Cite this chapter
Large, T., Krambeck, A.E. (2020). Holmium Laser Enucleation of the Prostate (HoLEP). In: Best, S., Nakada, S. (eds) Minimally Invasive Urology. Springer, Cham. https://doi.org/10.1007/978-3-030-23993-0_15
Holmium Laser Enucleation of the Prostate (HoLEP) is a transurethral procedure aimed at removing obstructive adenomatous tissue from the prostate to improve urinary function in patients with benign prostatic hyperplasia (LUTS/BPH). This surgery has been performed in the United States since 1998, and multiple randomized controlled trials have shown its lasting effects on LUTS improvement in men with BPH, independent of bladder health status, prostate size, and anticoagulation status. However, critics of HoLEP point to its high incidence of urinary incontinence and retrograde ejaculation, as well as its steep learning curve. With appropriate consultation and multimodal approaches (such as self-directed learning, video review, and guided procedures), the learning curve can be shortened and the mastery of the procedure expedited. The latest chapter reviews the current literature, step-by-step process, necessary equipment, and related complications.TURP is a common surgical method for treating BPH, but there are various alternative therapies, including PUL, water vapor thermal therapy, etc.Various therapies aim to improve LUTS and reduce side effects.For large gland BPH, laser enucleation and laparoscopic/robotic surgeries have replaced OP.HoLEP is the most rigorously studied surgical technique, offering profound and lasting improvements in urinary function and LUTS, and is considered the gold standard for BPH surgery.
As the age of LUTS/BPH patients increases and comorbidities multiply, the demand for minimally invasive BPH surgeries has risen. To reduce the morbidity associated with TURP/OP, laser therapies such as HoLEP, ThuLEP, and PVP have been developed for coagulating, vaporizing, and cutting prostate tissue. Advances in laser technology have enabled prostate lobe enucleation and tissue removal, with the holmium laser being the most widely accepted.HoLEP has become a common surgical therapy for LUTS/BPH, capable of handling complex cases.The procedure utilizes holmium laser cutting, enucleation of adenomas, and evacuation of excised tissue without the need for incisions.A substantial body of research confirms that HoLEP is safe and effective for BPH patients, regardless of gland size, even in those with bleeding tendencies or undergoing anticoagulation therapy.Compared to TURP and OP, HoLEP has a lower incidence of complications.Long-term studies show sustained relief of BPH symptoms 4-10 years postoperatively, with a very low retreatment rate.
HoLEP, with its excellent tissue reduction capability, can reduce prostate volume and prostate-specific antigen by 60-90%. It can also be performed as an outpatient procedure, with catheter removal within 24 hours post-surgery. Compared to other ablative surgeries, HoLEP has advantages such as actual tissue removal for pathological examination, significant volume reduction, and lasting effects, all while maintaining a low incidence of complications.HoLEP uses laser surgery with saline irrigation to prevent dilutional hyponatremia.The laser can coagulate, allowing for precise control of bleeding.Patients without bleeding typically require almost no transfusion postoperatively.Radical prostatectomy can be performed after HoLEP, addressing bladder, ureter, and kidney stones, with minimal impact on erectile function.HoLEP is more cost-effective than TURP and OP due to shorter hospital stays and fewer auxiliary interventions.Learning HoLEP requires a steep learning curve, and it is recommended to use teaching, video, and navigation training methods.This article provides the latest guidelines for HoLEP, including equipment, procedures, postoperative recovery, and complications.
