Click the “blue WeChat name” below the title to quickly follow
Source:Chinese Journal of Neurology, 2022, 55(10): 1200-1208
Authors:Huang Jiaqi, Zhu Yulan
Abstract
The circadian rhythm is driven by the biological clock in the suprachiasmatic nucleus, regulating many life activities and physiological functions, such as central nervous system activity, autonomic nervous system activity, endocrine function, metabolism, and immune function. At the molecular level, the circadian rhythm is regulated by the molecular mechanisms generated by the oscillation of clock genes. The endogenous circadian rhythm is one of the main processes controlling sleep. Disruption of the circadian rhythm can lead to various physiological dysfunctions, most commonly resulting in abnormalities in the sleep-wake cycle, but it can also lead to other sleep disorders, cognitive dysfunction, hypertension, diabetes, and a series of diseases and adverse consequences. Recently, the connection between circadian rhythms and sleep-wake has increasingly attracted researchers’ attention. This article reviews the research progress on circadian rhythms and circadian rhythm sleep-wake disorders.
The rotation of the Earth creates the alternation of day and night and temperature changes. To adapt to periodic environmental changes, most physiological processes in organisms exhibit periodic fluctuations of about 24 hours, known as circadian rhythms. The circadian rhythm is driven by the biological clock in the suprachiasmatic nucleus, regulating many life activities and physiological functions, such as central nervous system activity, autonomic nervous system activity, endocrine function, metabolism, and immune function. At the molecular level, the circadian rhythm is regulated by the molecular mechanisms generated by the oscillation of clock genes. Under optimal physiological conditions, the circadian rhythm is stable, life activities operate synchronously, and various physiological functions reach their best. The endogenous circadian rhythm is one of the main processes controlling sleep and may be influenced by external factors such as natural light, activity, and meal times. Disruption of the circadian rhythm can lead to various physiological dysfunctions, most commonly resulting in abnormalities in the sleep-wake cycle, but it can also lead to other sleep disorders, cognitive dysfunction, hypertension, diabetes, and a series of diseases and adverse consequences. We searched relevant reviews and randomized controlled trials in domestic databases such as CNKI, Wanfang, and Weipu, as well as international databases like PubMed and Embase, using keywords such as “circadian rhythm,” “sleep disorders,” and “biological clocks” to review literature from 2002 to 2022.
1. Origin of Circadian Rhythm and Biological Clocks
The circadian rhythm is the result of long-term evolution of organisms, helping them adapt to environmental changes and regulate physiological activities. Even after explosive evolution and mass extinction events, the characteristic of circadian rhythm still exists in organisms, indicating that circadian rhythm was internalized early in biological evolution rather than acquired as a characteristic later.[3] The circadian rhythm is driven by an endogenous timing system, and almost all organisms on Earth, from simple unicellular cyanobacteria to mammals and humans, have circadian clocks, also known as biological clocks. The biological clock consists of a central clock and peripheral clocks.[5, 6]
(1) Central Clock
The central clock is located in the suprachiasmatic nucleus (SCN) of the hypothalamus.[7] The SCN is a bilateral structure located in the anterior part of the hypothalamus and serves as the central pacemaker controlling physiological rhythms. The SCN consists of about 20,000 clock neurons, all containing molecular mechanisms that can function as independent cellular oscillators when cultured in isolation.[8]
