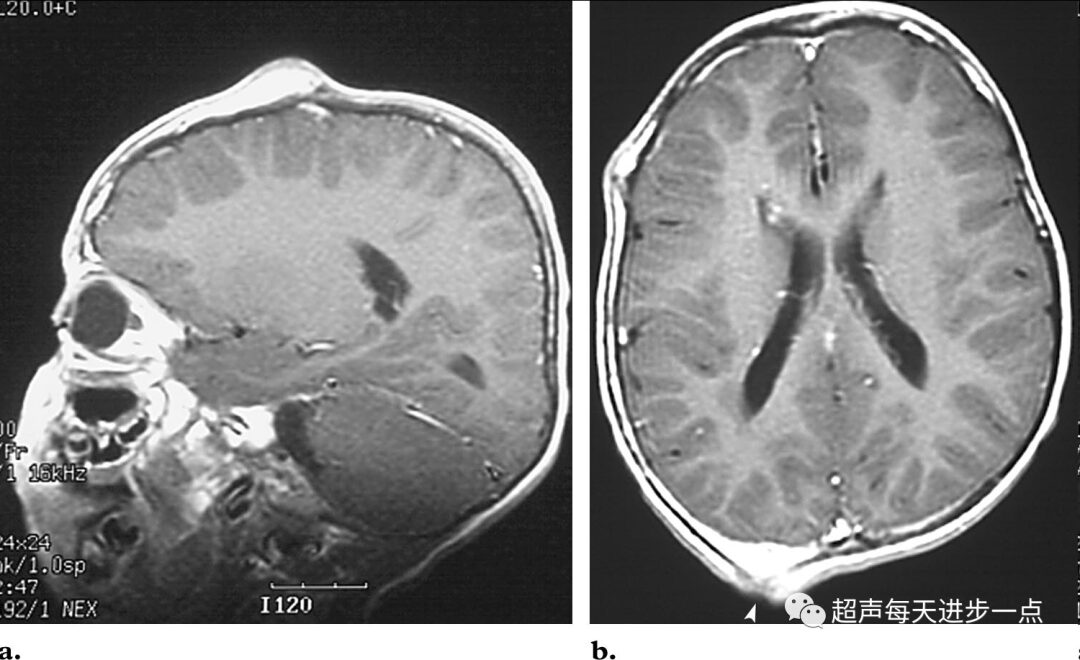
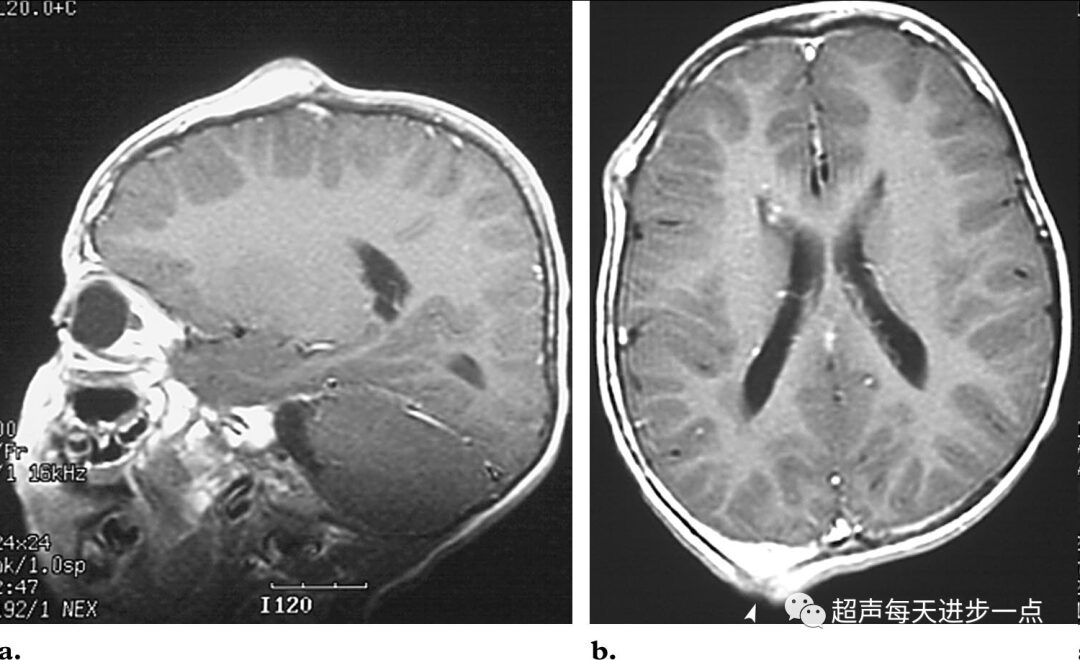 Cranial abnormalities. A 5-year-old patient’s head T1-weighted MRI enhanced image shows several focal bone abnormalities, with some segments of the skull showing expansive lesions of abnormal fat tissue accumulation and focal defects in the right occipital bone (indicated by the arrow in image b).