Current Equipment Used for HoLEP
Equipment List
- 1. 120W dual-footpedal holmium laser device
- 2. 550 μm Moses (Lumenis, Santa Clara, California) or 1000 μm SlimLine side-firing laser fiber (Lumenis)
- 3. 30-degree cystoscope lens
- 4. Video tower and freely swinging camera
- 5. Physiological saline irrigation
- 6. Continuous flow resectoscope (26–28 F) with modified inner sheath and laser stabilizer
- 7. 7 F stabilizing catheter
- 8. Van Buren urethral sound
- 9. Ellik evacuator
- 10. Offset rigid nephroscope with bridge connector
- 11. 5 mm tissue morcellator
- 12. Crocodile forceps
- 13. 22 F three-way catheter with Mandarin guide
- 14. Otis urethrotome
The holmium laser is a pulsed solid-state laser with a wavelength of 2140 nm. Unlike other available laser systems, the holmium laser is a contact laser, with a penetration depth of only 0.4 mm in prostate tissue. The laser energy is highly absorbed by water (absorption peak: 1.940 nm), with water comprising 60-70% of the prostate [ 25 ]. This water absorption generates an energy density that can heat prostate tissue to over 100 °C [ 27]. The thermal energy produced by the holmium laser allows for precise tissue cutting while minimizing carbonization and plane blurring. Using newer laser devices like the Lumenis 120H™, pulse width modulation can be performed, which, when set to a narrow pulse width, can further enhance the precision and anatomical capability of the laser. Additionally, the acoustic pulses generated by the laser can disrupt the loose tissue connections between the true prostate and the prostatic adenoma, facilitating the removal of obstructive tissue. Finally, when the laser is set to a wide pulse width and positioned on bleeding vessels, it can distribute heat that leads to vessel coagulation to a depth of 2-3 mm without cutting the surgical capsule [ 27]. The latest American Urological Association (AUA) LUTS/BPH surgical guidelines recognize the good hemostatic properties of the holmium laser. HoLEP is recommended as the procedure of choice for patients requiring anticoagulation (AC), antiplatelet (AP), or dual AC/AP therapy [ 2 ].The holmium laser is a versatile laser that can be used not only for tissue cutting (e.g., treating urethral strictures) and ablation (treating upper urinary tract tumors) but also for lithotripsy [ 3,28,29 ]. Ureteroscopic laser lithotripsy has become the most common surgical method for treating kidney stones [ 30 ]. Urologists can generally use holmium technology. However, to perform HoLEP effectively, the use of high-power lasers is recommended. Studies show that using a 30 W laser can achieve comparable intraoperative and postoperative outcomes for HoLEP, but generally, the dual-energy Lumenis120H™ or 100 W Versapulse holmium laser (Lumenis) is the best choice (Figure 15.1). The recent application of Moses laser technology developed by Lumenis shows further improvements in hemostasis and enucleation efficiency; however, publications are still lacking.
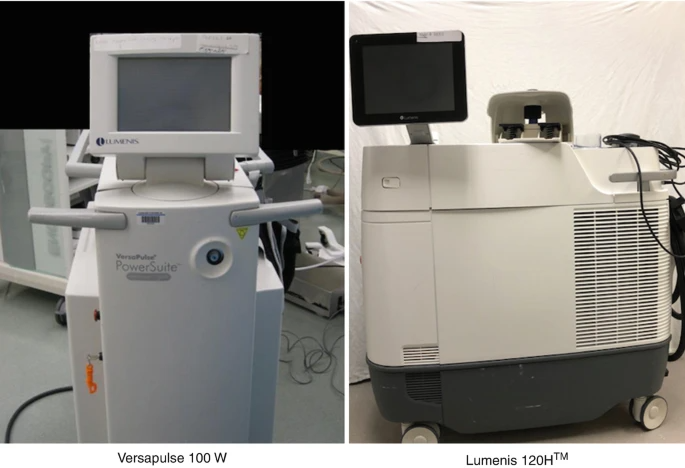
100 W Versapulse holmium laser and Lumenis 120H used for performing HoLEPThe holmium laser energy can be transmitted through flexible quartz fibers of various diameters (100 to 1000 μm). The ability to use multiple sizes of fibers allows the holmium laser to be used not only with cystoscopes but also with rigid and flexible ureteroscopes. Generally, larger laser fibers are preferred when performing HoLEP, such as the 550 or 1000 μm SlimLine side-firing (Figure15.2) and the recently developed 550 μm Moses fiber.Various companies provide both disposable and reusable quartz laser fibers. Unlike other laser surgical techniques, HoLEP can sterilize and reuse holmium laser fibers up to 20-30 times, thus reducing equipment costs [ 25 , 31]. During HoLEP, the protective coating of the laser fiber is typically stripped back (5-6 cm) and placed through a 7 Fr stabilizing catheter (Spencer Cook, Indiana). The catheter is secured in place through a Luer-Lok injection port (Baxter, Deerfield, IL). When using a 1000 μm fiber, the tip of the stabilizing catheter must be cut to allow the larger diameter fiber to pass (Figure15.3).