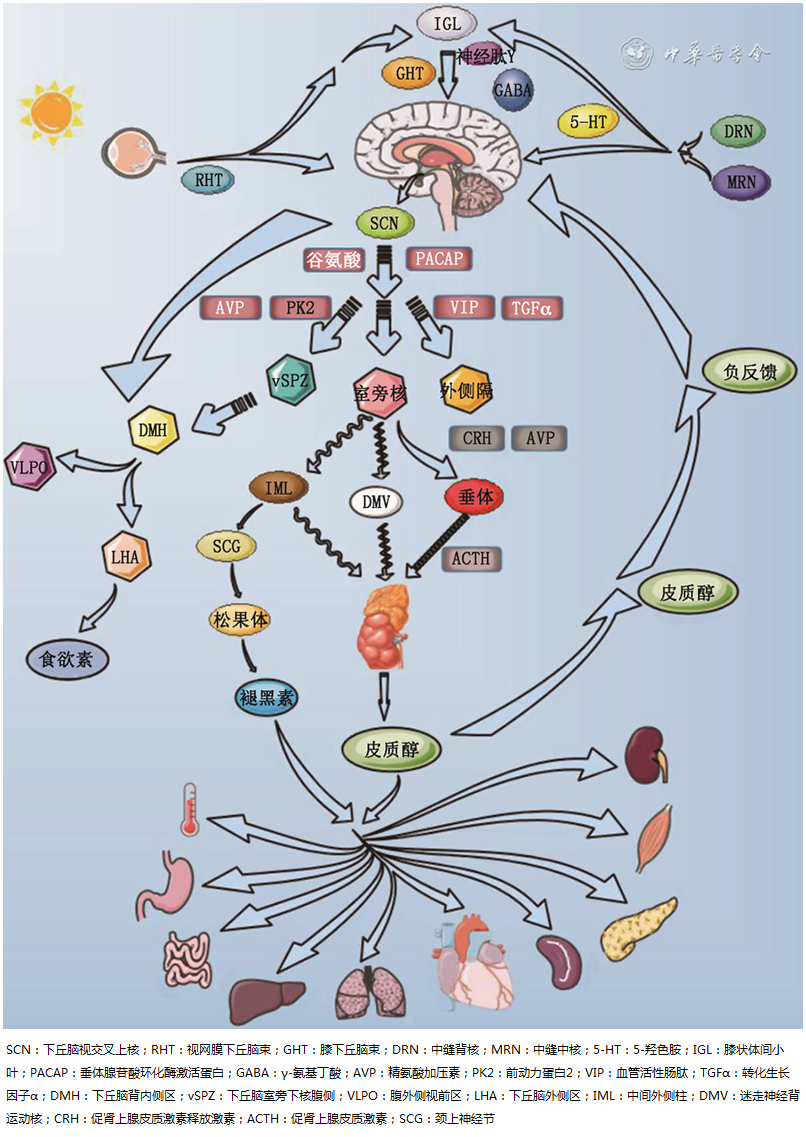
As the central pacemaker, the SCN receives, converts, and integrates light-dark cycle signals from the retina-hypothalamic pathway and sends out synchronized instructions.[4] The SCN has three main input pathways: the retinohypothalamic tract (RHT), the geniculohypothalamic tract (GHT), and the serotonergic pathways from the dorsal raphe nucleus and median raphe nucleus, which transmit light signals to multiple sleep-wake-related nuclei, participating in the transition between sleep and wakefulness, as detailed in Figure 1. The plasticity of brain structures is essential for the neural coding of light information and the adjustment of corresponding physiological behaviors.[9] Among them, the RHT mediates light information, while the intergeniculate leaflet (IGL) and the raphe nuclei provide non-light information to the SCN. Mammals primarily perceive light information through the retina, where photosensitive retinal ganglion cells (pRGCs) express the photopigment melanopsin, transmitting light information to the SCN via the RHT. Additionally, the RHT projects to the IGL, which releases neuropeptide Y and gamma-aminobutyric acid (GABA) to indirectly project to the SCN, thereby transmitting and processing light information. The IGL not only receives information from the retinal RHT but is also stimulated by non-light information from the dorsal raphe nucleus. Meanwhile, serotonergic pathways are involved in the non-light regulation from the dorsal raphe nucleus and median raphe nucleus and the regulation of the circadian clock. The most extensively studied output signal from the SCN is prokineticin 2 (PK2), whose receptors are expressed in many known brain regions receiving signals from the SCN, including the dorsomedial hypothalamus (DMH), paraventricular nucleus, and lateral hypothalamus.
Figure 1 Schematic diagram of circadian clock related regulatory pathways (Figure 1 is original by authors)
图1 Schematic diagram of circadian clock related regulatory pathways (Figure 1 is original by authors)
(2) Peripheral Clocks
In addition to regulating the rhythms of their own tissues, the SCN also transmits information to peripheral effectors through various body fluid signals and three main types of neurons as shown in Figure 1: (1) sympathetic projection neurons targeting intermediolateral columns (IML) spinal preganglionic neurons; (2) parasympathetic projection neurons targeting the dorsal motor nucleus of the vagus (DMV); (3) neuroendocrine neurons controlled by the paraventricular nucleus.[10]
The SCN indirectly regulates the rhythms of hormones such as adrenal cortex and cortisol through the paraventricular nucleus, while also indirectly controlling the function of the pineal gland through the superior cervical ganglion (SCG) to regulate the rhythms of melatonin and other hormones. Hormonal information from the adrenal gland feeds back to the central clock and transmits to peripheral clocks. The peripheral clocks regulated by the central clock and clock genes are present in almost all peripheral tissues and organs, including the heart, lungs, liver, and kidneys.[11, 12] Therefore, many important physiological factors, such as blood pressure[13], body temperature, immunity, metabolism, aging, hair growth, and pigmentation, exhibit strong circadian rhythm variations.[14, 15, 16] The expression of peripheral clock genes reflects the length, phase, and amplitude of the individual cycle, which can serve as a suitable and easily obtainable biomarker to assess molecular-level circadian rhythm disruptions. In summary, circadian rhythms play a crucial role in coordinating various complex life activities.