Cranial abnormalities. A 5-year-old patient’s head T1-weighted MRI enhanced image shows several focal bone abnormalities, with some segments of the skull showing expansive lesions of abnormal fat tissue accumulation and focal defects in the right occipital bone (indicated by the arrow in image b).
Pathogenic gene: Chimeric cell mutations of the AKT1 gene lead to Proteus syndrome. The gene mutation carried by patients is the currently known pathogenic variant for Proteus syndrome, found in approximately 90% of patients.
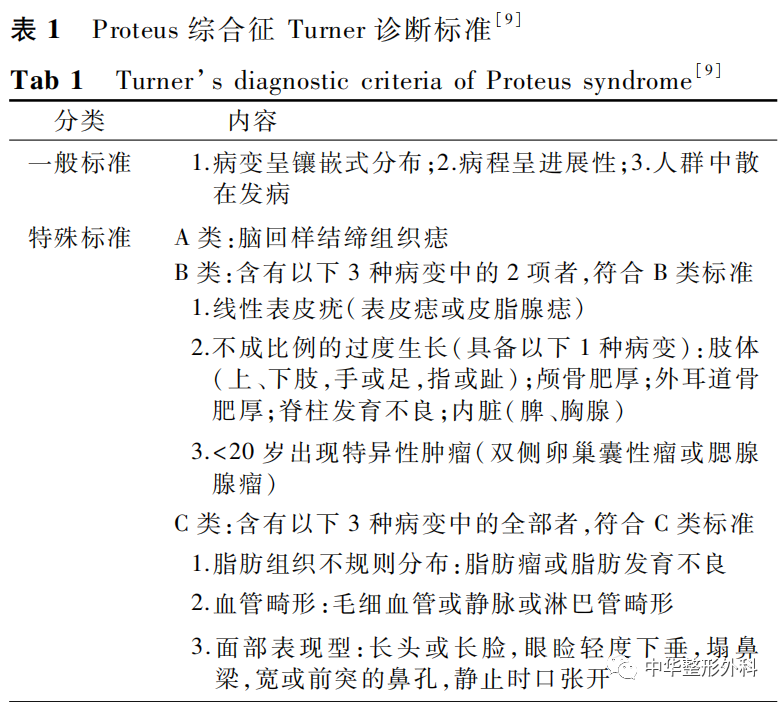
Diagnostic criteria: In 2004, Turner revised the diagnostic criteria, which are now internationally recognized as more precise and stringent. These include “general criteria” and “specific criteria.” Diagnosis of Proteus Syndrome must meet all three items in the “general criteria” and one type of lesion in the “specific criteria” A, B, or C (Table 1).
Differential diagnosis: Mainly compared with Klippel-Trenaunay syndrome, type I neurofibromatosis, and hemihyperplasia–multiple lipomatosis syndrome. Other overgrowth disorders include Maffucci syndrome and Bannayan-Riley-Ruvalcaba syndrome.
The first few are relatively common; let’s discuss the main manifestations of the latter two syndromes:
Bannayan-Riley-Ruvalcaba syndrome: A hereditary syndrome characterized by macrocephaly, multiple subcutaneous and visceral lipomas, vascular and bone deformities. There are venous capillary and lymphatic malformations in the skin and viscera, multiple skin lipomas, macrocephaly, genital freckle-like nevi, warts, and acanthosis nigricans.
Maffucci syndrome: Known as enchondromatosis-hemangiomatosis syndrome, also called enchondromatosis with multiple hemangiomas (mainly venous malformations). The onset is mainly between 1 to 5 years old, primarily affecting the small bones of the hands and feet with cartilage tumors that can develop into chondrosarcoma and progressive cartilage hypoplasia, with flat bones rarely affected.