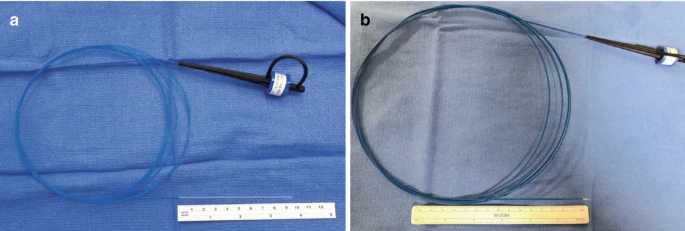
550 μm ( a ) and 1000 μm ( b ) quartz laser fibers used for performing HoLEP
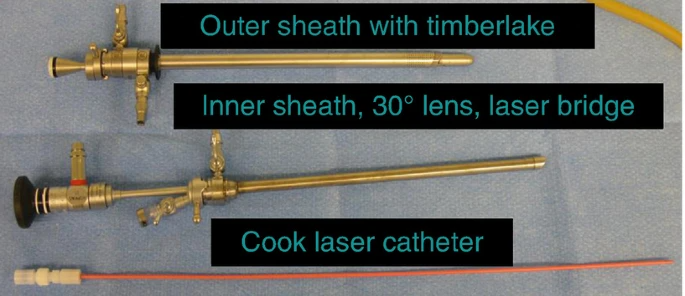
The laser aiming device and protective laser sheath after disassembly. The equipment shown is the Storz 28 Fr kit, consisting of a 28 Fr outer sheath, an inner sheath with a stabilizing ring, and a 30-degree telescope lens. The laser sheath passes through the working element of the endoscope and is secured in place by the stabilizing ring.Two different companies produce laser aiming devices that can be used for performing HoLEP. Olympus (Hamburg, Germany) produces 27 Fr, while Storz (Tuttlingen, Germany) produces 26 and 28 Fr continuous flow resectoscopes, with dedicated inner sheaths containing laser channels (Olympus) and laser rings (Storz) to stabilize and focus the laser fiber during enucleation (see Figure15.3).Regardless of the range of lasers used for performing HoLEP, a 30-degree lens is required for adequate visualization of the prostate and laser tip. Given the extreme hand movements required for performing HoLEP, it is recommended to use endoscopic cameras with rotating bases. High-definition video systems, such as those provided by Stryker (Kalamazoo, Michigan) and Olympus (Hamburg, Germany), can improve visualization of the surgical plane between the true prostate and adenoma, facilitating enucleation and enhancing HoLEP efficiency. Since HoLEP is a laser-based therapy, physiological saline irrigation is used in all cases.Once the prostate is excised, a tissue morcellator must be used to remove the tissue. Before introducing the morcellator, the internal working elements of the laser endoscope are removed, leaving only the outer sheath that passes through the length of the urethra. The morcellator is then introduced using a 26 Fr nephroscope with a 5 mm working channel and an adapter bridge to visualize the bladder tissue morcellation (Figure15.4a).There are two commercially available morcellators: Piranha (Richard Wolf, Knittlingen, Germany) and Versacut (Lumenis). The morcellator consists of a mobile unit with reciprocating blades and a control box with a suction pump, operated by a foot pedal (Figure15.4b).No continuous flow irrigation is used during morcellation. Due to the powerful suction potential of the morcellator, a third inflow line is connected to the outflow channel. The Piranha system uses two pedals solely for suction and suction/morcellation, while Versacut combines both functions into one pedal, with partial depression starting suction and full depression causing the morcellator blades to cycle with suction. Comparisons of the two morcellators show excellent tissue removal efficacy; however, in a comparative trial, the Piranha morcellator demonstrated higher efficiency and fewer complications compared to Versacut [ 32]. After all tissue is removed, a 22 Fr three-way catheter filled with 60 ml is placed in the balloon for an average of 15 hours, with removal occurring the next morning without any complications, initiating a trial of voiding.
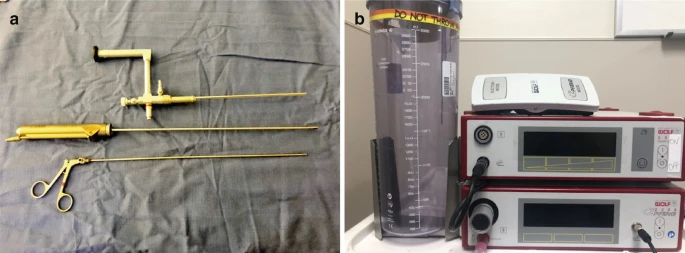
( a ) The long nephroscope shown here has a 5 mm working channel and length adapter bridge, allowing the morcellator and grasping forceps to pass through. The grasping forceps can be used for removing small fragments rather than morcellation. The Piranha morcellator is positioned between the grasping forceps and nephroscope. ( b ) The morcellator has a suction device that removes prostate tissue while morcellating.
HoLEP: Step by Step
Preoperative Assessment
Before undergoing HoLEP, patients should undergo an appropriate preoperative assessment. While the evaluation may be tailored to the individual patient, it should generally include a patient history, AUA symptom score (or appropriate validated metrics), and post-void residual urine flow. Laboratory evaluations should include a complete blood count (CBC), creatinine electrolytes, and serum prostate-specific antigen (PSA). Although evidence suggests that HoLEP can be offered to patients with LUTS/BPH, regardless of gland size, it is advised to perform a transrectal ultrasound (TRUS) volume study on patients without any prior imaging (CT or MRI). Once the surgeon masters HoLEP, their operative time is expected to reach 30-60, 90-120, and for prostates smaller than 80 g, 80-150 g, and larger than 150 g, respectively exceeding 120 minutes. Generally, patients with a history of prior transurethral surgery and/or a history of urethral stricture or risk factors should undergo preoperative cystoscopy. Finally, if the patient has severe urinary urgency, frequency, incontinence, or other neurological comorbidities, a complete urodynamic study may help distinguish significant detrusor instability from bladder outlet obstruction.As with any surgical procedure, informed consent is required. HoLEP is associated with a high incidence of transient urinary incontinence (1.3-44%), while the incidence of persistent incontinence lasting over 3 months is less than 2-5% of patients [ 33 , 34]. It has been noted that 80% to 100% of patients experience retrograde ejaculation, but erectile function is preserved after HoLEP [ 19]. Although the risk of clinically significant bleeding is less than 1% [ 4], the possibility of transfusion should be discussed even in those with anticoagulation or bleeding tendencies [ 17]. Morcellation injuries can have significant consequences; however, a recent study indicated that the Piranha system had zero morcellation injuries.35], Krambeck et al. reported similar findings. In over 1000 HoLEPs, only one morcellation injury required open repair [ 36].