2. Circadian Rhythm Sleep-Wake Disorders (CRSWD)
(1) Definition
CRSWD is a type of disorder characterized by sleep structure disruption and abnormal cycles caused by changes in the circadian timing system and circadian rhythm guidance mechanisms, or misalignment between the endogenous circadian rhythm and the external environment.[18, 19] It can impair social functioning and further affect health, safety, and work or study.
(2) Classification
The International Classification of Sleep Disorders categorizes sleep disorders into seven major categories, including CRSWD. CRSWD is divided into exogenous and endogenous types.[20] Exogenous CRSWD includes jet lag sleep disorder and shift work sleep disorder. Endogenous CRSWD includes delayed sleep-wake phase disorder (DSWPD), advanced sleep-wake phase disorder (ASWPD), irregular sleep-wake rhythm disorder (ISWRD), and non-24-hour sleep-wake rhythm disorder (N24SWD).
3. Mechanisms Related to Circadian Rhythm and CRSWD
(1) Circadian Rhythm and Sleep-Wake Regulation Model
Sleep and wakefulness are regulated by a dual process model of sleep regulation, namely “Process S” and “Process C”.[7] The homeostatic drive for sleep (Process S) is proportional to the duration of wakefulness. Conversely, the circadian pacemaker regulating wakefulness (Process C) generates a wakefulness drive that is opposite to Process S and depends on the individual’s inherent circadian rhythm.[14] Core body temperature and melatonin rhythms are markers of Process C. When an individual’s circadian rhythm is disrupted, sleep disorders occur, and this coordination of sleep-wake rhythms is provided by SCN neurons.[12] The SCN sends alerting signals during the day to help maintain wakefulness, while melatonin secreted by the pineal gland at night inhibits the SCN, reducing alerting signals to maintain sleep. Meanwhile, the SCN projects directly or indirectly through the ventral subparaventricular zone (vSPZ) neurons to the dorsomedial hypothalamus (DMH). DMH neurons continue to project to the ventrolateral preoptic area (VLPO) neurons to send rhythmic signals and to the lateral hypothalamic area (LHA) related nuclei to promote orexin secretion, stabilizing the transition between sleep and wakefulness, as detailed in Figure 1.
(2) Molecular Mechanisms of Circadian Rhythm
At the molecular level, circadian rhythms are composed of multiple transcription-translation feedback loops that drive the rhythmic transcription of core clock genes.[3, 11] This cycle takes 24 hours to complete. The precise 24-hour cycle is controlled by post-translational modifications such as phosphorylation, ubiquitination, and acetylation.[3, 21, 22]
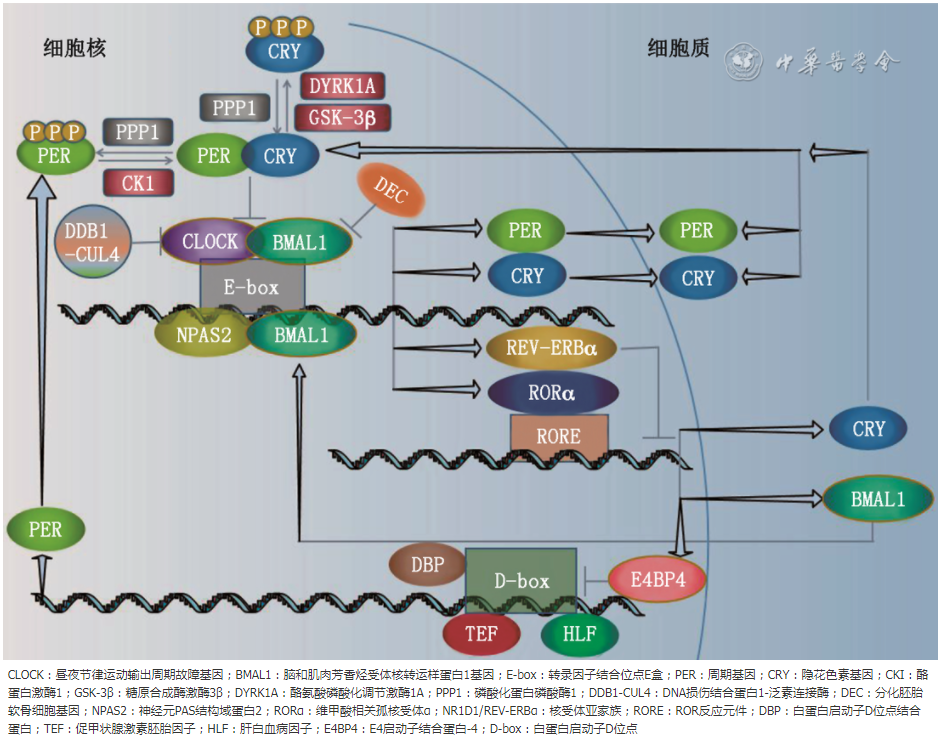
