【Live Broadcast Preview↓↓↓】
The defibrillator, also known as an electric cardioversion machine, is a medical electronic device that applies electric shocks to rescue and treat arrhythmias. It has advantages such as high efficacy, rapid action, ease of operation, and relative safety compared to medications, and is widely used in medical units at all levels in the military.
Working Principle of the Defibrillator
The method of eliminating arrhythmias and restoring sinus rhythm by passing a strong pulse current through the heart is called electric defibrillation or cardioversion. Both pacing and defibrillation utilize exogenous current to treat arrhythmias, and both are modern methods for treating arrhythmias. The difference between cardiac pacing and cardiac defibrillation is that the latter applies a single instantaneous high-energy pulse during defibrillation, generally lasting 4 to 10 ms, with energy levels ranging from 40 to 400 J (joules). The device used for cardiac electric defibrillation is called a defibrillator, which can perform electric cardioversion, i.e., defibrillation. When a patient experiences severe rapid arrhythmias, such as atrial flutter, atrial fibrillation, or supraventricular or ventricular tachycardia, it often leads to varying degrees of hemodynamic impairment.
The original defibrillator used industrial AC power directly for defibrillation, which often resulted in casualties due to electric shock. Therefore, currently, aside from using AC power for in-body defibrillation (ventricular fibrillation) during cardiac surgery, DC power is generally used for defibrillation.
The voltage converter transforms low-voltage DC into high-voltage pulses, which charge a storage capacitor C after high-voltage rectification, allowing the capacitor to store a certain amount of energy. During defibrillation treatment, the high-voltage relay K is controlled to cut off the charging circuit, connecting the storage capacitor C, inductor L, and the human body (load) in series, forming an RLC (where R is the sum of the body’s resistance, the resistance of the wire itself, and the contact resistance between the body and the electrode) series resonant decaying oscillation circuit.
In addition to the above charging and discharging circuits, the cardiac defibrillator should also have monitoring devices to check the progress and effectiveness of defibrillation in a timely manner.
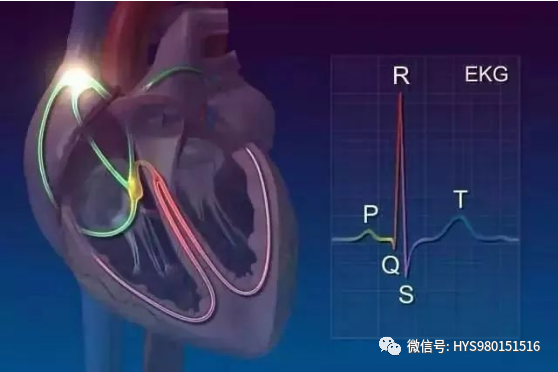
There are two types of monitoring devices: one is an electrocardiogram (ECG) oscilloscope, which observes the output waveform of the defibrillator on the oscilloscope screen for monitoring; the other is an automatic recorder, similar to an ECG machine, which automatically records the output waveform of the defibrillator and the ECG on recording paper for monitoring purposes. Of course, some devices have both functions, allowing observation of waveforms on the screen while also automatically recording them.
Some cardiac emergency devices combine a cardiac pacemaker, defibrillator, monitor, and automatic recorder into one, making it a good instrument for cardiac emergencies.
Classification of Defibrillators
(1) Classified by Synchronization with R-Wave
1. Asynchronous defibrillator. This type of defibrillator is not synchronized with the patient’s own R-wave during defibrillation and can be used for ventricular fibrillation and flutter (because there is no R-wave with sufficiently high amplitude and slope).
2. Synchronized defibrillator. This type of defibrillator is synchronized with the patient’s own R-wave during defibrillation. It generally uses an electronic control circuit to control the release of current pulses with the R-wave, ensuring that the electric shock pulse coincides with the descending phase of the R-wave, thus avoiding the electric shock pulse falling into the vulnerable period, thereby preventing ventricular fibrillation. It can be used for all rapid arrhythmias other than ventricular fibrillation and flutter, such as supraventricular and ventricular tachycardia, atrial fibrillation, and flutter.
(2) Classified by Electrode Placement
1. Internal defibrillator. This type of defibrillator places electrodes inside the chest in direct contact with the myocardium for defibrillation. Early defibrillation was mainly used for direct myocardial electric shocks during open-heart surgery, and this type of internal defibrillator has a simple structure. Modern internal defibrillators are implantable, which is different from early internal defibrillators; they can automatically defibrillate, monitor ECG, judge arrhythmias, and select therapies.
2. External defibrillator. This type of defibrillator places electrodes outside the chest, indirectly contacting the myocardium for defibrillation. Most defibrillators currently used clinically belong to this type.