Surgical Preparation
Patients are positioned in the dorsal lithotomy position. Spinal or general anesthesia is suitable for patients undergoing HoLEP, using a laryngeal mask airway (LMA) or endotracheal intubation. The LMA combines anesthetics, benzodiazepines, and propofol to provide adequate anesthesia with rapid induction and gentle awakening postoperatively. The urethra is dilated to 30–32 Fr to accommodate the outer sheath of the continuous flow laser resectoscope. After instilling additional lubricant transurethrally with a Toomey syringe, the outer sheath is introduced with a Timberlake obturator. The laser resectoscope with a 7 Fr laser stabilizing catheter is placed through the outer sheath and secured to it. Various laser fibers can be used, including 550 or 1000 μm single-use, reusable fibers, or Moses fibers, which can pass through a 7 Fr laser sheath. Due to the high energy used during HoLEP, it is expected that the laser will break, so the protective coating on the laser fiber is usually stripped back 5-6 cm. The preferred irrigation fluid is saline, which enters through a Y-connector attached to the inflow port of two 3 L saline bags.
Posterior Plane Anatomy and Creation Assessment
Once the resectoscope is firmly connected to the outer continuous flow sheath, the patient’s anatomy is assessed. Ideally, the surgeon should note any changes in the prostate structure, such as a large median lobe, high or tight bladder neck, or defects from prior BPH surgeries. In some cases, the patient’s body habitus or prostate may be too large to be disrupted with the resectoscope at the bladder neck. In such cases, a