In the morning, the circadian locomotor output cycles kaput gene (CLOCK) and brain and muscle aryl hydrocarbon receptor nuclear translocator-like protein-1 gene (BMAL1) form a heterodimer in mammals, activating the transcription of target genes such as period gene (PER) and cryptochrome gene (CRY) by binding to the E-box transcription factor binding sites in the promoter. In the evening, PER and CRY proteins accumulate in the cytoplasm, dimerize, and are transferred back to the nucleus, acting on the CLOCK-BMAL1 complex to inhibit its transcription, achieving a negative feedback mechanism.[23, 24] Casein kinase 1 (CKI), glycogen synthase kinase-3β (GSK-3β), and dual-specificity tyrosine-regulated kinase 1A (DYRK1A) mediate the phosphorylation of PER and CRY, which is antagonized by the phosphoprotein phosphatase 1 (PPP1). The CLOCK-BMAL1 complex also reduces its affinity for E-box sites through covalent modifications of gene chromatin via DNA damage binding protein 1 (DDB1)-Cullin-4 (CUL4) ubiquitin ligase. The differentiated embryonic chondrocyte gene (DEC) can competitively inhibit the transcription of the CLOCK-BMAL1 complex. Neuronal PAS domain protein 2 (NPAS2) can replace CLOCK to form a transcriptionally active complex with BMAL1, compensating for the loss of CLOCK in peripheral cells and the SCN.[25]
Retinoid acid receptor related orphan receptor α (RORα) and nuclear receptor subfamily 1 group D member 1 (NR1D1/REV-ERBα) act through ROR response elements (RORE) in the promoter.[8] This forms a positive-negative feedback network.[3]
Various transcription factors, including D site albumin promoter binding protein (DBP), thyrotroph embryonic factor (TEF), and hepatic leukemia factor (HLF) as positive regulators, and E4 promoter-binding protein 4 (E4BP4) as a negative regulator, interact with the D-box in target genes such as PER1-3 and RORα.[22] See Figure 2.
Figure 2 Schematic diagram of the circadian clock molecular mechanism loop (Figure 2 is original by authors)
图2 Schematic diagram of the circadian clock molecular mechanism loop (Figure 2 is original by authors)
Additionally, regulatory mechanisms such as gene polymorphisms,[26] chromatin remodeling, transcription factor network interactions, RNA modifications, post-transcriptional regulation, selective splicing, and post-translational regulation of subcellular transport and protein degradation impact the transcription-translation feedback loop regulating circadian clock behavior.[8]
(3) Mechanisms of CRSWD
Currently, there are no reports on the regulatory mechanisms of CRSWD, which may be related to disruptions in any link of the aforementioned regulatory processes, thereby affecting sleep structure and homeostasis. This may become a target for exploring the mechanisms of CRSWD, requiring further long-term research.