Clinical Applications
1. Equipment
The electric cardioversion machine, also known as a defibrillator, is the main device for performing electric cardioversion. It is equipped with electrode plates, typically in two sizes: larger ones for adults and smaller ones for children. Before use, check if all functions of the defibrillator are intact, if there are any faults in the power supply, if the charge is sufficient, and if there are any broken wires or poor contact. As a rescue device, the defibrillator should always maintain good performance, with the battery charged sufficiently to be ready for emergency electric defibrillation at any time.
2. Electrodes
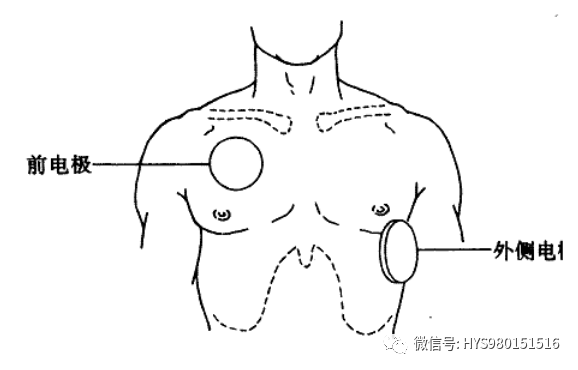
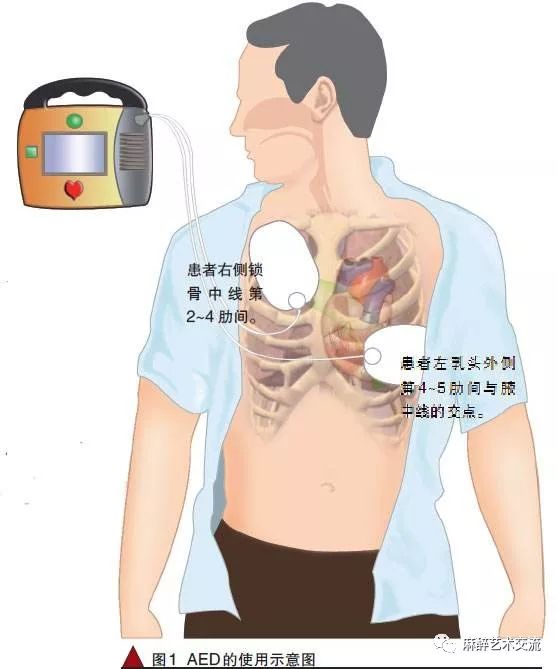
During external electric cardioversion, there are two ways to place the electrode plates. One is called the anterior-posterior position, where one electrode plate is placed under the scapula at the back, and the other is placed horizontally at the left edge of the sternum between the 3rd and 4th ribs. Some believe this method allows more current to flow through the heart, requiring less energy and potentially reducing complications. Selective electric cardioversion should adopt this method. The other method places one electrode plate at the right edge of the sternum between the 2nd and 3rd ribs (the heart’s base) and the other at the left anterior axillary line at the 5th intercostal space (the apex of the heart). This method is quick and convenient, suitable for emergency electric defibrillation. The distance between the two electrode plates should not be less than 10 cm. The electrode plates should be pressed tightly against the patient’s skin with slight pressure, leaving no gaps, and the edges should not be lifted. The skin at the electrode placement site should be coated with conductive paste, saline-soaked gauze can also be used, and in emergencies, even clean water can be used, but alcohol must be strictly avoided as it can cause skin burns. For thin patients with prominent intercostal spaces leading to poor contact between the electrodes and the skin, saline-soaked gauze can be used, applying several layers to improve contact between the skin and the electrodes. The two electrode plates should remain dry to avoid short circuits caused by conductive paste or saline connecting them. The handles of the electrode plates should also be kept dry, free from contamination by conductive paste or saline to prevent harm to the operator. When direct electric defibrillation of the heart is needed during cardiac surgery or open-heart massage, specialized small electrode plates are required, with one placed on the right ventricular surface and the other at the apex of the heart, with physiological saline sprinkled on the heart’s surface and the electrode plate pressed against the ventricular wall.
3. Selection of Electrical Energy
The electrical energy used for cardioversion is indicated in J (joules). Charge according to the needs: for ventricular fibrillation, 250 J to 300 J for asynchronous cardioversion; for ventricular tachycardia, 150 J to 200 J; for atrial fibrillation, 150 J to 200 J; for atrial flutter, 80 J to 100 J; for supraventricular tachycardia, 100 J, all for synchronized cardioversion.
Operation Steps
1. Prepare all necessary items at the bedside and turn on the power.
2. Expose the patient’s chest and establish ECG monitoring if necessary.
3. Determine the type of arrhythmia the patient has.
4. Evenly apply conductive gel to the electrode plates.
5. Select appropriate energy: synchronized is generally 70-100 J, asynchronous is generally 200-360 J (for adults: first shock 200 J, second shock 200-300 J, third shock 360 J; for biphasic: 150 J—150 J—200 J).