perineal urethrostomy can be safely performed prior to HoLEP and closed at the end of the case. These patients should retain a Foley catheter for one week.It is good practice to observe the ureteral orifice (UO), but it should not prolong the case time. Typically, the UO will be obscured by the intravesical projection of the prostate, especially in cases of larger median lobes. Assessing whether the patient has bilobed or trilobed hypertrophy will determine whether a single 6 o’clock or two incisions (5 o’clock and 7 o’clock) are needed for the initial groove. In cases of two incisions, the median lobe should be excised after connecting the grooves at 5 o’clock and 7 o’clock. Removing the median lobe will create more space for the prostatic fossa and better define the surgical capsule, which will expedite subsequent lateral lobe anatomy (Figure15.5).
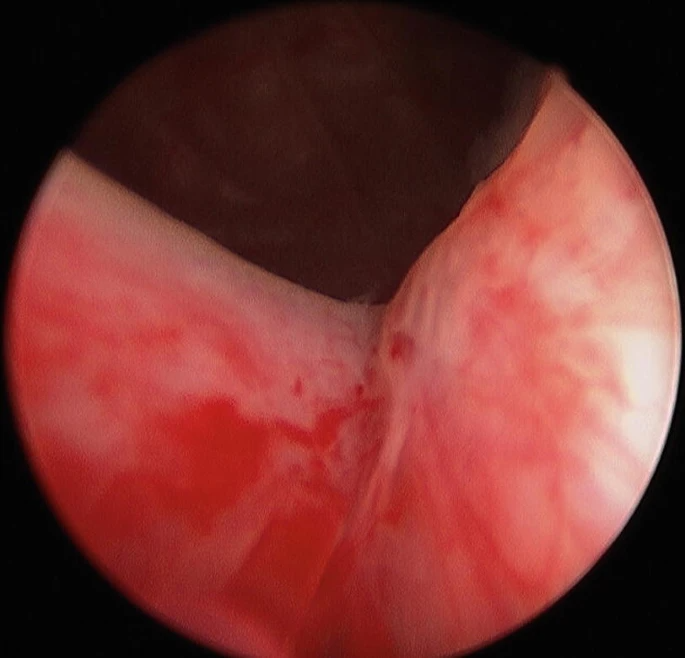
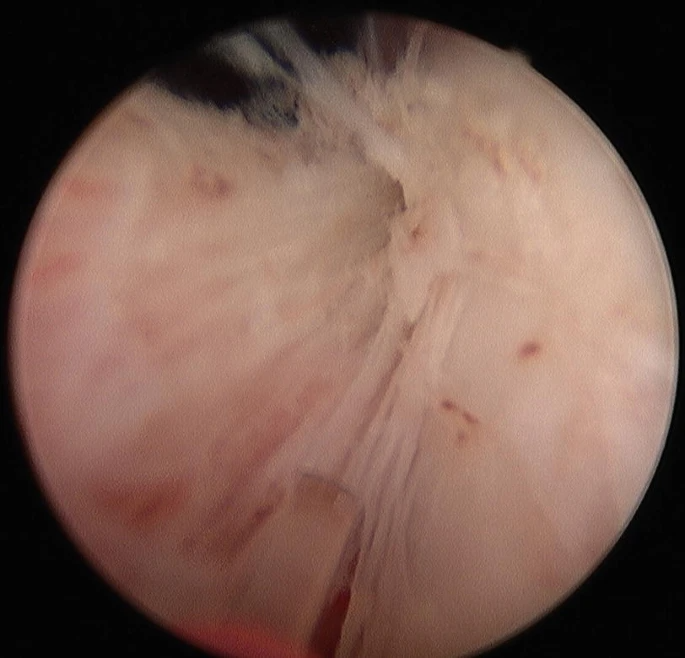
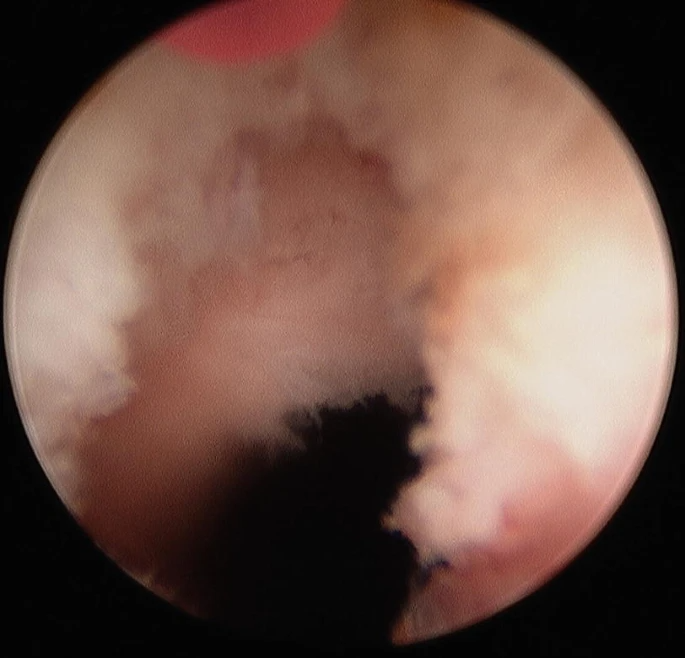
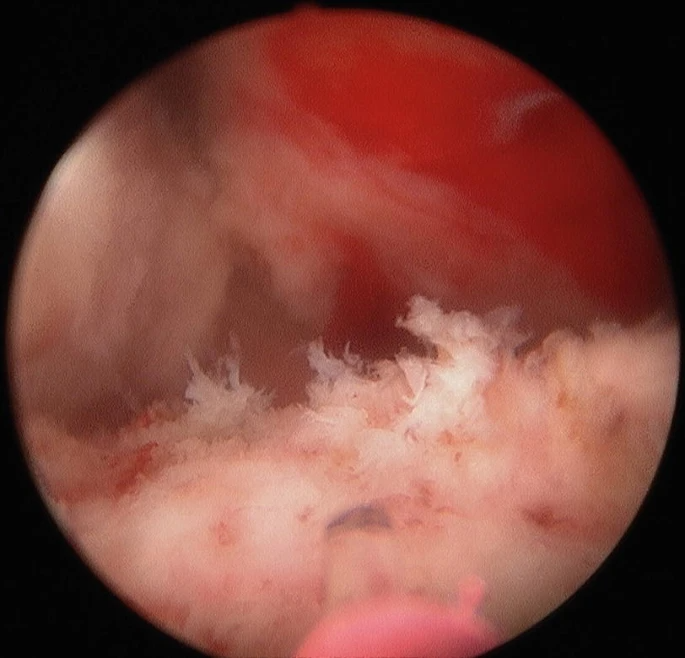
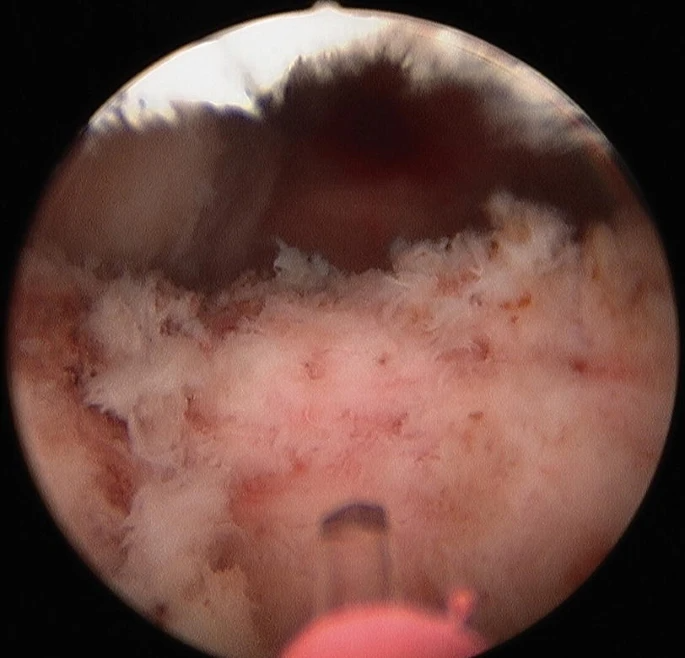
Initial posterior incision view, beginning from the 6 o’clock or 5 o’clock position and 7 o’clock position, depending on the presence of the median lobeThe standard laser settings for the initial portion of HoLEP are set to 2 joules (J) and 40 hertz (Hz). The initial groove should be deepened until the capsule is reached, which can be most easily recognized by the horizontal vesicular vessels or circular fibers near the bladder neck (Figures15.6 and15.7).Surgeons experienced in prostate ablation should be familiar with this depth near the bladder neck. During the initial