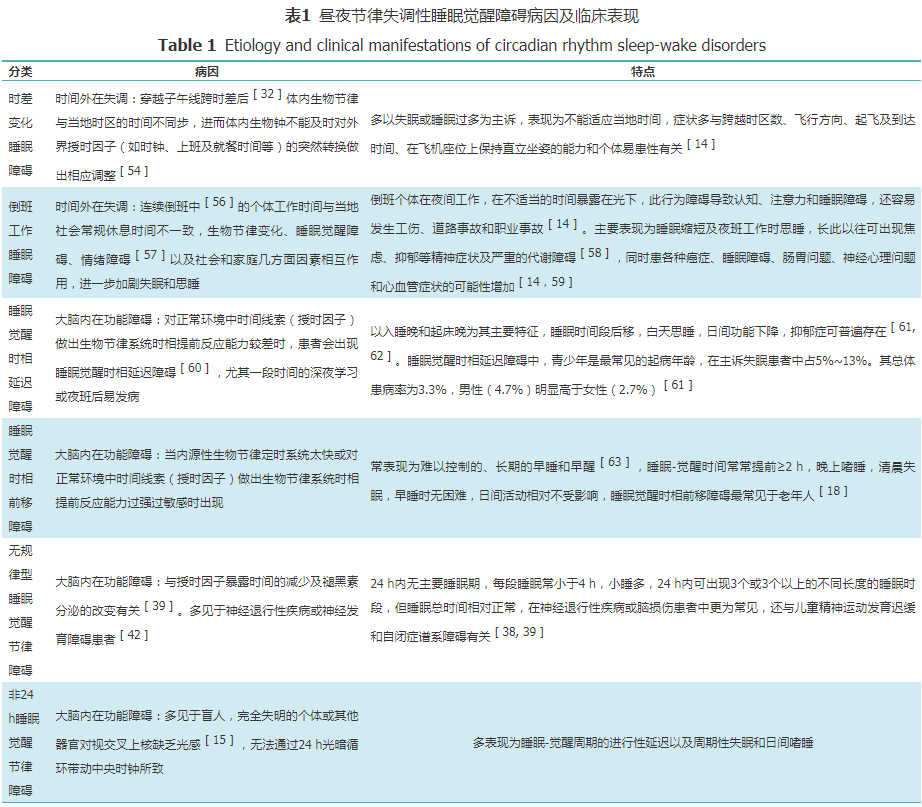
4. Etiology and Clinical Manifestations of CRSWD
CRSWD presents a variety of manifestations, each with its specific etiology and clinical features, summarized in Table 1.
5. Progress in Diagnosis and Treatment of CRSWD
(1) Diagnostic Criteria
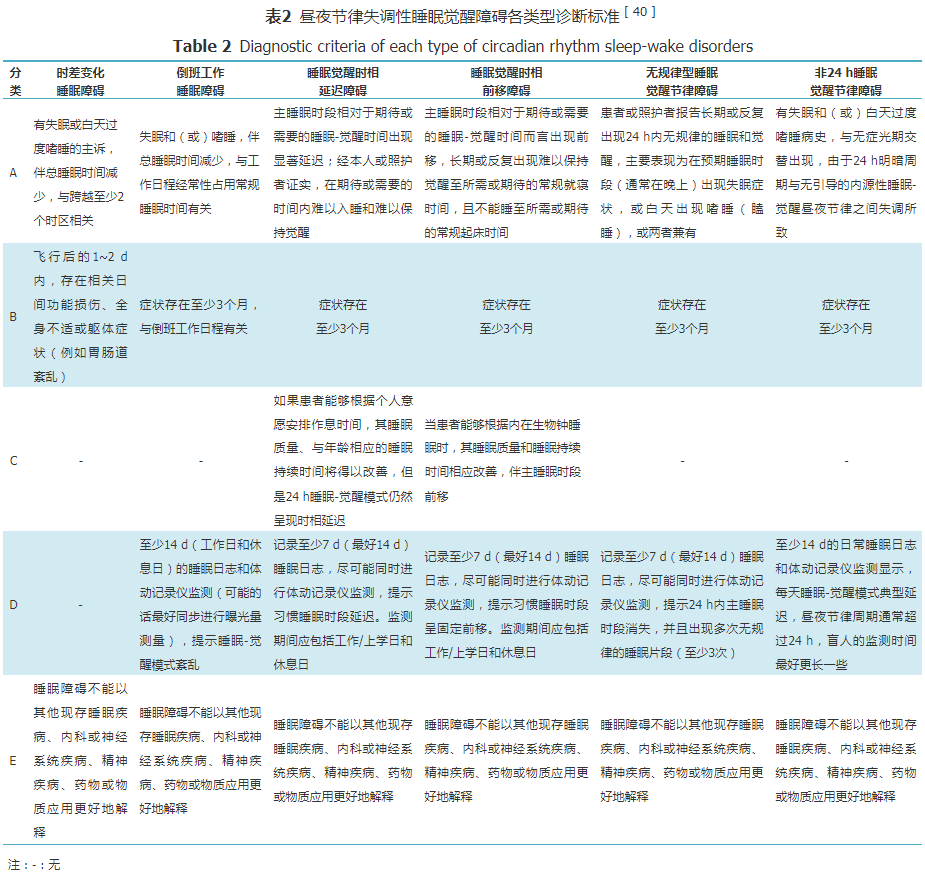
Currently, there are few reported diagnostic criteria for circadian rhythm disorders, and specific time limits for sleep delay or advance are not clearly defined. Many clinical trials use self-defined standards for inclusion, while the diagnostic criteria for circadian rhythm disorders in the book “Clinical Sleep Disorders” (Zhao Zhongxin, ed. Shanghai: Second Military Medical University Press, 2003) are more detailed and clear. The currently recognized diagnostic criteria for CRSWD come from the International Classification of Sleep Disorders (3rd edition, ICSD-3): (1) Long-term or recurrent sleep-wake rhythm disorders primarily due to changes in the endogenous circadian rhythm timing system, or due to misalignment between the individual’s endogenous circadian rhythm and the expected or required physiological environment or social and work schedules; (2) Circadian rhythm disruption leads to a series of insomnia or hypersomnia, or both; (3) Sleep-wake rhythm disorders lead to clinically significant distress or impairment in psychological, physiological, social, occupational, educational, and other important functions. ICSD-3 also proposes diagnostic criteria for each type of CRSWD (Table 2).
(2) Treatment Progress
1. Chronotherapy: Chronotherapy can be used to change the sleep-wake cycle of CRSWD patients,[28] invented by Czeisler and colleagues in 1981. Chronotherapy involves creating an individualized sleep-wake schedule for patients, such as going to bed later or earlier by 2-3 hours each week, gradually adjusting sleep times until reaching the desired sleep-wake schedule and maintaining it. This therapy aims to ensure that patients can receive light therapy and melatonin at appropriate times to restore proper circadian rhythm patterns,[29] which helps to establish a self-balancing sleep drive. Recent case reports have shown that chronotherapy successfully alleviated sleep disorders in two DSWPD patients during the COVID-19 pandemic.[30] However, chronotherapy was proposed early on and is limited to case studies, with few large population randomized controlled trials assessing its efficacy in recent years. The limitation of this therapy is that it is effective in the short term after treatment but difficult to maintain long-term effects. During the treatment period, patients will sleep during the day and be awake at night, requiring a flexible schedule, which greatly limits the clinical application of chronotherapy.