6. Charge: Place the electrode plates in appropriate positions (right edge of the sternum at the second intercostal space—apex of the heart; left anterior axillary line at the fifth intercostal space—base of the heart), ensuring the distance between the two electrode plates is greater than 10 cm; loudly instruct other personnel to leave the patient and bed.
7. Press the discharge buttons under both electrode plates simultaneously (the electrodes should be pressed firmly with a force of 10-12 kg).
8. Observe changes in the patient’s ECG.
9. If ventricular fibrillation/tachycardia (pulseless ventricular tachycardia) persists, immediately recharge and repeat the steps.
10. After the operation, return the energy switch to zero.
11. Clean the skin and place the patient appropriately.
12. Monitor heart rate and rhythm, and administer medications as prescribed.
13. Record.
14. Final processing.
Precautions
1. Timely check the defibrillator’s performance and charge it promptly.
2. Conductive gel should be applied evenly to prevent skin burns.
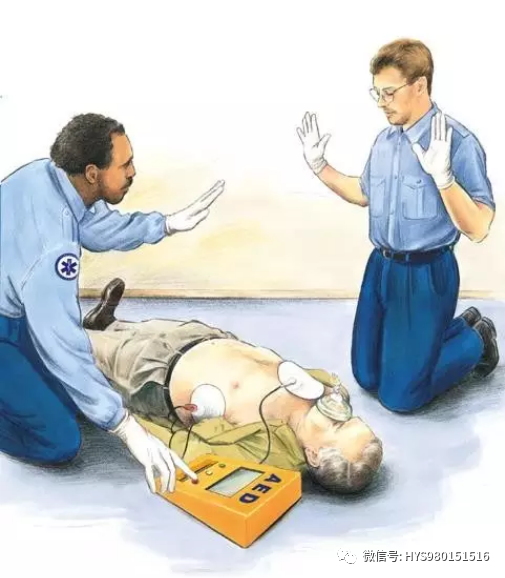
3. During discharge defibrillation, ensure insulation between the patient and other people or objects.
4. Energy selection for children: first shock 2 J/kg, second shock 2-4 J/kg, third shock 4 J/kg.
5. For ventricular tachycardia with distinguishable QRS and T waves, synchronized cardioversion should be performed; if indistinguishable, use asynchronous defibrillation.
6. For the same indications, synchronized cardioversion typically starts with a slightly lower energy as prescribed; the “synchronize” button should be pressed before selecting energy.
Maintenance of the Defibrillator
1. Clean the recorder’s print head
If the ECG strip prints too faintly or inconsistently, clean the print head with a cotton ball soaked in alcohol to remove any residual paper debris.
2. Maintain the battery
The defibrillator can be powered by AC or battery. Once the battery is inserted into the defibrillator, it should be charged for 24 hours to ensure it reaches full capacity. It should be connected to an AC power source to ensure it is charged adequately after each use; otherwise, it will reduce the battery’s capacity and lifespan. If the defibrillator is stored without AC power for more than a month, it should be charged for 48 hours before being removed from the device and stored in a cool, dry place, but not below zero degrees Celsius. The battery should be charged for at least 24 hours every six months while in storage to ensure it does not discharge completely. When the battery is removed from the device, it should be clearly marked that the device requires AC power to operate.
Prolonged periods without charging the battery can cause permanent damage. Therefore, the battery capacity should be checked at least once every six months. A sealed lead-acid new battery can provide at least 2.5 hours of monitoring time, and if it cannot provide the minimum of 2.5 hours of monitoring time, or if the battery cannot provide a 10-minute “low battery voltage” warning time, it needs to be replaced.
3. Clean the exterior surfaces
Keep the exterior of the device free of dust, thoroughly remove any conductive gel from the defibrillator electrodes, and clean the exterior with non-corrosive detergents like soapy water or chlorine bleach, ensuring no liquid enters the device’s interior. Avoid strong solvents like acetone or acetone-based compounds, as the display screen is prone to cracking, and be very careful while cleaning. Do not steam sterilize or fumigate the monitoring leads and defibrillator electrodes.
Personal opinions, for reference only
Source: Good Doctor
Copyright belongs to the original author. If there is any infringement, please contact us for modification or deletion, contact number: 0731-85054048
Recommended Reading
Join Group: Various specialized nursing WeChat groups, hurry and join
Submission: Original articles related to nursing are welcome for submission
Video Account: Nursing tips and expert live broadcasts
Follow: WeChat public account categorized by nursing departments
Buy Books: Nursing books, click “Read Original” below to purchase