incision, gently moving the tip of the resectoscope can widen the initial groove to help identify the capsule. Once the grooves at 5 o’clock and 7 o’clock are connected laterally, the adenoma should be lifted with the tip of the resectoscope while using thermal laser energy to release the attachments between the median lobe and the prostatic capsule, thereby disrupting the median lobe. The correct plane should present a spider web appearance, with the adenoma separated from the prostatic capsule (Figure15.8).Once the posterior attachments between the median lobe and the surgical capsule are released, the median lobe will be pushed into the bladder cavity and still tethered by the mucosal tissue at the bladder neck. Separating the adenoma from the bladder neck requires precise laser application near the bladder neck to avoid dissecting the back of the median lobe. Tension must be applied to the median lobe to cut the mucosal attachments. Positioning the UO at this step is crucial, as the resectoscope may recoil into the UO, potentially causing laser injury to the ureter.
Round fibers near the bladder neck
A spider web appearance of the adenoma separated from the prostatic capsule
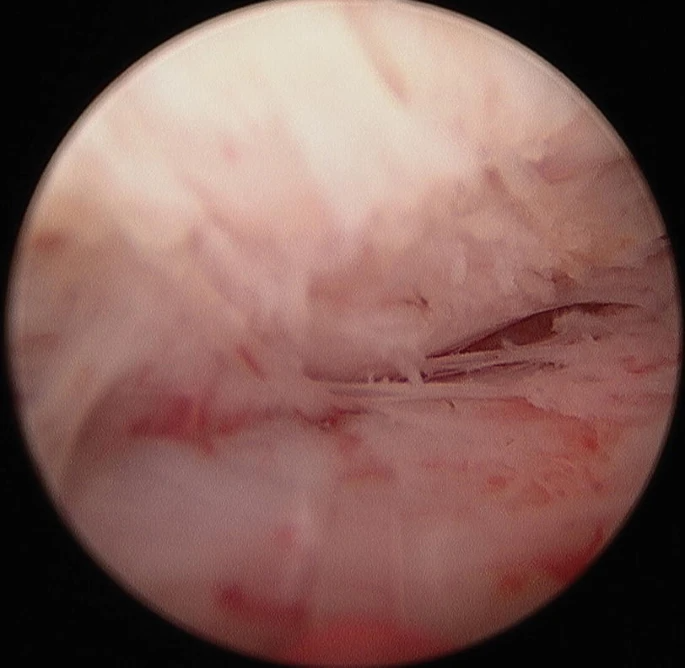
Anatomical anterior plane traversing from 10 o’clock to 2 o’clock through the bladder mucosa to allow the resectoscope to enter the bladder cavity. Note the laser fiber and capsule above and the adenoma below.If the median lobe is small or of moderate size, separate excision is not necessary. A single posterior groove can be made, and any posterior tissue can be enucleated along with the lateral lobe tissue.