2. Light Therapy: Light therapy affects the endogenous circadian rhythm by suppressing melatonin secretion through light exposure.[31] Light exposure before dim light melatonin onset (DLMO) and the lowest core body temperature delays the circadian rhythm, while light exposure afterward advances the circadian rhythm.[32] Evening or nighttime exposure to various intensities of light can induce light-induced suppression of melatonin secretion,[33] increasing the risk of CRSWD and worsening the condition of existing DSWPD patients; therefore, these patients should avoid light exposure at night.[34] The beneficial effects of light therapy on synchronizing circadian rhythms, improving sleep quality, and enhancing cognitive abilities depend not only on the spectral composition of the light but also on the timing and intensity of exposure.[35] DSWPD patients can use full-spectrum bright light, typically at 2,500 lx or brighter, for 2 hours after waking up.[2] Studies have shown that blue light has a more powerful effect, as human circadian rhythms are most sensitive to short-wavelength blue light (approximately 460-480 nm).[7, 31] Although potential side effects include eye fatigue, headaches,[36] nausea, and agitation, these symptoms often resolve spontaneously. Light therapy can trigger migraines in about one-third of susceptible patients, but treatment-induced headaches usually also resolve.[27] No serious adverse events have been reported for light therapy.[37]
ASWPD patients should be exposed to light later in the afternoon or early evening. Research results indicate that evening light improves subjective alertness in elderly patients with sleep difficulties, increases alpha EEG activity during wakefulness, and prolongs rapid eye movement latency, indicating that light therapy is beneficial for early evening drowsiness.[38] Generally, the combination of light therapy and melatonin is more effective than using either alone. The combination of bright light therapy, chronotherapy, and vitamin B12 may be beneficial for ISWRD. Daily exposure to 3,000-5,000 lx of light for 2 hours over 4 weeks can improve daytime alertness, but its effect on consolidating nighttime sleep is limited.[39]