Lateral Lobe Enucleation
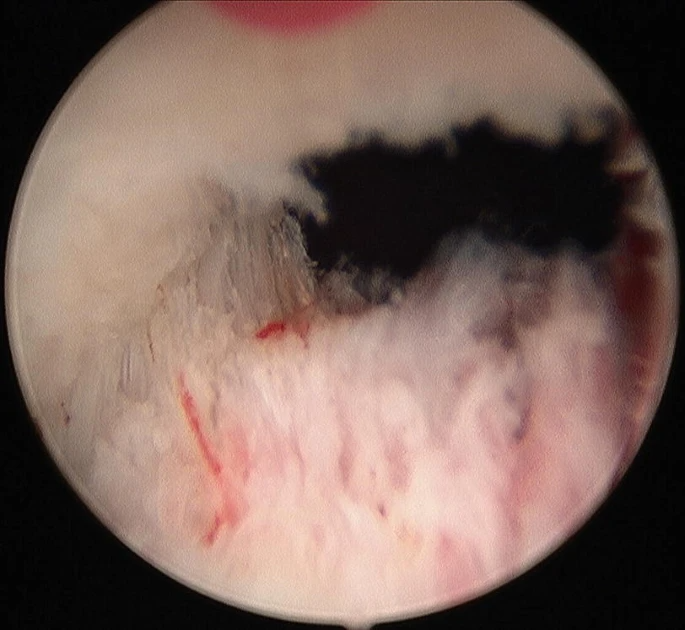
After completing median lobe enucleation or a single posterior incision, attention turns to the lateral lobe tissue. The lateral lobes are enucleated separately, starting from the initial groove located near the proximal and lateral side of the seminal colliculus. A short horizontal incision is made to form a mucosal surface incision, just enough to allow the tip of the resectoscope to enter. The laser energy should then be reduced to 2 J and 20 Hz to minimize potential damage to the external sphincter complex from direct iatrogenic laser injury or thermal diffusion. Combining blunt dissection with laser, gently rotating the endoscope around the apex of the adenoma until the endoscope is positioned at the 2 o’clock position, with the capsule above the endoscope and the adenoma below. It is important to extend the dissected anterior plane beyond the midline to facilitate the excision of the second lobe. Once the anterior plane is moved away from the sphincter complex, the laser energy is increased to 2 J and 40 Hz. The resectoscope then applies downward pressure on the adenoma, using the laser to separate any capsular attachments and cauterize any penetrating vessels, moving the dissected anterior plane towards the bladder neck.When pushing the anterior plane towards the bladder neck, it is crucial to maintain a wide dissected plane from the 10 o’clock to 2 o’clock position. Once the vertical bladder neck fibers are cut to expose the bladder cavity, the bladder neck should be normalized before entering the true prostatic cavity to cut the anterior commissure (see Figure 1). Once the anterior plane is moved away from the sphincter complex, the laser energy is increased to 2 J and 40 Hz. The resectoscope then applies downward pressure on the adenoma, using the laser to separate any capsular attachments and cauterize any penetrating vessels, moving the dissected anterior plane towards the bladder neck. When pushing the anterior plane towards the bladder neck, it is crucial to maintain a wide dissected plane from the 10 o’clock to 2 o’clock position. Once the vertical bladder neck fibers are cut to expose the bladder cavity, the bladder neck should be normalized before entering the true prostatic cavity to cut the anterior commissure (see Figure 1).Once the anterior plane is moved away from the sphincter complex, the laser energy is increased to 2 J and 40 Hz. The resectoscope then applies downward pressure on the adenoma, using the laser to separate any capsular attachments and cauterize any penetrating vessels, moving the dissected anterior plane towards the bladder neck. When pushing the anterior plane towards the bladder neck, it is crucial to maintain a wide dissected plane from the 10 o’clock to 2 o’clock position. Once the vertical bladder neck fibers are cut to expose the bladder cavity, the bladder neck should be normalized before entering the true prostatic cavity to cut the anterior commissure (see Figure 1).Once the anterior plane is moved away from the sphincter complex, the laser energy is increased to 2 J and 40 Hz. The resectoscope then applies downward pressure on the adenoma, using the laser to separate any capsular attachments and cauterize any penetrating vessels, moving the dissected anterior plane towards the bladder neck. When pushing the anterior plane towards the bladder neck, it is crucial to maintain a wide dissected plane from the 10 o’clock to 2 o’clock position. Once the vertical bladder neck fibers are cut to expose the bladder cavity, the bladder neck should be normalized before entering the true prostatic cavity to cut the anterior commissure (see Figure 1).By repositioning the scope in the prostatic urethra and splitting the anterior commissure at the 12 o’clock position, the two lobes are separated (Figure15.9).The incision extends from the bladder neck to the apex of the bladder. By cutting the anterior commissure, the anterior plane should be visible posteriorly, providing visual assistance to avoid excessive dissection distally, which could potentially affect or damage the sphincter complex.
Separating the two lobes by repositioning the scope in the prostatic urethra and splitting the anterior commissure at the 12 o’clock position.After separating the lateral lobes, the mucosal tissue strips surrounding the adenoma need to be separated from the sphincter. Using a circumferential technique, the endoscope is inverted at the 12 o’clock position of the bladder neck, then the resectoscope rotates around the outer edge of the adenoma to the 6 o’clock position, ensuring that the mucosal strip is on one side of the endoscope and the sphincter on the other. Pulling the endoscope forward allows the strip to fall in front, cutting transversely at a rate of 2 J and 20 Hz, avoiding sphincter injury.After separating the mucosal strip, connect the lateral and posterior planes, enucleating the remainder of the lobe. Once the adenoma is detached, push the endoscope tip into the bladder, cutting the attachments at the bladder neck, releasing the adenoma into the bladder. The same dissection is performed on the contralateral lobe.
View of the resected lateral lobe pushed into the bladder.“Hemostasis must be achieved immediately after resection. While the holmium laser is effective at sealing small vessels, thorough hemostasis requires additional time to identify and control small bleeding points. Improved visibility aids in successful morcellation.”
View of the prostatic fossa opened.After resection, the excised tissue is removed using a tissue morcellator. The internal components of the laser endoscope are replaced with a 26 Fr nephroscope, equipped with a 5 mm working channel. The morcellator enters through this channel. The morcellator uses a combination of suction and cutting blades to remove tissue. Ensure that a large volume of fluid flows through the endoscope to prevent suction from causing rapid bladder contraction and damaging the morcellator. After most of the tissue is removed, the prostatic fossa should undergo a final inspection to ensure no small adenoma fragments are obscured.After placing a 22 Fr three-way catheter on the Mandarin catheter guide, 60 ml of fluid should be injected into the balloon. Depending on the presence of hematuria, continuous bladder irrigation may be required. To enhance hemostasis at the bladder neck, catheter tension may be applied for a short period. The catheter should remain in place overnight and be removed the next day. After catheter removal, the patient should be able to void normally and check for residual urine volume to prevent urinary retention.
Predicting Postoperative Outcomes
HoLEP completely excises prostatic adenoma, with sustained symptom relief postoperatively, superior to other urethral surgeries. With an average follow-up of 43.5 months, the Qmax is 21.9 ml/s, and the retreatment rate is 4.3%. PSA and prostate volume significantly decrease. The longest follow-up shows a retreatment rate of 0-5.4%.Over 1000 HoLEP surgeries have been performed, with an average preoperative prostate weight of 99.3 g, AUA score of 20.3, and Qmax of 8.4 cc/s. Complications are minimal, occurring in 2.3% of patients. The average follow-up is 287 days. The latest AUA score is 5.3, with a Qmax of 22.7 cc/s. Three patients experienced urinary retention, all with bladder tension disorders. One patient required a second surgery due to rebleeding. The incidence of urethral stricture and bladder neck contracture is less than 2%. Elmansy et al. reported a 10-year stricture rate of 1.6% and bladder neck contracture of 0.8%.Postoperative incontinence is the most troublesome side effect of HoLEP surgery, with patients potentially experiencing urgency and mixed incontinence. Approximately 30% of patients have symptoms one month postoperatively, reducing to 5% at three months. These symptoms respond well to treatment and exercise, and most are self-limiting. In long-term follow-up, the overall incontinence rate is less than 5%. Diabetes, large prostate, and significant PSA reductions are predictive factors for postoperative stress urinary incontinence. Other complications include hematuria, clot retention, bladder-urethra injury, and complications from general anesthesia.
|
Complication |
Incidence (%) |
|---|---|
|
Bladder perforation |
0.1 |
|
Clinically significant hematuria |
0.7 |
|
Urethral stricture |
2.3 |
|
Bladder neck contracture |
1.5 |
|
Severe short-term stress urinary incontinence |
12.5 |
|
Severe short-term urgency urinary incontinence |
11.5 |
|
Severe long-term stress urinary incontinence |
1.8 |
|
Severe long-term urgency urinary incontinence |
1.5 |
|
Re-excision due to adenoma regrowth |
0.1 |
|
Persistent urinary retention |
0.03 |
-
a A total of three patients, two of whom had atonic bladder and one who developed neurogenic bladder after HoLEP due to spinal cord injury.
HoLEP has limited impact on sexual function, similar to TURP and OP. There is no difference in IIEF scores at 2 years postoperatively. Patients should be informed of the risk of retrograde ejaculation, with over 75% experiencing retrograde ejaculation 6 years later, affecting sexual satisfaction.
HoLEP is a safe, effective, and minimally invasive surgery for BPH. It is durable and rarely requires subsequent repairs. Compared to TURP, HoLEP has a lower incidence of complications, removes a large amount of tissue, has a steep learning curve, but once mastered, is the gold standard for treating LUTS/BPH.