3. Melatonin Therapy: Melatonin is a physiological hormone related to sleep timing, typically secreted by the pineal gland about 2 hours before habitual sleep time, gradually reaching a peak and sharply decreasing after night ends. Melatonin can be measured from plasma, saliva, or urine and is a reliable biomarker of circadian rhythm.[2] Melatonin is considered a drug at supraphysiological doses,[32] and taking it before sleep helps increase sleep duration and improve sleep quality, and it has been used exogenously for the treatment of primary and secondary sleep disorders. Exogenous melatonin can reduce sleep onset latency in DSWPD and primary insomnia patients and regulate sleep-wake patterns in blind individuals.[40] However, the effectiveness of exogenous melatonin may be reduced if patients continue to produce endogenous melatonin, and it has been reported that using the beta-blocker metoprolol to suppress endogenous melatonin secretion in conjunction with exogenous melatonin may benefit CRSWD patients.[41]
Taking melatonin at night advances the biological clock, while taking it in the morning delays the biological clock.[14] Studies have shown that doses of 0.3-3.0 mg of melatonin have resetting effects on circadian rhythms, while doses of 10 mg or more have smaller resetting effects. Some researchers believe that administering melatonin 3-6 hours before DLMO is more effective and should be done with small doses to avoid high melatonin levels in the morning. Although the precise timing of melatonin administration varies across studies, the optimal dose has not been determined. However, considering the physiological characteristics of melatonin secretion and synthesizing results from most literature, patients can take 0.3-5.0 mg of melatonin 3-6 hours before their expected endogenous melatonin secretion time, which is typically after their habitual sleep time.[7, 42]
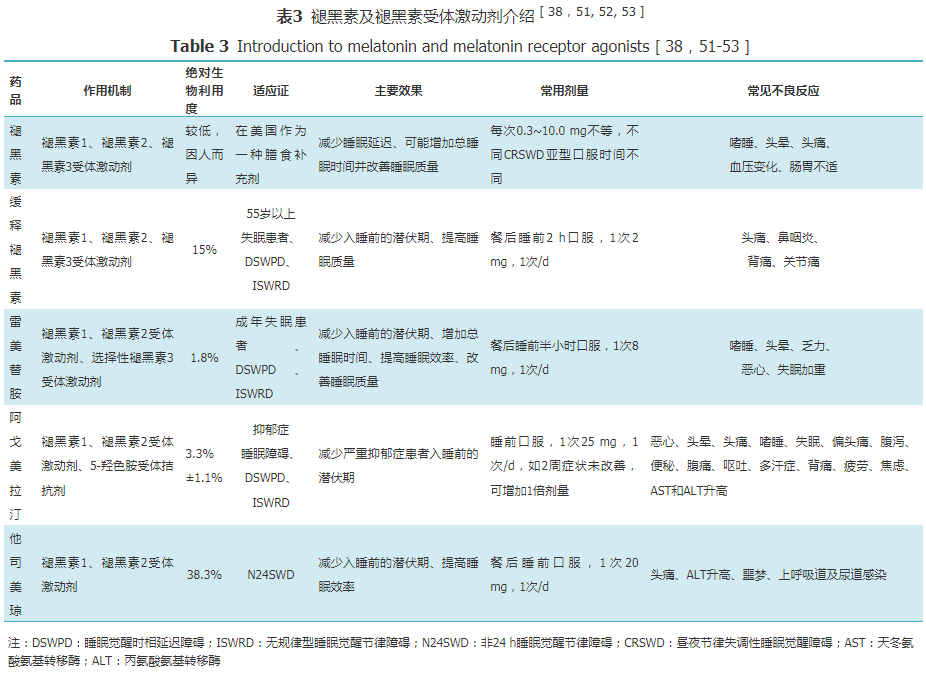
Currently, three subtypes of melatonin receptors have been identified: melatonin receptor 1, melatonin receptor 2, and melatonin receptor 3.[43] Melatonin receptors 1 and 2 are G-protein-coupled receptors, while melatonin receptor 3 is a quinone receptor found in plants. Melatonin primarily acts on melatonin receptors 1 and 2, resetting circadian rhythms and promoting sleep.[15] Recently introduced prolonged-release melatonin and melatonin receptor agonists such as ramelteon, agomelatine, and tasimelteon help regulate sleep-wake phases, each with distinct characteristics (Table 3).
Reports have indicated that administering 4 mg of ramelteon to a 15-year-old female patient with DSWPD at 7 PM successfully restored her sleep-wake rhythm to normal.[43] Tasimelteon, as a dual melatonin receptor agonist, has a high affinity for the MT2 receptor and is the only pharmacological therapy approved by the FDA and EMA for N24SWD patients.[44] Moreover, no safety concerns have been found for a single oral dose of 20 mg in patients with mild to moderate liver dysfunction or severe renal dysfunction, so no dosage adjustment is necessary in these patients.
However, more than 90% of cases relapse after discontinuing melatonin for one week, indicating that the effects of melatonin may require long-term use to maintain. Considering the good safety profile of melatonin,[42] and that the potential benefits of treatment outweigh the risks, clinicians may use longer melatonin courses for more severe DSWPD and N24SWD patients to provide a more sustained therapeutic response. For patients with ISWRD and developmental delays, doses of 2-20 mg of melatonin can improve and consolidate sleep patterns and reduce daytime sleep. Although appropriate doses of melatonin theoretically may improve symptoms in ASWPD patients, its sedative effects may make it difficult for patients to stay awake, so the American Academy of Sleep Medicine does not recommend morning supplementation of melatonin or melatonin receptor agonists for ASWPD.[7]
Adverse reactions from melatonin, such as drowsiness, dizziness, headaches, and low body temperature, are often mild,[45] and do not prompt patients to discontinue treatment. However, some studies have shown that exogenous melatonin treatment is associated with impaired glucose tolerance, and clinical doses (5 mg) of melatonin negatively affect glucose tolerance. Therefore, for patients with glucose intolerance or at risk for type 2 diabetes, the optimal timing may be at least 2 hours after the last meal to allow for normal blood sugar recovery before using melatonin, avoiding related glucose tolerance impairment.[46] Melatonin has been shown to be twice as active as vitamin E and is considered the most effective lipophilic antioxidant,[47] so caution should be exercised in patients using warfarin. Patients with dementia, epilepsy, asthma, and pregnant or breastfeeding women should avoid melatonin supplementation.[39, 45]
4. Other Therapies: Benzodiazepines and non-benzodiazepine hypnotics should be used cautiously due to their adverse reactions.[48] Especially in patients with dementia or brain injury, their use may further exacerbate cognitive dysfunction. Cognitive-behavioral therapy (CBT), including stimulus control, motivational interviewing, and relaxation strategies, can improve sleep perception.[49, 50] Research results indicate that CBT is more suitable for middle-aged women.[51] According to the clinical practice guidelines published by the Japanese Sleep Research Society on the appropriate use and cessation of sleep medications, CBT is positioned as a second-line treatment when pharmacotherapy fails. Educating patients on sleep hygiene behaviors also aids in the diagnosis and treatment of sleep disorders.[52] ISWRD is more common in neurodegenerative diseases such as dementia, so treatment of the underlying disease should not be overlooked.[7] Additionally, metabolic disorders related to sleep deprivation may be mediated by the excessive growth of specific gut bacteria, and it has been found that probiotic supplementation can improve subjective sleep quality.[53]
6. Conclusion and Outlook
Given the widespread presence of circadian rhythm biological clocks in the brain and peripheral tissues, controlling numerous physiological processes, when circadian rhythm disruptions occur, various aspects of the body are significantly affected.[54, 55] When other diseases are present, circadian rhythm disruptions are predictable. Therefore, research on CRSWD patients, including assessments of internal and/or external circadian rhythm disruptions and evaluations of the amplitude of central and peripheral circadian rhythms, may provide unique opportunities for scientific discovery. To this end, further basic research and clinical observations are needed to identify the output pathways of clock genes at the molecular level and their potential mechanisms for regulating peripheral clocks. Clinicians should consider that circadian rhythm disruptions are significant potential risk factors for sleep disorders, while also recognizing the various adverse impacts of CRSWD on patients’ daily lives and the critical importance of comprehensive treatment, actively considering available and potentially effective treatment options, which will help further enhance clinical diagnosis and treatment and optimize care.
References omitted